|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
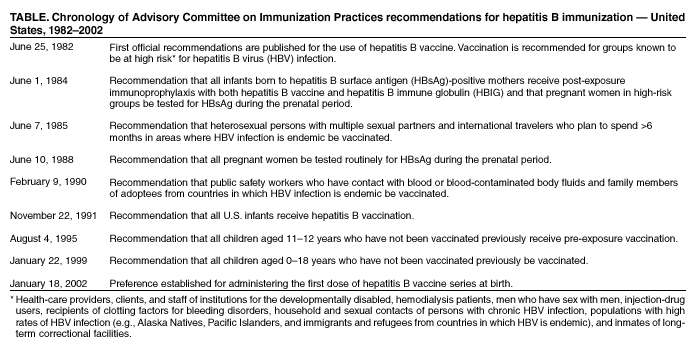
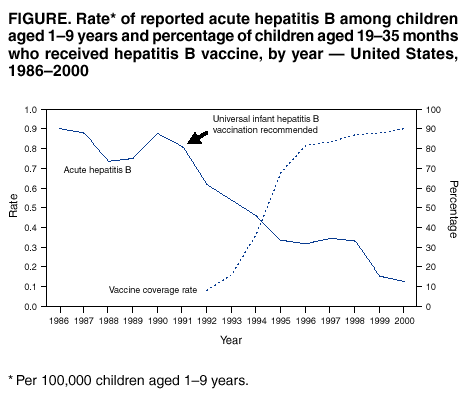
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Achievements in Public Health: Hepatitis B Vaccination --- United States, 1982--2002This year marks the 20th anniversary of the implementation in the United States of the world's first vaccine against hepatitis B virus (HBV). In addition to acute disease, persons infected with HBV are at risk for chronic HBV infection and severe morbidity and mortality from cirrhosis and hepatocellular carcinoma. Before 1982, an estimated 200,000--300,000 persons in the United States were infected annually with HBV, including approximately 20,000 children (1). No practical method of pre-exposure prophylaxis for HBV existed, and the only postexposure prophylaxis available was injection with hepatitis B immune globulin (HBIG). Since 1982, substantial progress has been made toward eliminating HBV transmission in children and reducing the risk for HBV infection in adults. During 1982--2002, an estimated 40 million infants and children and 30 million adults received hepatitis B vaccine. Because of vaccination and changes in risk-reduction behaviors among at-risk populations in response to the HIV/AIDS epidemic, the number of persons infected in the United States declined to an estimated 79,000 in 2001. To eliminate HBV transmission, high vaccine-coverage rates must be sustained among infants, children, and adolescents, and programs to vaccinate adults at high risk for HBV infection must be expanded. Evolving Vaccination StrategyIn June 1982, the Advisory Committee on Immunization Practices (ACIP) published the first official recommendations on the use of hepatitis B vaccine (Table) (2). ACIP recommended pre-exposure vaccination initially for groups with a high risk for HBV infection.* However, by 1989, it had become evident that members of these groups (e.g., men who have sex with men [MSM], injection-drug users [IDUs], and heterosexual persons with multiple partners) were not being vaccinated in substantial numbers. Some persons did not recognize the risk for HBV infection, and others did not know about the vaccine or were unable to purchase it. In addition, health-care providers often did not identify candidates for vaccination (CDC, unpublished data, 1987). Health-care workers comprised 80% of the approximately 2.5 million persons vaccinated during the 1980s; however, only 5% of acute hepatitis B cases occurred among health-care workers (3). In 1991, recognizing the difficulty of vaccinating high-risk adults and the substantial burden of HBV-related disease acquired from infections in childhood, ACIP recommended a comprehensive strategy to eliminate HBV transmission in the United States (4). The strategy focused on universal childhood vaccination, prevention of perinatal HBV transmission, vaccination of adolescents and adults in high-risk groups, and catch-up vaccinations for susceptible children in high-risk populations. In 1995, ACIP recommended the routine vaccination of all adolescents aged 11--12 years who had not been vaccinated previously (5), and in 1999, ACIP recommended that all unvaccinated children aged <19 years be vaccinated (6). The ACIP vaccination strategies for children and adolescents have been implemented successfully in the United States, and hepatitis B vaccine is now considered part of the routine childhood vaccination schedule. During 1993--2000, the national coverage rate for hepatitis B vaccine among children aged 19--35 months increased from 16% to 90%, and the coverage rate for U.S. adolescents aged 13--15 years increased from near zero to 67%. Part of the success of these strategies can be attributed to the availability of expanded funding for childhood vaccinations and to laws requiring vaccination of school children. In 1994, Congress enacted Vaccines for Children, a national program to purchase ACIP-recommended vaccines for eligible children aged <19 years. Laws have been enacted in 44 states mandating hepatitis B vaccination for children entering elementary schools and childcare centers and in 34 states requiring vaccination for adolescents in middle school (7). Substantial declines in the incidence of acute hepatitis B have occurred among highly vaccinated populations, such as young children and health-care workers. During 1986--2000, the rate of acute hepatitis B among children aged 1--9 years declined >80% (Figure). During 1983--1995, the rate of HBV infection in health-care workers declined 95% and is now lower than the rate for the general U.S. population (8). Since hepatitis B vaccination began in 1982, the prevalence of chronic HBV infection has been reduced substantially among populations whose infection rates previously were high. For example, in 1994, the prevalence of chronic HBV infection among Alaska Natives aged <10 years (i.e., children born after routine vaccination began) was zero, compared with 16% among Alaska Natives aged 11--30 years (9). Preventing Perinatal HBV TransmissionSince 1982, the control of perinatal infection has been a crucial part of ACIP's evolving HBV vaccination strategy. In 1984, ACIP recommended hepatitis B surface antigen (HBsAg) screening for pregnant women in groups at high risk for acquiring HBV infection and postexposure immunoprophylaxis with hepatitis B vaccine and HBIG for all infants born to HBsAg-positive mothers (10). However, within a few years, studies showed that screening women in high-risk groups failed to identify 35%--65% of HBsAg-positive pregnant women (11,12). Consequently, in 1988, ACIP recommended that all pregnant women be screened routinely for HBsAg (13). In 1990, the federal government began funding perinatal hepatitis B prevention programs to promote prenatal screening of all pregnant women for HBsAg and tracking of infants born to HBsAg-positive mothers to ensure that the infants receive appropriate postexposure prophylaxis. These programs have been implemented successfully. A survey of birthing hospitals conducted in 2000 in 14 states showed that 96.5% of pregnant women had been screened for HBsAg (CDC, unpublished data, 2000). During 2000, state health departments identified and tracked 10,192 infants born to HBsAg-positive mothers (CDC, unpublished data, 2000). Of these infants, 90% received hepatitis B vaccine and HBIG before hospital discharge. At age 6--8 months, 71% of these infants had completed the 3-dose hepatitis B vaccine series. On the basis of these coverage rates, CDC estimates that perinatal HBV infection in the United States declined 75% during 1987--2000 (CDC, unpublished data, 2000). Implementation ChallengesSince its inception in 1982, the U.S. hepatitis B vaccination effort has faced several challenges. In the mid-1980s, concern was expressed about the possible risk for human immunodeficiency virus (HIV) transmission by the original plasma-derived vaccine; however, no transmission of any microbial agent was demonstrated, and the safety of the vaccine was reaffirmed (14). Plasma-derived hepatitis B vaccines are no longer used in the United States, but their use continues safely in other countries. The vaccines currently available in the United States are produced by recombinant DNA technology. In 1991, some pediatric-care providers were reluctant to accept the ACIP recommendation that all U.S. infants be vaccinated. However, by 1996, comprehensive efforts to educate providers and parents about hepatitis B and the benefit of vaccination had resulted in broad acceptance of the vaccine (15). In June 1999, concerns were expressed about the risk to young children of mercury exposure from thimerosal, a preservative used in childhood vaccines, including hepatitis B vaccine. As a precaution, the U.S. Public Health Service (PHS), the American Academy of Pediatrics (AAP), and the American Academy of Family Physicians (AAFP) recommended postponing the first dose of hepatitis B vaccine from birth until age 2--6 months for infants born to HBsAg-negative mothers. These groups also recommended eliminating thimerosal from childhood vaccines as soon as possible. By 2000, the two companies that manufacture hepatitis B vaccine in the United States had eliminated thimerosal as a preservative from these vaccines, and PHS, AAP, and AAFP urged the resumption of hepatitis B vaccination at birth. However, the temporary postponement of hepatitis B vaccine at birth resulted in the failure of some hospitals to immunize high-risk infants appropriately. This situation persisted after vaccines that do not contain thimerosal as a preservative became available (16). Although concerns have been expressed over the past 20 years that certain chronic illnesses might be caused by hepatitis B vaccine, no evidence exists that any of these diseases is caused by the vaccine. For example, in the mid-1990s, concerns were expressed that the vaccine might cause multiple sclerosis. However, a report by the Institute of Medicine (IOM) found no evidence of a causal relation between hepatitis B vaccination in adults and multiple sclerosis (17). The vaccine continues to be considered safe by the U.S. Food and Drug Administration, ACIP, IOM, and other national professional vaccination advisory groups. Challenges for the 21st CenturyDespite progress in vaccinating children and adults in some occupational and racial/ethnic groups, approximately 1.2 million persons in the United States have chronic HBV infection, and an estimated 4,000--5,000 persons die each year from HBV-related liver diseases. The goal of eliminating HBV transmission in the United States can be achieved only by sustaining a high level of immunity against HBV infection in all age groups. The prospect for achieving immunity in children is already within reach; 90% of U.S. children aged 2 years receive 3 doses of hepatitis B vaccine, a coverage rate that meets national health goals. To maintain high hepatitis B vaccine coverage, public health professionals must ensure that the safety of hepatitis B vaccine is monitored appropriately through credible scientific studies that assure the public that vaccines are safe. Two important challenges for health departments and health-care providers are maintaining high screening rates among pregnant women for HBsAg and ensuring that newborn infants receive proper immunoprophylaxis. Although high screening rates have been achieved among pregnant women, current efforts to identify and track infants born to HBsAg-positive mothers are inadequate. Advances in the prevention of perinatal HBV transmission will depend on improved health department identification, tracking, and case management of infants born to HBsAg-positive mothers (18). Routine vaccination of adolescents must be increased and aggressive efforts made to vaccinate adults at high risk for HBV infection. Adolescent vaccination will remain an important goal for the next decade, until the cohort of vaccinated infants reaches adolescence. State laws mandating hepatitis B vaccination for middle-school children are effective in achieving high coverage rates (7). Adoption of these laws by more states will increase the adolescent vaccination rate. The greatest remaining challenge for hepatitis B prevention is the vaccination of high-risk adults. The rate of hepatitis B vaccination in this group has remained low, in part because of the difficulty in identifying candidates for vaccination before they become infected and limited public funding for adult vaccination. In serosurveys of MSM aged 15--22 years recruited at public venues in seven U.S. metropolitan areas during 1994--1998, only 9% had serologic evidence of hepatitis B vaccination (19). Among IDUs attending sexually transmitted disease (STD) clinics in San Diego from 1998--2001, only 6% reported previous hepatitis B vaccination (CDC, unpublished data, 2002). The national health objectives for 2010 call for a reduction of 75%--90% in acute hepatitis B cases among high-risk adults (20). To achieve this goal, adults with behavioral risk factors for HBV infection must be identified and vaccinated. Many opportunities to vaccinate high-risk adults are missed. For example, approximately 56% of adults with acute hepatitis B have received care previously in correctional facilities or STD treatment clinics, where vaccination could have been offered (21). The most effective approach to vaccinating high-risk adults is to integrate hepatitis B vaccination into programs that provide services to persons with risk factors for HBV infection (e.g., STD clinics, HIV counseling and testing sites, correctional facilities, and drug treatment clinics). CDC is working with state and local public health departments to integrate comprehensive hepatitis prevention measures, including hepatitis B vaccination, into programs providing services to persons at risk for HBV infection. In addition, CDC has funded cooperative agreements at 18 sites around the country to identify the most effective approaches to achieve integration of hepatitis B vaccination into these programs. Sustaining high vaccine-coverage rates among infants, children, and adolescents will ensure that future generations are protected from HBV infection and its consequences. However, unless efforts to vaccinate adults at increased risk for HBV infection are greatly expanded, complete elimination of HBV transmission might take another 20 years to achieve. Reported by: National Immunization Program; Div of Viral Hepatitis, National Center for Infectious Diseases, CDC. References
* Health-care providers, clients, and staff of institutions for the developmentally disabled, hemodialysis patients, men who have sex with men, injection-drug users, recipients of clotting factors for bleeding disorders, household and sexual contacts of persons with chronic HBV infection, populations with high rates of HBV infection (e.g., Alaska Natives, Pacific Islanders, and immigrants and refugees from countries in which HBV is endemic), and inmates of long-term correctional facilities.
|
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services. |
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 6/27/2002
|
|
|||||
|
HOME |
ABOUT MMWR |
MMWR SEARCH |
DOWNLOADS |
RSS
|
CONTACT
|
|||||
|
|
|||||
|
This page last reviewed 6/27/2002