|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
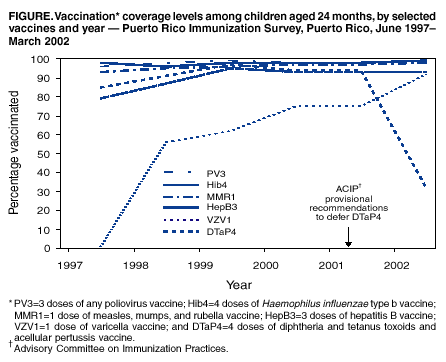
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Impact of Vaccine Shortage on Diphtheria and Tetanus Toxoids and Acellular Pertussis Vaccine Coverage Rates Among Children Aged 24 Months --- Puerto Rico, 2002In March 2001, because of a temporary shortage of diphtheria and tetanus toxoids and acellular pertussis (DTaP) vaccine, CDC recommended that providers whose supply of DTaP was inadequate defer administration of the fourth dose of the vaccine (DTaP4) (1,2). CDC recommended that providers recall for vaccination all children who had missed DTaP4 when adequate supplies of DTaP become available (2). On May 4, 2001, the Puerto Rico Department of Health (PRDOH) directed all regional vaccine coordinators to implement the deferment of DTaP4. Vaccine coordinators and their staffs visited all providers that receive vaccines from the Puerto Rico Immunization Program (PRIP), a majority of which are private providers serving indigent patients, to instruct them to defer administering DTaP4 while continuing the rest of the schedule. The recommendations also were implemented in special vaccination clinics for children operated by PRIP. In March 2002, to assess the impact of the vaccine shortage on vaccination coverage levels among children in Puerto Rico, PRDOH conducted a survey of vaccination coverage levels among children aged 24 months. This report summarizes the results of the survey, which indicate that the DTaP4 coverage level was substantially lower in 2002 than in 2001. Now that supplies have returned to normal levels, the routine schedule for DTaP vaccination of children should be resumed, and data from national and local immunization surveys will be used to monitor post-shortage vaccination levels. The Puerto Rico Immunization Survey (PRIS) is an annual household survey that measures vaccination coverage levels among children aged 24 months. For the 2002 survey, PRDOH selected a random sample of 1,080 children out of all 4,818 children born in Puerto Rico during March 2000. During March 2002, PRDOH attempted to locate and interview the parents or guardians of these 1,080 children to verify the children's vaccination status. Of the 1,080 children, 70 (6.5%) had left Puerto Rico or could not be traced. Survey responses were obtained for 990 of the remaining 1,010 children, for a response rate of 98.0%. These figures were similar to those obtained in 2001, when 78 (7.3%) of 1,080 children could not be located and the response rate was 96.9%. If a parent-held vaccination card was not available as proof of vaccination, the interviewers requested consent to visit the child's health-care provider to verify the child's vaccination history. Vaccinations were counted only if they were documented on the vaccination card or reported by a health-care provider. Children's coverage levels for routinely recommended vaccines in the 2002 PRIS were compared with 2001 results. DTaP3 vaccination coverage levels among children aged 24 months in 2002 (99.1%) showed little change from 2001 (98.3%). However, the coverage level for DTaP4 was substantially lower in 2002 (31.8%) than in 2001 (95.8%). Coverage levels with 3 doses of any poliovirus vaccine (PV3), 4 doses of Haemophilus influenzae type b vaccine (Hib4), 1 dose of measles, mumps, and rubella vaccine (1MMR), 3 doses of hepatitis B vaccine (HepB3), and 1 dose of varicella vaccine were nearly identical in 2002 and 2001 (Figure). However, consistent with the decline in DTaP4 coverage level, coverage with the 4:3:1:3 (DTaP4, PV3, 1MMR, and 3 doses of Hib) and the 4:3:1:3:3 (4:3:1:3 series and HepB3) vaccine series both were substantially lower in 2002 (31.2% and 30.9%, respectively) than in 2001 (94.1% and 93.8%, respectively). Reported by: A Rivera, MD, JC Orengo, MD, AL Rivera, C Rodríguez, MS, E Calderón, J Rullán, MD, Puerto Rico Dept of Health. H Yusuf, MBBS, L Rodewald, MD, Immunization Svcs Div; L Barker, PhD, Data Management Div, National Immunization Program; F Alvarado-Ramy, MD, Div of Applied Public Health Training, Epidemiology Program Office, CDC. Editorial Note:The decrease in DTaP4 coverage among children in Puerto Rico might herald similar findings for other parts of the United States. PRDOH implemented the recommendations for postponing DTaP4 in May 2001, during the period when children in the cohort reviewed in the 2002 PRIS were due to receive DTaP4. Consistent with the revised policy, PRIS detected a substantial decline in DTaP4 coverage among these children; coverage levels for the first 3 doses of DTaP and for other vaccines did not change. The annual National Immunization Survey (NIS) estimates coverage levels for routinely recommended vaccines among children aged 19--35 months in all 50 states and in 28 large urban areas (3,4). Because children included in NIS are slightly older than those included in PRIS and the larger NIS sample size results in a 6-month delay between data collection and reporting of results, declines in DTaP4 coverage levels in other parts of the United States monitored by NIS might not be recorded until late 2002 at the earliest. The maximum impact of the shortage might not be recorded until the second half of 2003, when all children in the cohort surveyed will be old enough to have received DTaP4 during the shortage period. The findings in this report are subject to at least two limitations. First, estimating vaccination coverage levels among children by using information in health-care providers' medical records is considered the most effective method for such assessments (5). For PRIS, the health-care provider was contacted only when the parent or guardian did not have the child's vaccination card. However, because vaccination cards are used officially in Puerto Rico to determine a child's vaccination needs, these records probably are accurate. Second, because PRIS samples children aged 24 months during the month of the survey, conclusions cannot be drawn about the duration of the decrease in DTaP4 coverage among these children. One measure used frequently to evaluate the performance of state and local vaccination programs that receive federal vaccination grants is their 4:3:1:3 vaccine series coverage levels; grantees are ranked annually according to these levels. Because of the temporary deferral of DTaP4 administration during the vaccine shortage, decreases in these coverage levels can be expected among children included in NIS during the next 3 years. Basing program performance results primarily on 4:3:1:3 series coverage might be misleading. The 4:3:1:3 coverage estimates are influenced most heavily by the vaccine with the lowest coverage level, usually DTaP4. Even with >90.0% coverage for other vaccines, using low DTaP4 coverage levels in the series might lead to the erroneous inference that coverage levels for all vaccines are low. Other elements (e.g., vaccination coverage levels for individual vaccines and incidence rates of vaccine-preventable diseases) might be better measures of overall program effectiveness. The DTaP supply problems were experienced disproportionately by the public sector and by private providers who depend on public supply, so the impact might vary among programs. On July 12, 2002, CDC published recommendations for returning to the full dosing schedule for DTaP now that supplies have returned to normal levels (6). Providers also were cautioned that for the next 2 months, supplies might not be adequate for the initiation of ambitious recall efforts (6). When adequate levels are reached, children who missed >1 dose of vaccine should be recalled and vaccinated, and catch-up vaccination levels should be monitored. PRIS can help monitor catch-up levels among children in Puerto Rico. State and local vaccination registries have the opportunity to facilitate catch-up vaccination in the rest of the United States. Through NIS, CDC will monitor the impact of vaccine shortages on vaccination coverage levels. References
|
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services. |
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 8/1/2002
|
|
|||||
|
HOME |
ABOUT MMWR |
MMWR SEARCH |
DOWNLOADS |
RSS
|
CONTACT
|
|||||
|
|
|||||
|
This page last reviewed 8/1/2002