 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Progress Toward Poliomyelitis Eradication -- Eastern Africa, 1988-1995In 1988, the World Health Assembly established the goal of eradicating poliomyelitis by the year 2000 (1). Commitment to this goal and to the strategies that have proven effective in other regions (2,3) was reaffirmed in 1995 by the African Regional Health Committee and in 1996 by heads of state attending the Organization of African Unity Summit. These strategies include 1) achieving and maintaining high vaccination coverage among children aged less than 1 year with at least three doses of oral poliovirus vaccine (OPV) through routine vaccination services; 2) establishing effective epidemiologic and laboratory surveillance systems, with examination of stool specimens from suspected cases of polio; and 3) providing supplemental vaccination through National Immunization Days (NIDs) * to interrupt wild poliovirus transmission. This report summarizes progress toward polio eradication since 1988 in the seven countries (Burundi, Eritrea, Kenya, Rwanda, Tanzania, Uganda, and Zambia) of the Eastern Africa Epidemiological Block (EAEB) of the African Region (AFR) of the World Health Organization (WHO) (Figure_1). ** Implementation of these polio-eradication strategies is proceeding rapidly; however, overall surveillance capacity in the EAEB is not yet adequate and requires strengthening. In 1993, all seven EAEB countries were classified by the World Bank as being among the 42 countries with "low income economies," and four of the seven were among the 10 poorest countries in the world (6). In the EAEB countries during 1991, annual gross national products ranged from $100 to $420 per capita (median: $210 per capita), the infant mortality rate ranged from 67 to 135 infant deaths per 1000 live-born infants (median: 115 per 1000), and life expectancy at birth ranged from 46 to 59 years (median: 48 years) (6,7). The estimated population of the EAEB in 1994 was 103 million persons, approximately 20% of the total population of the AFR. All countries of the EAEB have initiated substantial efforts to enhance surveillance for polio. To improve the efficiency and timeliness of surveillance, EAEB countries are developing nationwide systems to immediately report all cases of acute flaccid paralysis (AFP) or "suspected poliomyelitis" to district health offices and to identify geographic areas in which polio remains endemic or focal transmission is occurring. AFP or suspected polio cases are investigated within 48 hours, and a detailed history and two stool specimens are collected from the patient for examination for poliovirus. EAEB countries also are changing their routine reporting systems to include AFP or suspected poliomyelitis and are adopting and distributing the standard WHO case definition for AFP. *** During 1988-1995, the annual incidence of polio in the EAEB declined 91%, from 1813 cases to 160 cases -- reflecting, in part, the reporting by Kenya during 1988-1990 of previous cases of residual paralysis and other diseases as polio (Figure_2). The increase in the number of cases reported in the EAEB during 1992 and 1993 resulted in part from the initiation of polio reporting by Eritrea in 1993 (1 year after gaining its independence): Eritrea reported zero cases in 1993 and 23 cases in 1994. Surveillance for AFP with laboratory examination of stool specimens to isolate poliovirus was initiated in Rwanda, Tanzania, Uganda, and Zambia in 1994, and in Kenya in 1995. In Eritrea, initiation of AFP surveillance with case investigations is planned for early 1997; AFP cases are not investigated in Burundi. In 1995, a total of 113 AFP cases were reported in the EAEB, and stool specimens were collected and examined for 97 cases. Wild poliovirus was isolated from 15 case-patients: three in Tanzania, five in Uganda, and seven in Zambia. WHO-sponsored national polio reference laboratories are fully functional in Kenya, Uganda, and Zambia, and Tanzania is planning to establish a laboratory. These laboratories have the capacity to isolate and type polioviruses and identify other enteroviruses from stool specimens. An indicator of the quality of surveillance for polio is the rate of nonpolio AFP reported through the surveillance system -- a rate of greater than or equal to 1 case per 100,000 children aged less than 15 years indicates adequate completeness of reporting to the system (8). Only Zambia has achieved a national nonpolio AFP reporting rate greater than 1 per 100,000, although reporting is not uniform throughout the country. During 1988-1995, coverage with three doses of OPV among children aged 1 year increased from 53% to 80% in EAEB countries (Figure_2). In 1995, reported OPV coverage was 90% in Rwanda, 84% in Kenya, 82% in Tanzania and Zambia, 79% in Uganda, 62% in Burundi, and 45% in Eritrea. Although civil unrest in Rwanda resulted in disruption of vaccination services and health-care reporting systems in 1994, vaccination coverage increased to 83% in 1995 -- the highest level since 1983. Although Burundi had achieved 87% vaccination coverage in 1992, coverage declined to 64% in 1993 and to 48% in 1994; coverage increased to 62% in 1995, but civil unrest during 1996 could again result in disrupted vaccination services. In Eritrea, coverage increased from 1993 (when reporting of OPV coverage was initiated) through 1994; in 1993 and 1994, coverage levels were 28% and 36%, respectively. In 1996, Kenya, Rwanda, Tanzania, and Zambia conducted NIDs, achieving average coverage levels for the two rounds of 80%, 58%, 100%, and 87%, respectively. Kenya and Tanzania held their NIDs on the same days in August and September. Burundi conducted three 10-day mass-vaccination cycles during the first half of 1996, administering OPV and other routine childhood vaccines to all children aged less than 1 year; however, no data are available to WHO about the number of doses administered and the coverage level attained. In October and November, Eritrea conducted "Sub-National Immunization Days" (SNIDs), administering vaccines only at health centers and outreach posts that already provided routine vaccination services (i.e., fixed sites), and achieved national OPV coverage levels of 61% and 72%. Because only an estimated 50% of the children in Eritrea live within 2.4 miles (5 km) of the fixed sites, the first round was considered highly successful. Uganda is planning its first round of NIDs for December 1996. All seven EAEB countries are planning to conduct NIDs in 1997; Kenya, Tanzania, and Uganda are planning to conduct their rounds concurrently. Reported by: Ministry of Health, Burundi. Ministry of Health, Eritrea. Ministry of Health, Kenya. Ministry of Health, Rwanda. Ministry of Health, Tanzania. Ministry of Health, Uganda. Ministry of Health, Zambia. Expanded Program on Immunization, Regional Office for Africa, Brazzaville, Congo; Global Program for Vaccines and Immunization, World Health Organization, Geneva, Switzerland. Respiratory and Enterovirus Br, Div of Viral and Rickettsial Diseases, National Center for Infectious Diseases; Polio Eradication Activity, National Immunization Program, CDC. Editorial NoteEditorial Note: Despite multiple barriers (e.g., poverty and poorly developed infrastructure -- especially for transportation, communication, and electricity), the countries in the EAEB have made substantial progress toward polio eradication; if efforts and progress can be sustained, these countries should be polio-free by the year 2000 (7,9). Factors accounting for progress in the EAEB include 1) well-established national vaccination programs with substantial experience in cold-chain management and vaccine delivery; 2) widespread knowledge and acceptance by the public of routine vaccination services; 3) the capacities of the district health departments in most EAEB countries to maintain effective surveillance for polio and ensure the success of NIDs; 4) efforts to educate parents about the importance of vaccinations and the need for their children to receive supplemental doses of OPV; and 5) the political commitment of the heads of state, local leaders, and community organizations. For progress to continue toward polio eradication in the EAEB, polio-eradication activities and resources must be used to strengthen primary health care and the integration of health activities while still achieving vaccination program goals. For example, NIDs may divert efforts from other priority health problems and even interfere with routine preventive services. However, reports from EAEB countries that conducted NIDs in 1996 also indicated several benefits of NIDs, including improved planning capacities of district health departments, improved budgeting through more accurate estimation of the costs of vaccination services, the development of new national and local private-sector partners participating in the funding and delivery of vaccination services, enhancement of the vaccine cold chain, increased community participation in social mobilization and the provision of vaccination services, and improved surveillance for vaccine-preventable diseases. Despite efforts to strengthen polio surveillance, overall surveillance capacities in EAEB countries are not yet adequate to document eradication of polio in the EAEB. However, by the end of 1997, all countries in the EAEB are expected to have initiated AFP surveillance, and most should have attained a level of surveillance adequate to meet or exceed globally established indicators of performance. Sustained external political and financial support **** also will be essential to ensure that the goal of polio eradication is achieved in countries of the EAEB. References
* Nationwide mass campaigns over a short period (days to weeks), in which two doses of OPV are administered to all children in the target age group (usually aged less than 5 years), regardless of previous vaccination history, with an interval of 4-6 weeks between doses. ** Although located in eastern Africa, Djibouti, Somalia, and Sudan are part of the Eastern Mediterranean Region (EMR) of the World Health Organization, and progress in the EMR was summarized previously (4,5). In addition, Ethiopia is considered by the AFR as one of four large African countries in especially difficult circumstances and will be reported on separately. *** AFP is defined as acute (i.e., rapid progression), flaccid (i.e., floppy) paralysis, including Guillain-Barre syndrome, in a child aged less than 15 years or any paralytic illness at any age when polio is suspected. **** Support is provided by a coalition of organizations that include WHO, the United Nations Children's Fund (UNICEF), other bilateral and multilateral organizations, and Rotary International. Figure_1 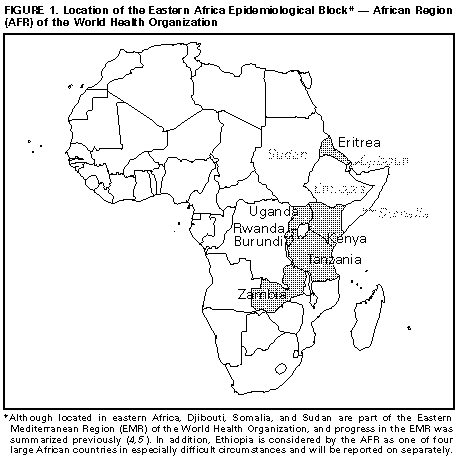 Return to top. Figure_2 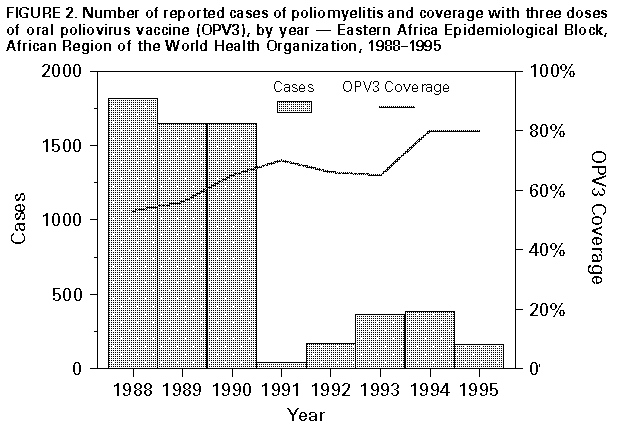 Return to top. Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 09/19/98 |
|||||||||
This page last reviewed 5/2/01
|
{kind=link}
{kind=link}