 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Surveillance for Waterborne-Disease Outbreaks -- United States, 1995-1996Deborah A. Levy, Ph.D., M.P.H. 1,2 Michelle S. Bens, M.P.H. 2 Gunther F. Craun, M.P.H. 3 Rebecca L. Calderon, Ph.D., M.P.H. 4 Barbara L. Herwaldt, M.D., M.P.H. 2 (1) Epidemic Intelligence Service, Epidemiology Program Office, CDC (2) Division of Parasitic Diseases, National Center for Infectious Diseases, CDC (3) Gunther F. Craun & Associates, Staunton, Virginia (4) Human Studies Division, National Health and Environmental Effects Laboratory, U.S. Environmental Protection Agency Abstract Problem/Condition: Since 1971, CDC and the U.S. Environmental Protection Agency have maintained a collaborative surveillance system for collecting and periodically reporting data that relate to occurrences and causes of waterborne-disease outbreaks (WBDOs). Reporting Period Covered: This summary includes data for January 1995 through December 1996 and previously unreported outbreaks in 1994. Description of the System: The surveillance system includes data about outbreaks associated with drinking water and recreational water. State, territorial, and local public health departments are primarily responsible for detecting and investigating WBDOs and for voluntarily reporting them to CDC on a standard form. Results: For the period 1995-1996, 13 states reported a total of 22 outbreaks associated with drinking water. These outbreaks caused an estimated total of 2,567 persons to become ill. No deaths were reported. The microbe or chemical that caused the outbreak was identified for 14 (63.6%) of the 22 outbreaks. Giardia lamblia and Shigella sonnei each caused two (9.1%) of the 22 outbreaks; Escherichia coli O157:H7, Plesiomonas shigelloides, and a small round structured virus were implicated for one outbreak (4.5%) each. One of the two outbreaks of giardiasis involved the largest number of cases, with an estimated 1,449 ill persons. Seven outbreaks (31.8% of 22) of chemical poisoning, which involved a total of 90 persons, were reported. Copper and nitrite were associated with two outbreaks (9.1% of 22) each and sodium hydroxide, chlorine, and concentrated liquid soap with one outbreak (4.5%) each. Eleven (50.0%) of the 22 outbreaks were linked to well water, eight in noncommunity and three in community systems. Only three of the 10 outbreaks associated with community water systems were caused by problems at water treatment plants; the other seven resulted from problems in the water distribution systems and plumbing of individual facilities (e.g., a restaurant). Six of the seven outbreaks were associated with chemical contamination of the drinking water; the seventh outbreak was attributed to a small round structured virus. Four of the seven outbreaks occurred because of backflow or backsiphonage through a cross-connection, and two occurred because of high levels of copper that leached into water after the installation of new plumbing. For three of the four outbreaks caused by contamination from a cross-connection, an improperly installed vacuum breaker or a faulty backflow prevention device was identified; no protection against backsiphonage was found for the fourth outbreak. Thirty-seven outbreaks from 17 states were attributed to recreational water exposure and affected an estimated 9,129 persons, including 8,449 persons in two large outbreaks of cryptosporidiosis. Twenty-two (59.5%) of these 37 were outbreaks of gastroenteritis; nine (24.3%) were outbreaks of dermatitis; and six (16.2%) were single cases of primary amebic meningoencephalitis caused by Naegleria fowleri, all of which were fatal. The etiologic agent was identified for 33 (89.2%) of the 37 outbreaks. Six (27.3%) of the 22 outbreaks of gastroenteritis were caused by Cryptosporidium parvum and six (27.3%) by E. coli O157:H7. All of the latter were associated with unchlorinated water (i.e., in lakes) or inadequately chlorinated water (i.e., in a pool). Thirteen (59.1%) of these 22 outbreaks were associated with lake water, eight (36.4%) with swimming or wading pools, and one(4.5%) with a hot spring. Of the nine outbreaks of dermatitis, seven (77.8%) were outbreaks of Pseudomonas dermatitis associated with hot tubs, and two (22.2%) were lake-associated outbreaks of swimmer's itch caused by Schistosoma species. Interpretation: WBDOs caused by E. coli O157:H7 were reported more frequently than in previous years and were associated primarily with recreational lake water. This finding suggests the need for better monitoring of water quality and identification of sources of contamination. Although protozoan parasites, especially Cryptosporidium and Giardia, were associated with fewer reported outbreaks than in previous years, they caused large outbreaks that affected a total of approximately 10,000 persons; all of the outbreaks of cryptosporidiosis were associated with recreational water, primarily swimming pools. Prevention of pool-associated outbreaks caused by chlorine-resistant parasites (e.g., Cryptosporidium and to a lesser extent Giardia) is particularly difficult because it requires improved filtration methods as well as education of patrons about hazards associated with fecal accidents, especially in pools frequented by diaper-aged children. The proportion of reported drinking water outbreaks associated with community water systems that were attributed to problems at water treatment plants has steadily declined since 1989 (i.e., 72.7% for 1989-1990, 62.5% for 1991-1992, 57.1% for 1993-1994, and 30.0% for 1995-1996). This decrease might reflect improvements in water treatment and in operation of plants. The outbreaks attributed to contamination in the distribution system suggest that efforts should be increased to prevent cross-connections, especially by installing and monitoring backflow prevention devices. Actions Taken: Surveillance data that identify the types of water systems, their deficiencies, and the etiologic agents associated with outbreaks are used to evaluate the adequacy of current technologies for providing safe drinking and recreational water. In addition, they are used to establish research priorities and can lead to improved water-quality regulations. INTRODUCTION Since 1920, national statistics on outbreaks associated with drinking water have been available (1). Since 1971, CDC, the U.S. Environmental Protection Agency (EPA), and the Council of State and Territorial Epidemiologists have maintained a collaborative surveillance system consisting of the collection and periodic reporting of data on the occurrences and causes of waterborne-disease outbreaks (WBDOs) (2-4). The surveillance system includes data about outbreaks associated with drinking and recreational water. This summary includes data for 1995 and 1996 and for previously unreported outbreaks in 1994. CDC's and EPA's efforts related to waterborne-disease surveillance have the following goals: a) to characterize the epidemiology of WBDOs; b) to identify the etiologic agents that caused WBDOs and to determine why the outbreaks occurred; c) to train public health personnel in how to detect and investigate WBDOs; and d) to collaborate with local, state, federal, and international agencies on initiatives to prevent waterborne diseases. The data gathered through this surveillance system are useful for evaluating the adequacy of current technologies for providing safe drinking and recreational water. Surveillance information also influences research priorities and can lead to improved water-quality regulations. EPA REGULATIONS FOR DRINKING WATER Public water systems are regulated under the Safe Drinking Water Act of 1974 (5), as amended in 1986 (6) and 1996 (7). Microbial contamination is regulated under the Surface Water Treatment Rule of 1989 (8) and the Total Coliform Rule of 1989 (8-10). The Surface Water Treatment Rule includes regulations for filtration, disinfection, and turbidity, as well as treatment criteria for removing Giardia lamblia, viruses, Legionella, and heterotrophic plate-count bacteria. All public community and noncommunity water systems that use surface-water sources or groundwater sources under the direct influence of surface water are covered by the Surface Water Treatment Rule, which requires these water systems to disinfect their water and to maintain a disinfectant residual in their distribution system. Filtration must also be provided unless water sources meet specified criteria for water quality and source-water protection. The Total Coliform Rule was promulgated specifically to identify public water systems that are contaminated or vulnerable to contamination. The total coliform group of organisms (see Glossary), which includes but is not limited to fecal coliforms and Escherichia coli, is used to indicate the possible presence or absence of pathogens and thus, provides a general indication of whether water is contaminated. The presence of fecal coliforms or E. coli provides stronger evidence than does a positive total coliform test of fecal contamination and the likely presence of pathogens (9). Additional rules are being developed. The Enhanced Surface Water Treatment Rule, proposed July 29, 1994 (11), and the Ground Water Disinfection Rule, which has yet to be proposed, also will address the prevention of waterborne diseases. The Enhanced Surface Water Treatment Rule will propose changes to the Surface Water Treatment Rule to provide additional protection against Cryptosporidium parvum and other waterborne pathogens, including Giardia and viruses. The regulation will be implemented in two stages: an interim rule and a final rule. Treatment requirements under the interim Enhanced Surface Water Treatment Rule are scheduled to be announced in late 1998. The Ground Water Disinfection Rule will apply to both community and noncommunity water systems served by groundwater. Maximum contaminant level goals will be set for pathogens. A maximum contaminant level goal of zero will be set for viruses and possibly Legionella. No maximum contaminant level goal is expected for heterotrophic plate-count bacteria. In lieu of monitoring for pathogens, performance criteria for water treatment will be established that are expected to produce the desired reduction in levels of pathogens. Minimum levels of disinfection will be proposed for viruses and Legionella, if included in the new rule. To fill gaps in existing data on the occurrence of microbial pathogens and other indicators of microbial contamination, the EPA promulgated the Information Collection Rule (12). This rule requires treatment plants that use surface water and supply communities of greater than or equal to 100,000 persons or that use groundwater systems and supply communities of greater than or equal to 50,000 persons to monitor their source water for specific microbes and chemicals beginning in July 1997. If the concentration of microbes or chemicals exceeds a predetermined threshold, then the utility must also monitor its finished water. Microbial monitoring is intended a) to provide data on the occurrence of pathogens and the effectiveness of treatment for the removal of pathogens and b) to evaluate the adequacy of the Surface Water Treatment Rule and the Total Coliform Rule. The Information Collection Rule requires utilities to monitor for the presence of Cryptosporidium and Giardia, total culturable viruses, and total and fecal coliforms or E. coli at least once a month for 18 months. METHODS Sources of Data State, territorial, and local public health agencies have the primary responsibility for detecting and investigating WBDOs and voluntarily reporting them to CDC on a standard form (CDC form 52.12 {4}). CDC annually requests reports from state and territorial epidemiologists or from persons designated as the WBDO surveillance coordinators. When needed, additional information about water quality and treatment is obtained from the state's drinking water agency. Definition of Terms * The unit of analysis for the WBDO surveillance system is an outbreak rather than an individual case of a particular disease. Two criteria must be met for an event to be defined as a WBDO. First, two or more persons must have experienced a similar illness after either ingestion of drinking water or exposure to water used for recreational purposes. This stipulation that at least two persons be ill is waived for single cases of laboratory-confirmed primary amebic meningoencephalitis and for single cases of chemical poisoning if water-quality data indicate contamination by the chemical. Second, epidemiologic evidence must implicate water as the probable source of the illness. Outbreaks caused by contamination of water or ice at the point of use (e.g., a contaminated water faucet or serving container) are not classified as WBDOs. If primary cases (among persons exposed to contaminated water) and secondary cases (among persons who became ill after contact with primary case-patients) are distinguished on the outbreak report form, only primary cases are included in the total number of cases. If both actual and estimated case counts are included on the outbreak report form, the estimated case count is used if the study population was sampled randomly or the estimated count was calculated by using the attack rate. Public water systems -- classified as either community or noncommunity water systems -- provide piped water to the public for general consumption and are regulated under the Safe Drinking Water Act. A community water system serves year-round residents of a community, subdivision, or mobile-home park that has greater than or equal to 15 service connections or an average of greater than or equal to 25 residents. A noncommunity water system is defined as any public water system that is not a community water system and is used by the general public for greater than or equal to 60 days per year and has greater than or equal to 15 service connections or serves an average of greater than or equal to 25 persons. Noncommunity water systems are divided into nontransient and transient categories, with nontransient noncommunity water systems (e.g., in factories and schools) serving greater than or equal to 25 persons greater than or equal to 6 months of the year. Of the approximately 170,000 public water systems in the United States, 115,000 (68%) are noncommunity systems, serving transients (95,000 systems) and nontransients (20,000); 55,000 (32%) are community systems (EPA Safe Drinking Water Information System data base, 1998). Community water systems serve approximately 243 million persons in the United States (91% of the U.S. population); approximately 24 million persons (9%) rely on private or individual water systems, which are small systems, not owned or operated by a water utility, that serve less than 15 connections or less than 25 persons. In addition, millions of persons use noncommunity systems while traveling or working. Each drinking water system associated with a WBDO is classified as having one of the following deficiencies: 1 = untreated surface water; 2 = untreated groundwater; 3 = treatment deficiency (e.g., temporary interruption of disinfection, chronically inadequate disinfection, and inadequate or no filtration); 4 = distribution system deficiency (e.g., cross-connection, contamination of water mains during construction or repair, and contamination of a storage facility); and 5 = unknown or miscellaneous deficiency (e.g., contaminated bottled water). If more than one deficiency is noted on the report form for an outbreak, the deficiency that most likely caused the outbreak is noted. Recreational waters include swimming pools, whirlpools, hot tubs, spas, water parks, and naturally occurring fresh and marine surface waters. Although the surveillance system includes whirlpool- and hot tub-associated outbreaks of dermatitis caused by Pseudomonas aeruginosa, it does not include wound infections resulting from waterborne organisms (e.g., Aeromonas species). Classification of Outbreaks This surveillance system classifies WBDOs according to the strength of the evidence implicating water (Table_1). The classification numbers (i.e., I-IV) are based on the epidemiologic and water-quality data provided on the report form. Epidemiologic data are weighted more heavily than water-quality data. Thus, although some outbreaks without water-quality data were included in this summary, reports without supporting epidemiologic data were excluded. Outbreaks of Pseudomonas dermatitis and single cases of primary amebic meningoencephalitis or of illness resulting from chemical poisoning are not classified according to this scheme. A classification of I means that adequate epidemiologic and water-quality data were reported but does not necessarily imply that the investigation was optimal. Classification numbers of II-IV do not necessarily imply that the investigations were flawed; the circumstances of each outbreak differ, and not all outbreaks can or should be rigorously investigated. RESULTS 1995-1996 Outbreaks Associated with Drinking Water For the period 1995-1996, 13 states reported a total of 22 outbreaks associated with drinking water. Sixteen outbreaks were reported for 1995 and six for 1996. Wisconsin reported five outbreaks (22.7%), followed by Idaho, which reported three (13.6%). The outbreaks caused an estimated total of 2,567 persons to become ill. The median outbreak size was 22 persons (range: 1-1,449). No deaths were attributed to these outbreaks. Outbreaks were most common in the summer and fall months (Figure_1). Seventeen (77.3%) of the 22 outbreaks occurred during June through October. Twelve (54.5%) of the 22 outbreaks were assigned a classification of I based on epidemiologic and water-quality data, three (13.6%) Class II, and six (27.3%) Class III; an individual case of chlorine poisoning was not classified. Outbreaks are listed individually by state (Table_1), (Table_2) and (Table_3) and are tabulated by the etiologic agent and type of water system (Table_4) and by the type of deficiency and type of water system (Table_5). Etiologic Agents Fifteen (68.2%) of the 22 outbreaks were of infectious or suspected infectious etiology, and seven (31.8%) were attributed to chemical poisoning. Two (9.1%) of the 22 outbreaks were caused by the parasite Giardia, four (18.2%) by bacteria, one (4.5%) by a small round structured virus, and eight (36.4%) were of unknown etiology (Figure_2). Parasites. Two outbreaks in 1995 were caused by Giardia, one in Alaska and the other in New York. The outbreak of giardiasis in Alaska occurred in August, affected 10 persons, and was associated with untreated surface water. The outbreak in New York occurred in December, affected an estimated 1,449 persons, and was associated with surface water that was both chlorinated and filtered. A dose-response relation was found between consumption of municipal water and illness. No interruptions in chlorination were identified at the water plant. Postfilter water turbidity readings, which serve as an index of the effectiveness of filtration, exceeded the regulated limit (i.e., 95% of water samples must be less than 0.5 nephelometric turbidity units {NTUs} for conventional and direct filtration) before and during the outbreak. Bacteria. Four outbreaks were caused by bacteria: two were attributed to Shigella sonnei, one to E. coli O157:H7, and one to Plesiomonas shigelloides. The outbreak of shigellosis in Idaho, which affected 83 persons, occurred at a resort supplied by untreated well water, which became contaminated by sewage from a line that was draining poorly (13). The outbreak of shigellosis in Oklahoma, which affected 10 persons, was associated with tap water in a convenience store that was supplied by chlorinated well water. Although the factors contributing to contamination of the water were not determined, the water was thought to have been inadequately chlorinated. The outbreak of E. coli O157:H7 infection occurred at a summer camp in Minnesota that was supplied by chlorinated spring water. Several of the 33 affected persons had stool cultures that also were positive for Campylobacter jejuni and Salmonella serotype London. Water samples from the spring and distribution system were positive for coliforms and E. coli. The contamination was attributed to flooding from heavy rains and to an improperly constructed spring. The outbreak of Plesiomonas shigelloides infection occurred in a restaurant in New York that was supplied by a noncommunity water system. The outbreak affected 60 persons and is thought to be the largest outbreak of Plesiomonas infection reported in the United States (14). Chlorinated spring water that supplied a kitchen tap in the restaurant had a high coliform count, including E. coli, and the disinfectant residual was zero. The chlorinator was found to be depleted of disinfectant, and cultures of water from the river adjacent to the uncovered reservoir where treated water was stored grew Plesiomonas. Viruses. One outbreak in 1995 was documented to have been caused by a virus, specifically a small round structured virus. The outbreak occurred in September at a high school in Wisconsin and affected 148 persons. The school received its drinking water from a community water supply. Contamination of the potable water system likely occurred from backsiphonage of water through hoses submerged in a flooded football field. However, the source of the virus on the field was not determined. Chemicals. Seven outbreaks of chemical poisoning were reported, one of which was an individual case of chlorine poisoning. A person became ill immediately after drinking water obtained from a Florida restaurant's drive-through window; symptoms included a burning sensation in the throat and vomiting. Water samples obtained on the day of the incident had chlorine levels ranging from 1.2 mg/L to 4.7 mg/L (median: 4.5 mg/L). The source of the excessive levels of chlorine in the drinking water at the restaurant remained unclear. In the two outbreaks of nitrite poisoning (i.e., in California and New Jersey), defective check valves for prevention of backflow allowed chemicals to contaminate drinking water. In California, three persons at a school became ill after consuming water from a system that had a double-check backflow prevention valve that did not meet the industry standard and that allowed chemicals used to treat a cooling tower and chilling system for the school's air conditioning unit to contaminate the drinking water. Furthermore, the valve had rubber gaskets that were badly deteriorated. In New Jersey, the drinking water was contaminated with boiler-conditioning fluids through a faulty backflow check valve. Six persons developed acute onset of cyanosis and were diagnosed with methemoglobinemia caused by nitrites, which are strong oxidizing agents (15). Elevated copper levels in tap water in Wisconsin were associated with gastrointestinal illness in at least 37 persons in private homes. The homes in this community had recently been built or remodeled, and new copper plumbing was thought to have contributed to the contamination of the water. Thirty persons in Florida developed chemical burns in their mouths after they drank water contaminated with sodium hydroxide. The water became contaminated when an operator at the treatment plant unintentionally released the chemical into the water. The pH of the finished water was 11.8. Thirteen persons at a health-care facility in Iowa developed burning in their mouths and flu-like symptoms after drinking water contaminated with a concentrated liquid soap. A valve on the water supply hose to the soap dispenser had been left open, allowing the soap to enter the water system. Vacuum breakers to prevent backsiphonage were installed incorrectly at the soap dispensers. Unidentified Etiologic Agent. The etiologic agent was not identified for eight (36.4%) of the 22 WBDOs associated with drinking water. The illnesses associated with at least four of these outbreaks had incubation periods, durations, and symptom complexes that were consistent with viral syndromes. For five of the six outbreaks for which testing was done, including three of the four outbreaks of suspected viral etiology, stool specimens were negative for bacterial and parasitic pathogens. One of these outbreaks (i.e., an outbreak in 1995 at the restaurant of a resort in Wisconsin) might have been caused by a rotavirus. The state laboratory reported identifying rotavirus in two of six stool specimens with an enzyme immunoassay. Eight stool specimens were tested for enteric pathogens and three for enteroviruses. However, no testing was done for Norwalk-like caliciviruses, which have been more commonly associated with WBDOs than the rotaviruses have been. Of the eight outbreaks for which the etiologic agent was not identified, three outbreaks were associated with untreated well water, three with inadequate chlorination of unfiltered well water, and one with possible short-term cross-connection and backsiphonage problems in the distribution system. The other outbreak was associated with water from an outside tap at a waste-water treatment plant that was not marked as nonpotable. Even though the water was not intended for drinking, this outbreak was categorized as a drinking water outbreak for lack of a better category. Hikers accessed the tap by entering fenced property. The water from the tap was waste water that had been through a sedimentation process twice but still required additional treatment; the water had levels of fecal coliforms greater than 23 most probable number/100 mL. Water-Quality Data Water-quality data (e.g., information about the presence of coliform bacteria, pathogens, or chemical contaminants) were available for 20 (90.9%) of the 22 outbreaks. The relevant chemical was found in water samples for all seven outbreaks of chemical poisoning. Water samples were tested for coliform bacteria during the investigation of 13 (86.7%) of the 15 outbreaks that had a known or suspected infectious etiology and were positive for total coliforms or fecal coliforms for 11 (84.6%) of the 13 outbreaks. No information about the presence of coliforms was available for an outbreak of giardiasis and an outbreak of shigellosis. Coliforms were detected for three (75.0%) of the four bacterial outbreaks, and all eight outbreaks of unknown etiology, including one for which water samples collected 1 month after the outbreak (at a campground using untreated well water) did not exceed prescribed limits. Coliforms were not detected for two outbreaks. Giardia-like cysts and Cryptosporidium-like oocysts were found in a filtered, chlorinated water system during the investigation of an outbreak of giardiasis; but no coliforms were detected in water samples from the distribution system. During the investigation of an outbreak caused by a small round structured virus at a school, no coliforms could be detected 4 days after the water, which was chlorinated and filtered, had been contaminated by backsiphonage. Water System and Water Source Ten (45.5%) of the 22 WBDOs were associated with community systems, 10 (45.5%) with noncommunity systems, and two (9.1%) with individual water systems (Table_4) and (Table_5); (Figure_2). Only three of the 10 outbreaks associated with community water systems were caused by problems at water treatment plants, and the other seven were the result of problems in the water distribution systems and plumbing of individual facilities (e.g., offices, schools, and restaurants). Six of these seven outbreaks were associated with chemical contamination of the drinking water. Two of the six outbreaks were attributed to nitrites that contaminated the water when check valves for prevention of backflow at the facilities malfunctioned; two resulted from copper leaching into the water after plumbing was installed in new homes; one occurred when concentrated liquid soap contaminated the water because of backsiphonage through an improperly installed vacuum breaker; and in one outbreak, the source of the excessive levels of chlorine in the drinking water at a restaurant remained unclear. The seventh outbreak was attributed to a small round structured virus that likely contaminated the drinking water when backsiphonage of water through hoses submerged in a flooded football field occurred. During 1995-1996, outbreaks in noncommunity systems were more likely than those in community systems to be associated with untreated water (40.0% versus 0.0%). Eight (80.0%) of the 10 outbreaks in noncommunity systems were associated with well-water sources, as were three (30.0%) of the 10 community outbreaks. Of the 15 outbreaks with a known or suspected infectious etiology, nine (60.0%) were associated with well-water sources, three (20.0%) with surface-water sources, two (13.3%) with spring-water sources, and one (6.7%) with partially treated sewage. For four (44.4%) of the nine well-water systems, the water was untreated. For another four (44.4%), the identified deficiency was inadequate chlorination or interrupted disinfection (e.g., coliforms, which are chlorine sensitive, were present in tap water). For one (11.1%), the deficiency occurred in the distribution system. The identified deficiency for both outbreaks associated with spring-water systems was inadequate or interrupted chlorination. For the outbreaks associated with surface-water systems, the identified deficiencies were inadequate filtration, backsiphonage, and no treatment. 1995-1996 Outbreaks Associated with Recreational Water For the period 1995-1996, 17 states reported 37 outbreaks associated with recreational water (Table_6), (Table_7) and (Table_8). Twenty-three outbreaks were reported for 1995 and 14 for 1996. The states that reported the most outbreaks were Minnesota (six outbreaks) and Texas (five outbreaks). The 37 outbreaks caused illness in an estimated 9,129 persons. The median outbreak size was 10 persons (range: 1-5,449). All but one of the 22 outbreaks of gastroenteritis occurred during the summer (Figure_1). The six cases of primary amebic meningoencephalitis, all of which were fatal, occurred in summer and early fall. Five (55.6%) of the nine outbreaks of dermatitis (i.e., rash or folliculitis), which all were associated with hot tubs and lakes, occurred during the relatively colder months of September through February. Etiologic Agents Thirty-three (89.2%) of the 37 recreational water outbreaks were of infectious etiology (Table_6), (Table_7) and (Table_8); (Figure_3). Seven (31.8%) of the 22 outbreaks of gastroenteritis were caused by parasites, 10 (45.5%) by bacteria, one (4.5%) by a virus, and four (18.2%) were of unknown etiology (Table_6) and (Table_7). Parasites. Six (27.3%) of the 22 outbreaks of gastroenteritis were caused by Cryptosporidium and one (4.5%) by Giardia. Six of these seven outbreaks were associated with swimming pools and water parks. In 1995, a large outbreak of cryptosporidiosis at a water park in Georgia caused an estimated 5,449 persons to become ill after a probable fecal accident in the children's pool. Some stools were positive for both Cryptosporidium and Giardia. Similarly, in 1996, an estimated 3,000 persons acquired cryptosporidiosis after visiting a water park in California. Again, a few of the stool specimens were also positive for Giardia. Park patrons were exposed to untreated water both at the swimming pool and when water from a jet-ski sprayed an audience watching a show. At a swimming pool in Kansas, 24 persons acquired cryptosporidiosis, one of whom was hospitalized (16). Inadequate filtration and possible fecal accidents in the pool led to an outbreak of cryptosporidiosis associated with a shallow wading pool in Florida. Twenty-two persons became ill, six of whom were hospitalized. Other conditions that might have contributed to the outbreak included overcrowding of the area around the pool, an excessive number of swimmers, loss of water clarity, and an ozonator that was not operational. After heavy rains, runoff that contained cattle feces and that passed from a pasture into a lake led to an outbreak in Indiana in which three persons became ill with cryptosporidiosis. One of the stool specimens was also positive for Giardia cysts. Run-off containing livestock feces might have been responsible for an outbreak of cryptosporidiosis in Nebraska, which affected 14 persons. Seventy-seven persons in Florida became ill after visiting a children's wading pool. Sixty persons had stool specimens that tested positive for Giardia, 17 had specimens that tested positive for Cryptosporidium, and eight had specimens that were positive for both organisms. The wading pool was supplied by municipal well water that was coagulated, settled, filtered, and disinfected with chlorine. In 1995, six cases of primary amebic meningoencephalitis were attributed to Naegleria. All six of the infected children, who ranged in age from 4 to 11 years, died. Infection was acquired when the children swam in a shallow lake, river, pond, or canal. Five of the six cases were associated with exposure in Texas and one in Florida. Bacteria. Ten (45.5%) of the 22 outbreaks of gastroenteritis were attributed to bacteria, and eight of these outbreaks were associated with lakes. Six outbreaks (27.3%) were caused by E. coli O157:H7 (17), three (13.6%) by Shigella sonnei, and one (4.5%) by Salmonella serotype Java. At a swimming pool in Georgia, 18 persons became ill after ingesting water contaminated with E. coli O157:H7. Inadequate chlorination was thought to have allowed the E. coli to multiply. Thirty-four persons became ill from five outbreaks of E. coli O157:H7 infection associated with lakes. All three outbreaks of shigellosis were associated with lakes. In Colorado, a lake contaminated with human feces caused a total of 120 persons to become ill in two outbreaks. In Pennsylvania, soiled diapers were found near the implicated lake, and most of the laboratory-confirmed cases were in children aged less than 10 years who were playing in the sand close to the water. Other. In an outbreak in Idaho in 1996, 55 persons became ill from infection with Norwalk virus. Lake water tested positive for coliforms, and the outbreak was presumptively attributed to fecal contamination by swimmers. No agent could be identified for four (18.2%) of the 22 outbreaks of gastroenteritis; all four of these outbreaks were associated with lakes. An estimated 169 persons were affected in nine outbreaks of dermatitis that were associated with hot tubs or lakes. All nine outbreaks had a known or suspected infectious etiology (Table_8). Pseudomonas aeruginosa was confirmed as the etiologic agent for four of the seven Pseudomonas outbreaks and was suspected (based on the clinical syndrome) for the other three. Schistosoma sp. was the presumptive etiologic agent of the two outbreaks of swimmer's itch. Previously Unreported Outbreaks Reports of three previously unpublished WBDOs for 1994 also were received (Table_9). In the one outbreak associated with drinking water, well water at a small mobile-home park in Florida was inadequately treated, and coliforms were detected in samples of chlorinated water. Two persons were reported to have been ill, one of whom was hospitalized. The other two outbreaks were associated with recreational water and affected an estimated 312 persons. The etiologic agent was not identified for one of these two outbreaks. In the outbreak in Florida, 12 persons had gastroenteritis, two of whom were hospitalized. This outbreak occurred among children and adults who attended a birthday party at a park and swam in a lake, which was fed by an artesian well and had a history of high-quality water. During the investigation, samples of lake water had 80-230 total coliforms/mL and up to 40 fecal coliforms/mL. In a New Jersey state park, at least 300 cases of shigellosis were reported among bathers in the swimming area of a reservoir where numerous fecal accidents were reported and persons were seen rinsing diapers in lake water. Outbreaks Not Classified as Waterborne-Disease Outbreaks Outbreaks attributed to drinking water contaminated at its point of use, rather than at the source or in the distribution system, traditionally are not classified as WBDOs. Seven point-of-use outbreaks that affected a total of 200 persons were reported, one from 1991 and six from the 1995-1996 reporting period. Twenty-one persons became ill with symptoms suggestive of viral gastroenteritis after consuming ice at a picnic in New York in 1991. In Florida, consumption of water from an outdoor faucet equipped with a hose by attendees at a day camp resulted in 77 primary cases of cryptosporidiosis, as well as 24 probable secondary cases in household members (18). Portable water coolers were filled with water from the hose, which was also used for rinsing garbage cans. Water samples from the outdoor faucet were positive for total coliforms and Cryptosporidium, whereas samples collected at other sites at the school where the camp was held and at the municipal water plant were negative or below detectable limits for total coliforms, E. coli, and parasites. Feces were observed on several occasions near the faucet and attached hose; thus, the most likely source of contamination of the water was the hose nozzle. Three outbreaks in the 1995-1996 reporting period were thought to be associated with consumption of contaminated ice. At a church festival in Wisconsin, 27 cases of E. coli O157:H7-related gastroenteritis were associated with consumption of ice from plastic water containers that had been filled with water and then frozen. The possible sources of contamination of the ice included a water faucet, which might have been contaminated while preparing ground beef, and the plastic water containers, which might have been contaminated when they were previously used to store the ground beef. Bagged ice was linked to infection with Campylobacter sp. in seven persons who became ill at a private home in Ohio. The third ice-related outbreak occurred in New Jersey and affected 39 persons who became ill with symptomatology suggestive of viral gastroenteritis after consuming ice that might have been contaminated with human sewage. In Florida, two persons became ill after consuming iced tea that had been left in a water cooler overnight. The acid in the tea caused the metal coils in the water cooler to corrode and release metals into the tea. Seventeen possible WBDOs that occurred during 1995-1996 were not included in this surveillance summary because of insufficient epidemiologic data (i.e., the outbreaks did not meet the criteria for Classes I-IV). DISCUSSION General Considerations About Surveillance Data for Waterborne-Disease Outbreaks The waterborne-disease surveillance data, which identify the types of water systems, their deficiencies, and the respective etiologic agents associated with the outbreaks, are useful for evaluating the adequacy of current technologies for providing safe drinking and recreational water. However, the data in this surveillance summary are subject to at least one important limitation: they probably do not reflect the true incidence of WBDOs or the relative incidence of outbreaks caused by various etiologic agents. Not all WBDOs are recognized, investigated, and reported to CDC or EPA; and the extent to which WBDOs are unrecognized and underreported is unknown. The likelihood that individual cases of illness will be detected, epidemiologically linked, and associated with water varies considerably among locales and is dependent on factors such as public awareness, the likelihood that multiple ill persons consult the same rather than different health-care providers, the interest of health-care providers, availability of laboratory-testing facilities, local requirements for reporting cases of particular diseases, and surveillance and investigative activities and capacities of state and local health and environmental agencies. Therefore, the states that report the most outbreaks might not be those in which the most outbreaks occur. Recognition of WBDOs also is dependent on certain outbreak characteristics; outbreaks involving serious illness are most likely to receive the attention of health authorities. Outbreaks of acute diseases, particularly those characterized by a short incubation period, are more readily identified than those associated with disease from chronic, low-level exposure to an agent (e.g., a chemical). Outbreaks associated with community water systems are more likely to be recognized than those associated with noncommunity systems because the latter serve mostly nonresidential areas and transient populations. Outbreaks associated with individual systems are the most likely to be underreported because they generally involve relatively few persons. The identification of the etiologic agent of a WBDO is dependent on the timely recognition of the outbreak so that appropriate clinical and environment samples can be obtained. The interests and expertise of investigators and the routine practices of local laboratories can also influence whether the etiologic agent is identified. For example, diarrheal stool specimens generally are examined for bacterial pathogens, but not for viruses. In most laboratories, testing for Cryptosporidium is done only if requested and is not included in routine stool examinations for ova and parasites (19). The water-quality data that are collected vary widely among outbreak investigations, depending on such factors as available fiscal, investigative, and laboratory resources. Furthermore, a few large outbreaks can substantially alter the relative proportion of cases of waterborne disease attributed to a particular agent. Finally, the number of reported cases is generally an approximate figure, and the method and accuracy of the approximation vary among outbreaks. 1995-1996 Outbreaks Associated with Drinking Water The number of outbreaks reported for 1995 (i.e., 16) is comparable with those reported for each year during 1987-1994, except for an increase in 1992 (2-4; (Figure_4) and (Figure_5)). However, the number of outbreaks reported for 1996 (i.e., six) is much lower than for previous years. WBDO reports peaked during 1979-1983. The increase and subsequent decrease in the number of reports might reflect, at least in part, changes in surveillance activities (20). The decrease in the number of outbreaks reported for 1996 might indicate the beginning of a new trend or simply might reflect a reporting artifact. The number of outbreaks attributed to various etiologic agents changed for this reporting period. The number caused by parasites decreased substantially from the previous reporting period (i.e., 1993 and 1994), during which 10 reported outbreaks were caused by parasites (i.e., five outbreaks each attributed to Cryptosporidium and Giardia). For the 1995-1996 reporting period, only two outbreaks were caused by parasites. However, one of these two outbreaks (i.e., the outbreak of giardiasis in New York) affected the largest number of persons of any outbreak for this reporting period. The outbreak of giardiasis in New York was associated with surface water that was filtered and disinfected with chlorine. Although no interruptions in chlorination at the water plant were identified, postfilter water turbidity readings, which serve as an index of the effectiveness of filtration, exceeded the regulated limit before and during the outbreak. The occurrence of the two outbreaks of giardiasis underscores the importance of requiring water systems to monitor turbidity, to meet turbidity standards, and to provide an adequate chlorine concentration and contact time (as specified by the Surface Water Treatment Rule) to inactivate Giardia and other organisms that are relatively chlorine-resistant, especially if the surface water is unfiltered (21). Giardia can be inactivated by disinfection without filtration, but only if stringent conditions are consistently maintained. Providing both filtration and chlorination is an example of using multiple barriers to protect water supplies. The outbreak of giardiasis in New York reportedly was the first attributed to a filtered municipal water system in that state and demonstrates that this organism remains a public health risk even in chlorinated and filtered water systems if levels of water turbidity are not consistently maintained (i.e., 95% of water samples must be less than 0.5 NTUs for conventional and direct filtration). Optimal filtration requires frequent, if not continuous, monitoring of the turbidity of the water both before filtration (i.e., after coagulation, flocculation, and/or settling) and after filtration. No outbreaks in 1995 or 1996 were attributed to Cryptosporidium, a protozoan parasite that is greater than 50-fold more chlorine-resistant than Giardia. More stringent EPA standards for acceptable turbidity values have become effective in all states since the outbreak of cryptosporidiosis in Milwaukee in 1993 (22). Many of the large water utilities have joined the Partnership For Safe Water (23), which is an American Water Works Association/EPA activity that helps treatment plants consistently achieve low water turbidity values, reducing the risk for outbreaks of cryptosporidiosis and giardiasis. The number of small utilities that have joined the partnership is unknown. During 1995-1996, all four outbreaks caused by bacteria were associated with noncommunity systems that used either untreated well water or inadequately chlorinated surface or groundwater. Adequate, continuous disinfection of surface water and groundwater used for drinking water should reduce the occurrence of WBDOs, particularly for small systems in which intermittent contamination of wells and springs is difficult to detect or prevent. In addition, wells and springs should be protected from sources of contamination such as surface run-off, septic-tank drainage, and sewage discharges. Unlike in recent years (i.e., 1991-1994), for which no viral outbreaks were reported, one reported outbreak in 1995 was documented to have been caused by a virus. Researchers used electron microscopy to identify a small round structured virus in stool specimens. Methods for detection of enteric viruses have improved greatly in recent years (24). State health departments should be encouraged to submit clinical specimens for viral testing, either at CDC or at state laboratories that have developed the capability to conduct these tests. Seven outbreaks of chemical poisoning were reported to CDC for 1995-1996, which is similar to the number of outbreaks for the 1993-1994 reporting period (i.e., eight). The two outbreaks associated with nitrite poisoning highlight the importance of preventing backflow when potable water systems are connected to boilers and water chillers; approved backflow prevention devices should be used and periodically monitored for effectiveness. EPA has established a maximum contaminant level of 1.0 mg/L for nitrites; this regulation applies to public water systems but not individual water systems. The two outbreaks of copper poisoning underscore the fact that corrosive water can cause leaching of metals from household plumbing and the water distribution system. EPA requires monitoring for copper (and lead) at the tap rather than at the treatment plant, and EPA's action level for copper is 1.3 mg/mL (25). The results of this monitoring are used to determine whether treatment to control corrosion is needed or is being applied properly. Occupants of new and older homes in communities that could have corrosive water might be able to reduce their risk for chemical poisoning by adequately flushing water through the household system before drinking the water, especially if the water has stood overnight. Several reasons could help explain why waterborne chemical poisonings are rarely reported to CDC: a) most poisonings of this nature (e.g., those associated with the leaching of copper from plumbing systems) probably occur in private residences, affect relatively few persons and thus, might not come to the attention of public health officials; b) exposure to chemicals via drinking water can cause illness that is difficult to attribute to chemical intoxication, or it can cause nonspecific symptoms that are difficult to link to a specific chemical; and c) the mechanisms for detecting waterborne chemical poisonings and reporting them to the WBDO surveillance system are not as well established as they are for WBDOs caused by infectious agents. Future efforts should be tailored to improve the sensitivity of surveillance activities, the detection of associations between environmental releases or exposure incidents and individual health events, and the assessment of the public health burden associated with water-related chemical exposures. As in previous reporting periods, except for 1993-1994, a large proportion (8 or 36.4%) of the WBDOs were of unknown etiology (Figure_3) and (Figure_4). Seven (87.5%) of these eight outbreaks were associated with groundwater sources, three (42.9%) of which involved untreated water; three (42.9%) a treatment deficiency; and one (14.3%) a deficiency in the distribution system. Of the eight outbreaks for which the etiologic agent was not identified, most (i.e., seven) were associated with noncommunity or individual systems; this finding reflects the difficulty of investigating outbreaks affecting the transient populations that use water from these systems. The relative proportion of outbreaks associated with various types of water systems has remained fairly constant; the proportions associated with community water systems were 42.3% for 1989-1990, 23.5% for 1991-1992, 46.7% for 1993-1994, and 45.5% for 1995-1996. However, the proportion of reported outbreaks associated with community water systems that were attributed to problems at water treatment plants, and thus affected entire communities, has steadily declined since 1989 (i.e., 72.7% for 1989-1990, 62.5% for 1991-1992, 57.1% for 1993-1994, and 30.0% for 1995-1996). This decrease might reflect improvements in water-treatment practices and in operation of plants. For the 1995-1996 reporting period, most outbreaks (i.e., 7 of 10) associated with community water systems were the result of problems in the distribution system at individual facilities (e.g., a restaurant). Four of these seven outbreaks were associated with problems with backflow prevention devices (i.e., they had not been installed or had been inappropriately installed or inadequately maintained). Unfortunately, such problems at individual facilities are not amenable to actions taken by treatment plants. However, they can be remedied by effective cross-connection control regulations that require inspection and testing. Monitoring, regulating, and standardizing the practices of the multitudinous individual facilities (e.g., offices, schools, and restaurants) in this country is a daunting task. 1995-1996 Outbreaks Associated with Recreational Water The most frequently reported WBDOs caused by exposure to recreational water were outbreaks of gastroenteritis. Swimming and other recreational activities in which the unintentional ingestion of water can occur are known to increase the risk for gastrointestinal illness, even in nonoutbreak settings (26,27). The number of outbreaks of gastroenteritis for 1995-1996 (i.e., 22) was greater than reported for previous years (i.e, 14 each for 1993-1994 and 1991-1992, and 13 for 1989-1990). Although the number of outbreaks caused by parasites decreased from 10 for the previous reporting period to seven for this period, two of these seven, both attributed to Cryptosporidium, accounted for a total of greater than 8,000 ill persons. Each of these recreational water outbreaks affected more persons than the total number of persons affected by all of the reported drinking water outbreaks. In both of these outbreaks, which occurred at water parks, some stool specimens also tested positive for Giardia. The setting for six of the seven outbreaks was a swimming pool or water park. Investigators for only one of the six outbreaks reported that the pool water was inadequately chlorinated. All six outbreaks of cryptosporidiosis reported for 1995-1996 were associated with recreational water (i.e., none with drinking water), five of which were associated with swimming pools. Cryptosporidium, and to a lesser extent Giardia, is resistant to disinfection by chlorine at levels generally used in swimming pools. Because Cryptosporidium oocysts measure only 4-6 um in diameter, pool filtration systems that use sand or other granular materials (without the special chemical pretreatment that is commonly used by the drinking water industry) might not be effective in removing oocysts. Infection can occur after swallowing as few as 10-100 oocysts (28,29). Therefore, presumably swallowing a single mouthful of contaminated water could cause illness. Prevention of recreational water-associated cryptosporidiosis is particularly difficult. Effective prevention measures require efforts to improve filtration methods and the design of pools and to educate patrons. The prolonged time required to filter all the water in a pool, problems in the design of pools that result in areas with poor water circulation (i.e., "dead spots"), and mixing of water from different pools during filtration increase the risk for cryptosporidiosis (30). Improving filtration systems, having specific pools designated for children to reduce the risk of contaminating the entire facility, and having separate filtration systems for the pools for children and those for adults might reduce risk. However, such changes can be costly, and the degree to which they reduce risk is unknown. Behavioral changes, such as showering before entering the pool and restricting access of diaper-aged children to certain pools, will require education of both patrons and facility management because few facilities currently enforce such measures. Development and enforcement of clear and effective policies regarding fecal accidents in recreational water facilities is needed, but the effectiveness of various approaches in this regard is unclear and should be tested. Questions that still need to be addressed include a) how long should a pool be vacated after a fecal accident? b) is it beneficial to drain a pool after a fecal accident? and c) what hyperchlorination strategy should be used, especially for Cryptosporidium? The number of reported outbreaks caused by bacteria increased from four during 1993-1994 to 10 during this reporting period. The same number of outbreaks of swimming-associated shigellosis (i.e., three) were reported during 1993-1994 and this reporting period. The probable source of the pathogen for the three outbreaks during 1995-1996, as for previous outbreaks, was fecal contamination of lake water by swimmers. Five of the six outbreaks caused by E. coli O157:H7 also were associated with lake water, which suggests the need for better monitoring of water quality and identification of sources of contamination; the sixth was associated with water from a swimming pool that was inadequately chlorinated. E. coli O157:H7, like Shigella spp., apparently has a low infectious dose (31,32). Thus, infection can be acquired by swallowing water with low concentrations of these bacteria. In contrast to the outbreaks caused by parasites, most of which were associated with adequately chlorinated water, all of the outbreaks attributed to bacteria were associated with unchlorinated water (i.e., in lakes) or inadequately chlorinated water (i.e., in pools). The outbreaks associated with swimming pools underline the critical need for maintaining adequate chlorination (30). EPA has published criteria for evaluating the quality of both marine and fresh water used for recreation (33,34). Microbial monitoring has been recommended for recreational areas potentially contaminated by sewage. However, the health risk associated with various levels of fecal coliforms has not been established. Prevention efforts have focused on providing adequate bathroom facilities, including diaper-changing areas, at recreational areas and on limiting the number of swimmers per unit area. An additional important measure, although difficult to enforce, is to prevent persons (especially young, nontoilet-trained children) from entering recreational water if they are either experiencing or convalescing from a diarrheal illness. For the period 1995-1996, most of the reported outbreaks of dermatitis associated with hot tubs were directly related to inadequate operation and maintenance procedures. Outbreaks of Pseudomonas dermatitis associated with hot tubs are preventable if water is maintained at a pH of 7.2-7.8 with free, residual chlorine levels in the range of 2.0-5.0 mg/L (35). A person's susceptibility and immersion time, along with the number of bathers per unit area, also could influence the risk for infection (36). For the period 1995-1996, all six deaths associated with recreational water were caused by primary amebic meningoencephalitis, a rarely reported disease in the United States. Naegleria infections are generally acquired during the summer months, when the temperature of fresh water is favorable for multiplication of the organism (37,38). CONCLUSIONS Information from the nationwide surveillance of WBDOs is used to characterize the epidemiology of waterborne diseases in the United States. Data about the types of water systems and deficiencies associated with outbreaks are needed to evaluate the adequacy of current regulations for water treatment and monitoring of water quality. The identification of the etiologic agents of outbreaks is particularly critical because agents newly associated with WBDOs could require new methods of control. Trends in the incidence of WBDOs caused by various etiologic agents can lead to changes in policies or resource allotment. For agents that are recognized as important waterborne pathogens, rapid recognition and control of WBDOs are facilitated by surveillance at the local and state levels. Close communication between local health departments and water utilities is crucial. For example, if epidemiologic evidence suggests the possibility of waterborne transmission, water utilities should be contacted promptly and asked about such factors as recent treatment deficiencies and changes in source-water quality. Similarly, local policies should be developed that specify the thresholds for reporting various water-quality data to health departments. Timely water testing and environmental investigations can facilitate the identification of an outbreak's etiologic agent and the correctable source(s) of water contamination, as well as establish whether control measures (e.g., boil-water advisories) are indicated. Means of improving the surveillance system for WBDOs should be explored. The review of information that has been gathered through other mechanisms (e.g., issuances of boil-water advisories and computerized data on water quality) could facilitate the detection of WBDOs. Special epidemiologic studies are needed that supplement the findings of this surveillance system by addressing such issues as the public health importance of newly identified agents of waterborne disease, the effectiveness of prevention strategies in nonoutbreak settings, and the timeliness with which state and local health departments act in response to these pathogens. State health departments can request epidemiologic assistance and laboratory testing from CDC for the investigation of WBDOs. CDC and EPA can be consulted about the engineering and environmental aspects of water treatment and about collecting large-volume water samples to identify pathogenic viruses and parasites, which require special methods for recovery. Requests for testing for viruses should be addressed to CDC' s Viral Gastroenteritis Section, Respiratory and Enterovirus Branch, Division of Viral and Rickettsial Diseases at (404) 639-3577. Requests for testing for parasites should be addressed to CDC's Division of Parasitic Diseases at (770) 488-7760. Additional information is available from EPA's Safe Drinking Water Hotline (telephone {800} 426-4791; e-mail sdwa@epamail.epa.gov), CDC's Cryptosporidiosis Information Line of the Parasitic Diseases Information Line (voice telephone system {888} 232-3228, fax {888} 232-3299), and the CDC/National Center for Infectious Diseases' home page on the Internet at http://www.cdc.gov/ncidod/ncid.htm. Information about cryptosporidiosis is available at http://www.cdc.gov/ncidod/dpd/ list_crp.htm. WBDOs should be reported to CDC's Division of Parasitic Diseases (telephone {770} 488-7760), and reports may be faxed to (770) 488-7761. Glossary In this glossary, italicized terms that are not names of microorganisms are defined elsewhere in the glossary. Action level: A specified concentration of a contaminant in water; if this concentration is reached or exceeded, certain actions (e.g., further treatment and monitoring) must be taken to comply with a drinking water regulation. Boil-water advisory: A statement to the public advising persons to boil tap water before drinking it. Class: Refer to the Classification of Outbreaks section in the text and to (Table_1) for a comprehensive definition. Coagulation: The process of adding chemicals to water to destabilize charges on naturally occurring particles to facilitate their subsequent aggregation and removal by flocculation and/or filtration. Coliforms: All facultative anaerobic, gram-negative, nonsporeforming, rod-shaped bacteria that ferment lactose with gas and acid formation within 48 hours at 35 C. Community water system: A public water system that serves year-round residents of a community, subdivision, or mobile-home park that has greater than or equal to 15 service connections or an average of greater than or equal to 25 residents. Contact time: The length of time water is exposed to a disinfectant (e.g., chlorine contact time). Cross-connection: Any actual or potential connection between a drinking water supply and a possible source of contamination or pollution (e.g., a waste-water line). Cyst: The infectious stage of Giardia lamblia and some other protozoan parasites that has a protective wall, which facilitates survival in water and other environments. Disinfection by-products: Chemicals formed in water through reactions between organic matter and disinfectants. Distribution system: Water pipes, storage reservoirs, tanks, and other means used to deliver drinking water to consumers or to store it before delivery. Excystation: The release of the internal (i.e., encysted) contents (e.g., trophozoites or sporozoites) from cysts or oocysts. Fecal coliforms: Coliforms that grow and produce gas from lactose at 44.5 C in 24 hours. Filter backwash: The water containing the material obtained by reversing the flow of water through a filter to dislodge the particles that have been retained on it. Filtration: The process of removing suspended particles from water by passing it through one or more permeable membranes or media of small diameter (e.g., sand, anthracite, or diatomaceous earth). Finished water: The water (i.e., drinking water) delivered to the distribution system after treatment, if any. Flocculation: The water treatment process after coagulation that uses gentle stirring to cause suspended particles to form larger, aggregated masses (floc). The aggregates are removed from the water by a separation process (e.g., sedimentation, flotation, or filtration). Free, residual chlorine level: The concentration of chlorine in water that is not combined with other constituents and thus serves as an effective disinfectant. Groundwater system: A system that uses water extracted from the ground (i.e., a well or spring). Heterotrophic microflora: Microorganisms that use organic material for energy and growth. Individual water system: A small water system, not owned or operated by a water utility, that serves less than 15 residences or farms that do not have access to a public water system. Maximum-contaminant level: The maximum permissible concentration (level) of a contaminant in water supplied to any user of a public water system. Nephelometric turbidity units: The units in which the turbidity of a sample of water is measured when the degree to which light is scattered is assessed with a nephelometric turbidimeter. Noncommunity water system: A public water system that a) serves an institution, industry, camp, park, hotel, or business that is used by the public for greater than or equal to 60 days per year; b) has greater than or equal to 15 service connections or serves an average of greater than or equal to 25 persons; and c) is not a community water system. Oocyst: The infectious stage of Cryptosporidium parvum and some other coccidian parasites that has a protective wall, which facilitates survival in water and other environments. Public water system: A system, classified as either a community or a noncommunity water system, that provides piped water to the public for human consumption and is regulated under the Safe Drinking Water Act. Raw water: Surface water or groundwater that has not been treated in any way. Reverse osmosis: A filtration process that removes dissolved salts and metallic ions from water by forcing it through a semipermeable membrane. This process is also highly effective in removing microbes from water. Siphonage: A reversal of the normal flow of water or other liquid caused by a negative-pressure gradient (e.g., within a water system). Source water: Untreated water (i.e., raw water) used to produce drinking water. Surface water: The water in lakes, rivers, reservoirs, and oceans. Total coliforms: Nonfecal and fecal coliforms that are detected with a standard test. Turbidity: The quality (e.g., of water) of having suspended matter (e.g., clay, silt, or plankton), which results in loss of clarity or transparency. Untreated water: Refer to raw water. Water-quality indicator: A microbial, chemical, or physical parameter that indicates the potential risk for infectious diseases associated with use of the water for drinking, bathing, or recreational purposes. The best indicator is one whose density or concentration correlates best with health hazards associated with a given type of hazard or pollution. Water utility: A water provider that distributes drinking water to a community through a network of pipes. Watershed: An area from which water drains to a single point; in a natural basin, the area contributing flow (i.e., water) to a given place or a given point on a stream. Watershed-control program: A program to protect a watershed from sources of contamination or pollution. Acknowledgments The authors thank the state waterborne-disease surveillance coordinators; the state epidemiologists; the state drinking water administrators; the Office of Ground Water and Drinking Water, U.S. Environmental Protection Agency; the Division of Bacterial and Mycotic Diseases and the Division of Viral and Rickettsial Diseases, NCID, CDC; the Division of Environmental Hazards and Health Effects, NCEH, CDC; and Dennis Juranek, Division of Parasitic Diseases, NCID, CDC, for contributing to the waterborne-disease surveillance summary. References
Figure_1 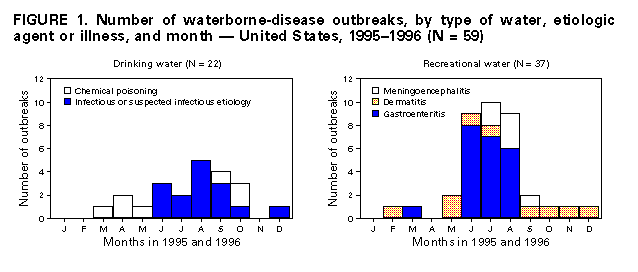 Return to top. Figure_2 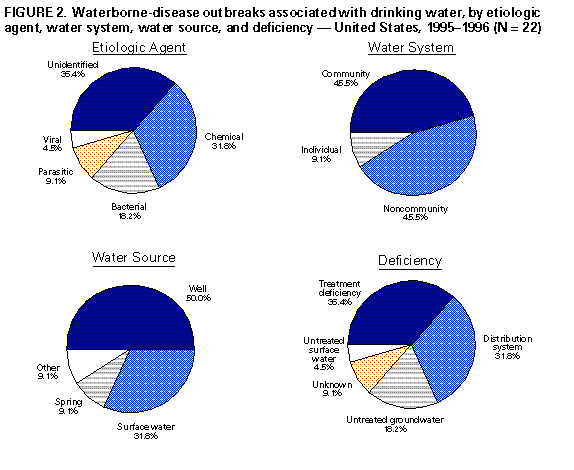 Return to top. Figure_3 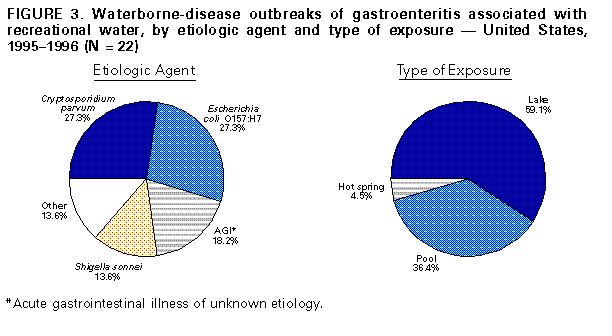 Return to top. Figure_4 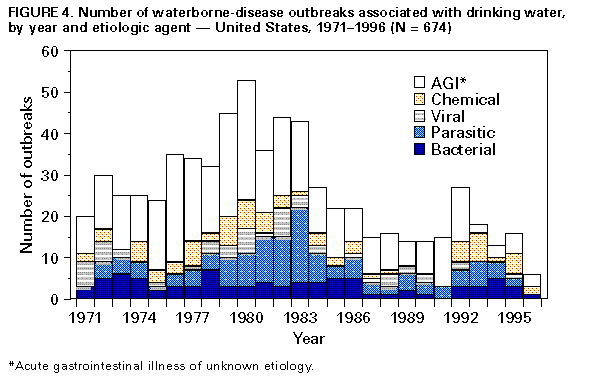 Return to top. Figure_5 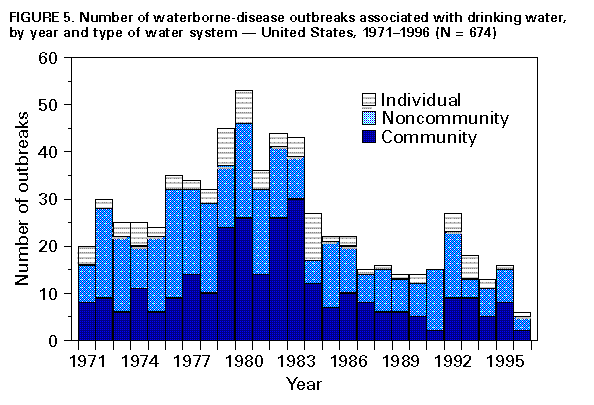 Return to top. Table_1 Note: To print large tables and graphs users may have to change their printer settings to landscape and use a small font size.
TABLE 1. Classification of investigations of waterborne-disease outbreaks -- United States *
=====================================================================================================================
Class+ Epidemiologic data Water-quality data
---------------------------------------------------------------------------------------------------------------------
I ADEQUATE& a) Data were provided about exposed and PROVIDED AND ADEQUATE Could be historical
unexposed persons; and b) the relative risk or information or laboratory data (e.g.,the history
odds ratio was >=2,or the p-value was <0.05 that a chlorinator malfunctioned or a water main
broke,no detectable free-chlorine residual,or the
presence of coliforms in the water)
II ADEQUATE NOT PROVIDED OR INADEQUATE (e.g.,stating that a
lake was crowded)
III PROVIDED,BUT LIMITED a) Epidemiologic data were PROVIDED AND ADEQUATE
provided that did not meet the criteria for Class
I; or b) the claim was made that ill persons had
no exposures in common besides water,but no data
were provided.
IV PROVIDED,BUT LIMITED NOT PROVIDED OR INADEQUATE
---------------------------------------------------------------------------------------------------------------------
* Outbreaks of Pseudomonas dermatitis and single cases of primary amebic meningoencephalitis or of illness resulting
from chemical poisoning are not classified according to this scheme.
+ The classification is based on the epidemiologic and water-quality data that were provided on the form.
& Adequate data were provided to implicate water as the source of the outbreak.
=====================================================================================================================
Return to top. Table_2 Note: To print large tables and graphs users may have to change their printer settings to landscape and use a small font size. TABLE 2. Waterborne-disease outbreaks associated with drinking water -- United States, 1995 (N = 16)* =================================================================================================================================================== State Month Class+ Etiologic agent No. cases Type of system& Deficiency@ Source Setting --------------------------------------------------------------------------------------------------------------------------------------------------- Alaska Aug II Giardia lamblia 10 Ind 1 Surface** Rural area Florida Apr -- ++ Chlorine 1 Com 5 Lake Restaurant Florida May III Sodium hydroxide 30 Com 3 River Water utility Idaho Aug I Shigella sonnei 83 NCom 2 Well Resort Idaho Sept I AGI&& 18 Com 3 Well Community Iowa Oct III Concentrated liquid soap 13 Com 4 Lake Health-care facility Minnesota Jul I Escherichia coli O157:H7 33 NCom 3 Spring Camp Montana Aug II AGI 450 NCom 2 Well Campground New York Dec I G. lamblia 1,449 Com 3 Lake Water utility Oklahoma Oct II S. sonnei 10 NCom 3 Well Store Pennsylvania Aug I AGI 19 NCom 2 Well Inn South Dakota Jun I AGI 48 NCom 2 Well Camp Wisconsin Aug III AGI@@ 26 NCom 3 Well Restaurant Wisconsin Sept I Small round structured virus 148 Com 4 Lake School Wisconsin Sept I Copper 22 Com 4 Well Private home Wisconsin Oct I Copper 15 Com 4 Well Private home --------------------------------------------------------------------------------------------------------------------------------------------------- * Refer to the Methods section for a description of the reporting variables. + Refer to Table 1 for information concerning the classification of outbreaks. & Com = community; NCom = noncommunity; Ind = individual; refer to the Methods section for definitions of the types of water systems. @ Refer to the Methods section for the classification of water- system deficiencies. ** Surface water from an unknown source. ++ Not applicable; see Table 1. && AGI = acute gastrointestinal illness of unknown etiology. @@ See text about the possibility that this outbreak was caused by a rotavirus. =================================================================================================================================================== Return to top. Table_3 Note: To print large tables and graphs users may have to change their printer settings to landscape and use a small font size. TABLE 3. Waterborne-disease outbreaks associated with drinking water -- United States, 1996 (N = 6)* ========================================================================================================================================= State Month Class+ Etiologic agent No. cases Type of system& Deficiency@ Source Setting ---------- ----- ------ -------------------------------------------------------------------------------------------------------- California Apr III Nitrite 3 Com 4 River School California Sept I AGI** 8 Ind 5 Outside tap Waste-water plant Idaho Jul III AGI 94 NCom 3 Well Camp New Jersey Mar I Nitrite 6 Com 4 Mixed++ Office New York Jun I Plesiomonas shigelloides 60 NCom 3 Spring Restaurant Wisconsin Jun III AGI 21 NCom 4 Well Restaurant ---------------------------------------------------------------------------------------------------------------------------------------- * Refer to the Methods section for a description of the reporting variables. + Refer to Table 1 for information concerning the classification of outbreaks. & Com = community; Ncom = noncommunity; Ind = individual; refer to the Methods section for definitions of the types of water systems. @ Refer to the Methods section for the classification of water- system deficiencies. ** AGI = acute gastrointestinal illness of unknown etiology. ++ The source was both surface water and groundwater. ========================================================================================================================================= Return to top. Table_4 Note: To print large tables and graphs users may have to change their printer settings to landscape and use a small font size.
TABLE 4. Waterborne-disease outbreaks associated with drinking water, by etiologic agent and type of water system -- United States, 1995-1996 (N = 22)*
=========================================================================================================================================================
Type of water system+
Community Noncommunity Individual Total
------------------------ ------------------------- ----------------------- -----------------------------
Etiologic agent Outbreaks Cases Outbreaks Cases Outbreaks Cases Outbreaks Cases
---------------------------------------------------------------------------------------------------------------------------------------------------------
AGI& 1 18 6 658 1 8 8 684
Giardia lamblia 1 1,449 0 0 1 10 2 1,459
Shigella sonnei 0 0 2 93 0 0 2 93
Copper 2 37 0 0 0 0 2 37
Nitrite 2 9 0 0 0 0 2 9
Small round structured virus 1 148 0 0 0 0 1 148
Plesiomonas shigelloides 0 0 1 60 0 0 1 60
Escherichia coli O157:H7 0 0 1 33 0 0 1 33
Sodium hydroxide 1 30 0 0 0 0 1 30
Concentrated liquid soap 1 13 0 0 0 0 1 13
Chlorine 1 1 0 0 0 0 1 1
Total 10 1,705 10 844 2 18 22 2,567
(Percentage @) (45.5) (66.4) (45.5) (32.9) (9.1) (0.7) (100.0) (100.0)
---------------------------------------------------------------------------------------------------------------------------------------------------------
* Ordered by total number of outbreaks and secondarily by total number of cases.
+ Refer to the Methods section for definitions of the types of water systems.
& AGI = acute gastrointestinal illness of unknown etiology.
@ The percentage is based on 22 outbreaks or 2,567 cases.
=========================================================================================================================================================
Return to top. Table_5 Note: To print large tables and graphs users may have to change their printer settings to landscape and use a small font size.
TABLE 5. Waterborne-disease outbreaks associated with drinking water, by type of deficiency and type of water system --
United States, 1995-1996 (N = 22)
=======================================================================================================================
Type of water system*
---------------------------------------------------------
Community Noncommunity Individual Total
-------------- --------------- ------------- ---------------
Type of deficiency+ No. (%) No. (%) No. (%) No. (%)
-----------------------------------------------------------------------------------------------------------------------
Untreated surface water 0 ( 0) 0 ( 0) 1 ( 50.0) 1 ( 4.5)
Untreated groundwater 0 ( 0) 4 ( 40.0) 0 ( 0) 4 ( 18.2)
Inadequate treatment 3 ( 30.0) 5 ( 50.0) 0 ( 0) 8 ( 36.4)
Distribution system 6 ( 60.0) 1 ( 10.0) 0 ( 0) 7 ( 31.8)
Miscellaneous or unknown 1 ( 10.0) 0 ( 0) 1 ( 50.0) 2 ( 9.1)
Total 10 (100.0) 10 (100.0) 2 (100.0) 22 (100.0)
-----------------------------------------------------------------------------------------------------------------------
*Refer to the Methods section for definitions of the types of water systems.
+Refer to the Methods section for the classification of water- system deficiencies.
=======================================================================================================================
Return to top. Table_6 Note: To print large tables and graphs users may have to change their printer settings to landscape and use a small font size. TABLE 6. Waterborne-disease outbreaks of gastroenteritis and meningoencephalitis associated with recreational water -- United States, 1995 (N = 17) ======================================================================================================================= State Month Class* Etiologic agent Illness No. cases Source Setting ----------------------------------------------------------------------------------------------------------------------- Florida Aug --+ Naegleria fowleri Meningoencephalitis 1 Canal Canal Georgia Jul I Cryptosporidium parvum Gastroenteritis 5,449 Pool Water park Idaho Mar I Salmonella serotype Java Gastroenteritis 3 Pool Park Illinois Jun I Escherichia coli O157:H7 Gastroenteritis 12 Lake Beach Kansas Jun III C. parvum Gastroenteritis 24 Pool Park Minnesota Jun II AGI& Gastroenteritis 12 Lake Beach Minnesota Jul IV E. coli O157:H7 Gastroenteritis 6 Lake Beach Minnesota Jul IV E. coli O157:H7 Gastroenteritis 2 Lake Beach Nebraska Jul IV C. parvum Gastroenteritis 14 Pool Water park Pennsylvania Aug I AGI Gastroenteritis 17 Lake Park Pennsylvania Aug III Shigella sonnei Gastroenteritis 70 Lake Beach Texas Jul -- N. fowleri Meningoencephalitis 1 River River Texas Jul -- N. fowleri Meningoencephalitis 1 Pond Pond Texas Aug -- N. fowleri Meningoencephalitis 1 Lake Lake Texas Aug -- N. fowleri Meningoencephalitis 1 Lake Lake Texas Sept -- N. fowleri Meningoencephalitis 1 Lake Lake Wisconsin Jun III E. coli O157:H7 Gastroenteritis 8 Lake Beach ----------------------------------------------------------------------------------------------------------------------- *Refer to Table 1 for information concerning the classification of outbreaks. +Not applicable; see Table 1. &AGI = acute gastrointestinal illness of unknown etiology. ======================================================================================================================== Return to top. Table_7 Note: To print large tables and graphs users may have to change their printer settings to landscape and use a small font size. TABLE 7. Waterborne-disease outbreaks of gastroenteritis associated with recreational water -- United States, 1996 (N = 11) ================================================================================================================= State Month Class* Etiologic agent No. cases Source Setting ----------------------------------------------------------------------------------------------------------------- California Aug II Cryptosporidium parvum 3,000 Pool Amusement park Colorado Jul I Shigella sonnei 39 Lake Recreation area Colorado Jul I S. sonnei 81 Lake Recreation area Florida Jun I C. parvum 22 Pool Community Florida Jun I Giardia lamblia+ 77 Pool Community Georgia Jul I Escherichia coli O157:H7 18 Pool Mobile-home park Idaho Jun II Norwalk 55 Hot spring Camp Indiana Aug IV C. parvum 3 Lake Beach Indiana Aug IV AGI& 4 Lake Beach Minnesota Jun IV E. coli O157:H7 6 Lake Beach Oregon Aug IV AGI 32 Lake Camp ----------------------------------------------------------------------------------------------------------------- * Refer to Table 1 for information concerning the classification of outbreaks. + Sixty persons had stool specimens that tested positive only for G. lamblia; 17 had specimens that tested positive only for C. parvum; and eight had specimens that were positive for both organisms. & AGI = acute gastrointestinal illness of unknown etiology. ================================================================================================================= Return to top. Table_8 Note: To print large tables and graphs users may have to change their printer settings to landscape and use a small font size. TABLE 8. Waterborne-disease outbreaks of dermatitis associated with recreational water -- United States, 1995-1996 (N = 9) ==================================================================================================================== State Year Month Class* Etiologic agent No. cases Source Setting -------------------------------------------------------------------------------------------------------------------- Maine 1995 Dec --+ Pseudomonas aeruginosa 10 Hot tub Hotel Minnesota 1995 May -- P. aeruginosa 4 Hot tub Hotel Minnesota 1995 Oct -- P. aeruginosa 6 Hot tub Hotel New Mexico 1995 Sept -- P. aeruginosa 4 Hot tub Apartment complex Oregon 1996 Jun III Schistosoma sp. 71 Lake Beach Oregon 1996 Jul III Schistosoma sp. 50 Lake Beach Washington 1995 Feb -- P. aeruginosa 2 Hot tub Resort Washington 1995 May -- P. aeruginosa 5 Hot tub Spa Washington 1996 Nov -- P. aeruginosa 17 Hot tub Motel -------------------------------------------------------------------------------------------------------------------- * Refer to Table 1 for information concerning the classification of outbreaks. + Not applicable; see Table 1. ==================================================================================================================== Return to top. Table_9 Note: To print large tables and graphs users may have to change their printer settings to landscape and use a small font size. TABLE 9. Waterborne-disease outbreaks of gastroenteritis associated with drinking or recreational water that were not included in the previous surveillance summaries -- United States, 1994 (N = 3)* ============================================================================================================================================================== State Month Year Exposure+ Class& Etiologic agent No. cases Type of system@ Deficiency** Source Setting -------------------------------------------------------------------------------------------------------------------------------------------------------------- Florida Jun 1994 Wid III Escherichia coli O157:H7 2 NCom 3 Well Mobile- home park Florida Jul 1994 Rec I AGI++ 12 --&& --&& Lake Park New Jersey Jun 1994 Rec III Shigella sonnei 300 -- -- Reservoir Park -------------------------------------------------------------------------------------------------------------------------------------------------------------- * Refer to the Methods section for a description of the reporting variables. + Rec = recreational water; Wid = water intended for drinking. & Refer to Table 1 for information concerning the classification of outbreaks. @ Ncom = noncommunity; refer to the Methods section for definitions of the types of water systems. ** Refer to the Methods section for the classification of water- system deficiencies. ++ AGI = acute gastrointestinal illness of unknown etiology. && Recreational water outbreaks are not categorized by type of system or water deficiency. ============================================================================================================================================================== Return to top. Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 12/14/98 |
|||||||||
This page last reviewed 5/2/01
|
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}