 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Heat-Related Illnesses and Deaths -- Missouri, 1998, and United States, 1979--1996Please note: An erratum has been published for this article. To view the erratum, please click here. Although heat-related illness and death* are readily preventable (5), exposure to extremely high temperatures caused an annual average of 381 deaths in the United States during 1979-1996 (6). Basic behavioral and environmental precautions are essential to preventing adverse health outcomes associated with sustained periods of hot weather (daytime heat index** of greater than or equal to 105 F [greater than or equal to 40.6 C] and a nighttime minimum temperature of 80 F [26.7 C] persisting for at least 48 hours). This report describes four heat-related deaths that occurred in Missouri during 1998, summarizes heat-related deaths in the United States during 1979-1996, describes risk factors associated with heat-related illness and death, especially in susceptible populations (young and elderly, chronically ill, and disabled persons), and recommends preventive measures. Case Reports Case 1. In June 1998, a 92-year-old man was admitted to a city hospital emergency department. He was unresponsive to stimuli, had a heart rate of 170 beats per minute, a rectal temperature of 105.6 F (40.9 C), and a history of heart disease. The medical examiner's report listed the cause of death as hyperthermia as a result of exposure to high environmental temperature. To conserve electricity, his family had not been running the air conditioner in their residence. The daytime heat index recorded at the local airport during the 5 days preceding his death ranged from 102 F to 109 F (38.9 C to 42.8 C). Case 2. In July 1998 at 4:47 p.m., a 4-year-old girl was found in a locked car in front of a child care center. She had disappeared from the center at approximately 10 a.m. Cardiopulmonary resuscitation was administered on the scene, but rigor mortis already had occurred. Death was attributed to hyperthermia. The temperature inside the car at the time of her death was unknown; however, the estimated heat index in the area that day was 93 F (33.9 C). Case 3. In July 1998, a 70-year-old woman was found dead in a mobile home. When she was discovered, the air conditioner was blowing hot air, and the temperature inside the mobile home was approximately 115 F (46 C). The autopsy report indicated that she suffered from congestive heart failure, arthritis, and chronic obstructive pulmonary disease, and that death was caused by pulmonary insufficiency brought about by exposure to excessive heat. Case 4. In July 1998, a 42-year-old man was found dead in his apartment. His partially decomposed body was discovered by police officers investigating reports of a foul odor. The air conditioner was not on. The heat index at the city airport when the man was last seen alive was 93 F (33.9 C). The man had schizophrenia and was under psychiatric care. He also was a heavy smoker and had emphysema. The medical examiner's report indicated that the cause of death was hyperthermia. Missouri During 1979-1996, the years for which data are available, Missouri had the second highest age-adjusted rate for heat-related deaths "due to weather conditions"*** (3 per 1 million population) in the United States. During 1998, after reviewing death certificates, the Missouri Department of Health attributed 12 deaths to high temperatures, and the state's heat surveillance system recorded 470 heat-related illnesses: the average age among decedents was 65.6 years (range: 4-92 years; median 73.5 years); seven (58%) decedents were female. United States During 1979-1996, an annual average of 381 deaths in the United States (6) were attributable to "excessive heat exposure" (range: 148 in 1979 to 1700 in 1980), for an average age-adjusted rate of 2 deaths per 1 million population. During this 18-year period, 6864 deaths were attributable to excessive heat exposure: 2914 (42%) "due to weather conditions," 343 (5%) "of man-made origin," and 3607 (53%) "of unspecified origin." Of the 2862 persons whose death was caused by weather conditions and for whom age data were available, 1745 (61%) were aged greater than or equal to 55 years, and 19 (4%) were aged less than or equal to 14 years. Approximately half of all heat-related deaths occurred among persons aged greater than or equal to 65 years (Figure 1). During 1979-1996, the annual age-adjusted death rate for hyperthermia in this age group was 6 per 1 million. Among persons aged greater than or equal to 35 years, the annual death rate "due to weather conditions" was 1.7 times higher for men (1.5 per 1 million) than for women (0.9 per 1 million), and four times higher for blacks (four per 1 million) than for whites (0.9 per 1 million). Reported by: DC Rackers, Office of Epidemiology, H Donnell, MD, State Epidemiologist, Missouri Dept of Health. Health Studies Br, Div of Environmental Hazards and Health Effects, National Center for Environmental Health; and an EIS Officer, CDC. Editorial Note:All persons are at risk for hyperthermia when exposed to a sustained period of excessive heat (2). The cases described in this report illustrate risk factors associated with heat-related mortality, including age (the young and the elderly), medical history (e.g., cardiovascular disease), social circumstances (e.g., living alone), chronic health conditions (e.g., respiratory diseases), and other conditions that might interfere with the ability to care for oneself (2,3). Also contributing to heat-related illness are alcohol consumption (which may cause dehydration), previous heatstroke, physical activity (e.g., exertion in exceptionally hot environments during work or recreation), and the use of medications that interfere with the body's heat regulatory system, such as neuroleptics (antipsychotics or major tranquilizers) and medications with anticholinergic effects (e.g., tricyclic antidepressants, antihistamines, some antiparkinsonian agents, and some over-the-counter sleeping pills [2-4]). Although the annual death rate from hyperthermia is higher for men aged greater than or equal to 35 years and for black persons than for women aged greater than or equal to 35 years and white persons, the reasons for these differences have not been identified (5). Illnesses associated with high environmental temperatures include heatstroke (hyperthermia), heat exhaustion, heat syncope, and heat cramps (2). Heatstroke is a medical emergency characterized by the rapid onset and increase (within minutes) of the core body temperature to greater than or equal to 105 F (greater than or equal to 40.6 C) and lethargy, disorientation, delirium, and coma (2). Heatstroke is often fatal despite medical care directed at rapidly lowering the body temperature (e.g., ice baths) because in many cases irreparable neurologic damage has occurred (2). Heat exhaustion is characterized by dizziness, weakness, or fatigue often following several days of sustained exposure to hot temperatures and results from dehydration or electrolyte imbalance (2); treatment includes replacing fluids and electrolytes and may require hospitalization (2). Physical exertion during hot weather increases the likelihood of heat syncope and heat cramps caused by peripheral vasodilation (2). Persons who lose consciousness because of heat syncope should be placed in a recumbent position with feet elevated and given fluid and electrolyte replacement (2). For heat cramps, physical exertion should be discontinued and fluids and electrolytes replaced (2,7). Persons working either indoors or outdoors in high temperatures should take special precautions, including allowing 10-14 days to acclimate to high temperatures. Although adequate salt intake is important, salt tablets are not recommended and may be hazardous to many people (2). Although the use of fans may increase comfort at temperatures less than 90 F (less than 32.2 C), they are not protective against heatstroke when temperatures reach greater than or equal to 90 F (greater than or equal to 32.2 C) and humidity is greater than 35% (2,4). Measures for preventing heat-related illness and death include spending time in air-conditioned environments, increasing nonalcoholic fluid intake, exercising only during cooler parts of the day, and taking cool-water baths (2). Elderly persons should be encouraged to take advantage of air-conditioned environments (e.g., shopping malls and public libraries), even if only for part of the day (2-4). Public health information about exceptionally high temperatures should be directed toward susceptible populations. For example, parents should be educated about the heat sensitivity of children aged less than 5 years (2). When a heat wave is predicted, friends, relatives, and neighbors should make an effort to check on elderly, disabled, and homebound persons, and during periods of high temperatures, prevention messages about avoiding heat-related illness should be disseminated as early as possible to prevent heat-related illness, injury, and death. References
* The National Association of Medical Examiners' (NAME) definition of heat-related death includes exposure to high ambient temperature either causing the death or substantially contributing to it, cases where the body temperature at the time of collapse was greater than or equal to 105 F (greater than or equal to 40.6 C), and a history of exposure to high ambient temperature and the reasonable exclusion of other causes of hyperthermia (1). Because death rates from other causes (e.g., cardiovascular and respiratory disease) increase during heat waves (2-4) (defined by the National Weather Service as greater than or equal to 3 consecutive days of temperatures greater than or equal to 90 F [greater than or equal to 32.2 C]), deaths classified as caused by hyperthermia represent only a portion of heat-related mortality. ** Heat index is a measure of the effect of combined elements (e.g., heat and humidity) on the body. *** Underlying cause of death attributed to "excessive heat exposure," classified according to the International Classification of Diseases, Ninth Revision (ICD-9), as code E900.0, "due to weather conditions" (deaths); code E900.1, "of man-made origin" (deaths); or code E900.9, "of unspecified origin" (deaths). These data were obtained from the Compressed Mortality File (CMF) of CDC's National Center for Health Statistics, which contains information from death certificates filed in 50 states and the District of Columbia. All rates were age-standardized to the 1990 U.S. population. Figure 1 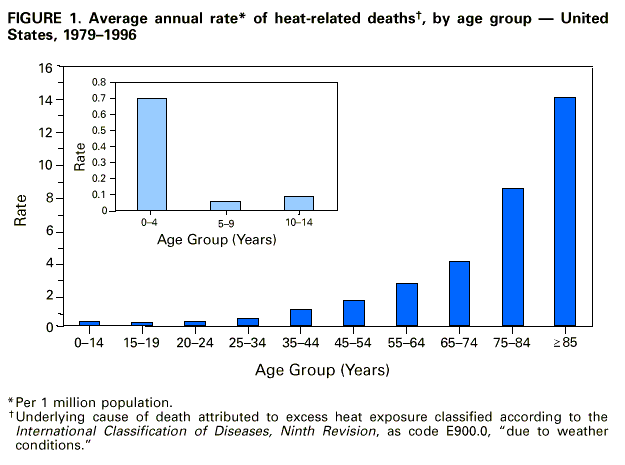 Return to top. Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 6/10/99 |
|||||||||
This page last reviewed 5/2/01
|