 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Drug-Susceptible Tuberculosis Outbreak in a State Correctional Facility Housing HIV-Infected Inmates --- South Carolina, 1999--2000During 1999--2000, South Carolina's Department of Corrections (SCDC), Department of Health and Environmental Control (DHEC), and CDC investigated an outbreak of drug-susceptible tuberculosis (TB) that occurred in a state correctional facility housing human immunodeficiency virus (HIV)-infected inmates. All culture-confirmed case-patients have been linked by IS6110-based DNA fingerprinting of Mycobacterium tuberculosis isolates (1). This report describes the outbreak investigation and illustrates the need for increased vigilance for TB in settings in which HIV-infected persons congregate. During 1998, SCDC began mandatory HIV testing upon incarceration of all inmates with negative or unknown HIV serostatus, and in November 1998, began segregating HIV-infected prisoners, placing them in three dormitories of one prison with each dormitory partitioned into right and left sides. On admission to the facility, all inmates were screened for TB infection and disease with a tuberculin skin test (TST)* and chest radiography. TST-negative inmates undergo a TST annually. During mid-August 1999, the source case-patient, a HIV-infected man aged 34 years housed on the right side of one of the dormitories (dormitory A), was diagnosed at a community hospital with sputum acid-fast bacilli (AFB) smear-positive pulmonary TB. His CD4 lymphocyte count was 17 cells/µL (normal range: 359--1519 cells/µL)], and he was not receiving antiretroviral therapy. In 1984, he had a documented TST reaction of 15mm; however, two attempts to treat his latent TB infection (LTBI) with isoniazid were discontinued because of gastrointestinal side effects. In early July 1999, 6 weeks before his TB diagnosis, he was taken to the same hospital with a 2-week history of fever, abdominal pain, and cough. His chest radiograph was normal; sputum specimens were not obtained for AFB smear and culture, and he was not placed in respiratory isolation. He was returned to the prison in mid-July without a definitive diagnosis. In late August, corrections medical staff learned of a second case of sputum smear-positive pulmonary TB in a former dormitory A inmate who had been released in July 1999. SCDC and DHEC began a contact investigation of dormitory A inmates in early September 1999. Inmates who had had contact with a case-patient and had signs and symptoms of active TB were transferred from dormitory A to respiratory isolation for medical evaluation. The exposure period for identifying contacts was 6 weeks before signs of TB appeared in the source case-patient to the day the last sputum culture-positive case-patient left dormitory A (i.e., May 1--September 30, 1999). The exposed cohort comprised 323 men who had spent from 1 to 152 days (median: 135 days) in dormitory A during that period. Screening consisted of TST, chest radiograph, and symptom review for all dormitory A inmates; follow-up TST was conducted on remaining TST-negative inmates in December 1999 (Table 1). As of November 2000, 31 current or former inmates had TB diagnosed (Figure 1). All case-patients were non-Hispanic black men born in the United States and HIV- infected. The median age was 36 years (range: 23--56 years); 19 cases were culture-confirmed and 19 isolates were tested by IS6110-based DNA fingerprinting and demonstrated a matching nine-band pattern. Of the 31 case-patients, 27 (87%) resided on the right side of dormitory A during the exposure period; four (13%) resided on the left. Five case-patients had TB diagnosed after being released from prison; all five were released before the source case-patient had TB diagnosed the previous August. A medical student who examined the source case-patient during the July hospitalization had sputum AFB smear-positive cavitary TB diagnosed in December; the DNA fingerprint of the student's isolate matched the outbreak pattern bringing the number of related cases to 32. Reported by: S Patterson, D Bugenske, South Carolina Dept of Corrections, Columbia; C Pozsik, E Brenner, MD, R Bellew, MD, D Drociuk, MSPH, S Rabley, TB Control; J Gibson, MD, State Epidemiologist, South Carolina Dept of Health and Environmental Control. Div of Applied Public Health Training, Epidemiology Program Office; Surveillance and Epidemiology Br, Div of Tuberculosis Elimination, National Center for HIV, STD, and TB Prevention, and EIS officers, CDC. Editorial Note:Persons infected with both HIV and M. tuberculosis are at high risk for developing TB disease and for an accelerated progression from TB infection to disease (2,3). Persons with HIV infection who are placed in settings such as prisons, hospital wards, group residences, and homeless shelters contribute to outbreaks of TB (4,5). In this report, the source case-patient was a longterm inmate who developed TB disease after a long period of LTBI and unsuccessful LTBI treatment. The outbreak demonstrates that rapid spread of M. tuberculosis to other inmates can be a consequence of segregated housing for HIV-infected inmates. Because inmates transfer within and among correctional facilities and are released upon completion of their sentence regardless of medical status, correctional health and security records should display prisoners' M. tuberculosis infection, disease, and therapy status. Newly incarcerated inmates whose TST status is negative or unknown should be screened for TB infection and disease with medical history and evaluation, TST, and chest radiography. Those with documented positive TST should undergo medical evaluation and chest radiography for signs and symptoms of TB. Medical personnel should attempt to confirm LTBI treatment completion, and treatment of LTBI in prison should be observed directly. For new HIV-infected inmates, screening for TB infection and disease should be thorough; not all HIV-infected persons manifest a TST reaction in the presence of LTBI and may have atypical or negative findings of active disease on chest radiograph (6--8). Additional screening and control measures (e.g., sputum collection for AFB smear and culture and temporary respiratory isolation) may be necessary before the inmate can be housed with the prison population. Those with an undocumented history of LTBI treatment may need to complete a course of directly observed therapy with either a 9-month course of isoniazid or a 2-month course of a rifamycin and pyrazinamide (9). The reasons cited by SCDC for segregating HIV-infected inmates included efforts to reduce the transmission of HIV to uninfected prisoners and to improve medical care for HIV-infected inmates. In 2000, the U.S. Supreme Court upheld a law that permits segregation of HIV-infected inmates in Alabama. As a result, more state correctional systems may adopt this practice (10); therefore, administrative and environmental controls should be strictly maintained. Unlike other acquired immunodeficiency syndrome-associated infections, M. tuberculosis is spread from person-to-person by aerosols and poses a risk for all exposed persons regardless of immune status. A diagnosis of infectious TB should be excluded promptly in all inmates with signs and/or symptoms compatible with TB, and respiratory isolation measures should be applied until infectious TB disease is excluded. For HIV-infected inmates with respiratory signs and symptoms, a diagnosis of infectious TB should be considered even in the presence of a negative chest radiograph. Correctional health-care providers need continuing education to maintain expertise in managing HIV and TB in settings where HIV-infected inmates are incarcerated. References
* TST was defined as induration of >5mm in contacts and HIV-infected inmates. A TST conversion was defined as an increase of >5mm from the most recent TST. Table 1  Return to top. Figure 1 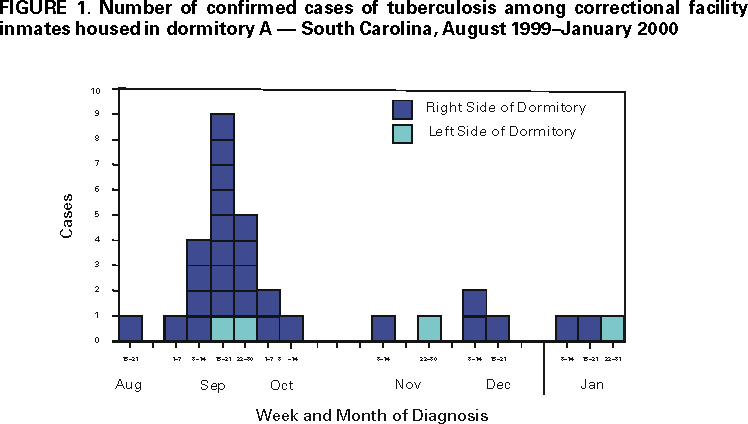 Return to top. Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 11/21/2000 |
|||||||||
This page last reviewed 5/2/01
|