 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
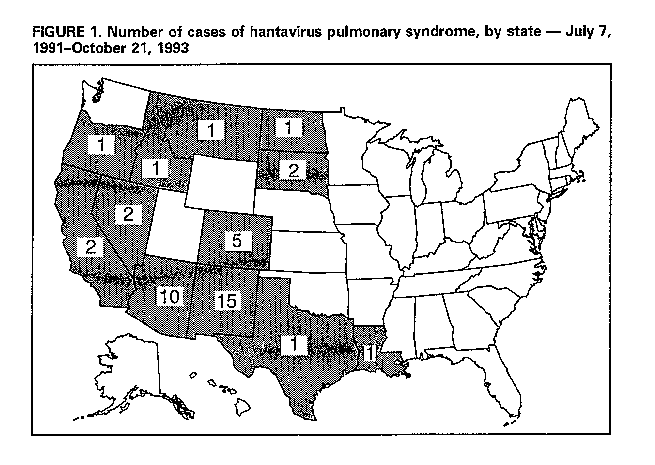
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Update: Hantavirus Pulmonary Syndrome -- United States, 1993A unique hantavirus has been identified as the cause of the outbreak of respiratory illness (hantavirus pulmonary syndrome {HPS}) first recognized in the southwestern United States in May 1993 (1-3). The habitat of the principal rodent reservoir for this virus, Peromyscus maniculatus (deer mouse), extends throughout most of the United States except the Southeast (2). Through October 21, 1993, HPS has been confirmed in 42 persons reported to CDC from 12 states (Figure_1). This report summarizes major clinical, pathologic, and diagnostic findings in patients with this newly recognized syndrome; addresses the use of the investigational antiviral drug ribavirin; and presents revised screening criteria for national surveillance. The earliest retrospectively confirmed case of HPS occurred in July 1991; the two most recently reported case-patients had onsets of illness in September 1993 (Figure_2). Case-patients' ages have ranged from 12 years to 69 years (median: 32 years); 22 (52%) were male. Overall, 26 (62%) case-patients have died. Twenty-three (55%) case-patients were American Indians; 15 (36%), non-Hispanic whites; three (7%), Hispanic; and one (2%), black. Clinical findings. Onset of illness has been characterized by a prodrome consisting of fever, myalgia, and variable respiratory symptoms (e.g., cough) followed by the abrupt onset of acute respiratory distress. Other symptoms reported during the early phase of illness have included headache and gastrointestinal complaints (e.g., abdominal pain, nausea, and/or vomiting). Among 17 case-patients studied in the four-corners region (New Mexico, Arizona, Colorado, and Utah), hemoconcentration was noted on admission in 13 (76%) and thrombocytopenia in 12 (71%). In all case- patients reviewed, bilateral pulmonary infiltrates developed within 2 days of hospitalization. The hospital course was characterized by fever, hypoxia, and hypotension; recovery in survivors has been without sequelae. Pathologic findings. Postmortem examination has routinely revealed serous pleural effusions and heavy edematous lungs. Although histopathologic findings in the lung are characteristic of the illness, the degree of involvement has varied among patients. Microscopic findings have included interstitial infiltrates of mononuclear cells in the alveolar septa, congestion, septal and alveolar edema with or without mononuclear cell exudate, focal hyaline membranes, and occasional alveolar hemorrhage. Cellular debris and neutrophils are not prominent. Large mononuclear cells with the appearance of immunoblasts were found in red and periarteriolar white pulp of the spleen, hepatic portal triads, and other sites. Hantavirus antigens can be detected by immunohistochemistry (IHC) in formalin-fixed tissues using specific monoclonal and polyclonal antibodies. Hantavirus antigens, localized primarily in endothelial cells, have been detected in most organs, with marked accumulations in the lungs. Virologic diagnosis. Adequate serum specimens were available for antibody testing in 39 of the 42 confirmed case-patients; 38 had detectable antibodies against heterologous hantavirus antigens, particularly Prospect Hill virus. One additional case-patient had antibodies detected only with a recombinant protein serologic assay (4). Twenty-seven case-patients had polymerase chain reaction (PCR) evidence of hantavirus ribonucleic acid in frozen lung tissue and/or positive immunohistochemical staining of formalin-fixed tissue for hantavirus antigen, in addition to compatible pathologic findings. Each of three tests -- serology, PCR, and IHC -- were completed for 16 case-patients. The three tests were concordantly positive for 15 case-patients; antibodies against heterologous antigens were not detected in the serum of one patient. In addition, in seven of these patients, PCR testing of peripheral blood mononuclear cells obtained early in the course of disease was positive. Clinical screening criteria. To standardize the investigation and laboratory assessment of persons with possible HPS in the United States, clinical screening criteria were developed by CDC in consultation with the Council of State and Territorial Epidemiologists to detect persons with an illness similar to that of persons with confirmed hantavirus infection reported in the initial outbreak in the four-corners region. Cases meeting the clinical screening criteria (see box Table_B1) should be reported to CDC through state health departments. In addition, patients meeting these clinical screening criteria will need to have laboratory evidence of acute hantavirus infection before they can be confirmed as having HPS. Reported by: S Allen, R Feddersen, K Foucar, MD, B Hjelle, MD, D James, S Jenison, MD, F Koster, MD, H Levy, MD, G Mertz, MD, S Simpson, J Williams, Dept of Pathology, and Dept of Medicine, Univ of New Mexico School of Medicine, Albuquerque; K Nolte, MD, New Mexico Office of Medical Investigations; CM Sewell, DrPH, State Epidemiologist, New Mexico Dept of Health. L Sands, DO, State Epidemiologist, Arizona Dept of Health Svcs. GW Rutherford, III, MD, State Epidemiologist, California Dept of Health Svcs. RE Hoffman, MD, State Epidemiologist, Colorado Dept of Health. FR Dixon, MD, State Epidemiologist, Div of Health, Idaho Dept of Health and Welfare. L McFarland, DrPH, State Epidemiologist, Office of Public Health, Louisiana Dept of Health and Hospitals. TA Damrow, PhD, State Epidemiologist, Montana State Dept of Health and Environmental Sciences. A DiSalvo, MD, State Health Laboratory, Div of Health, Nevada State Dept of Human Resources. LA Shireley, MPH, State Epidemiologist, North Dakota State Dept of Health and Consolidated Laboratories. D Fleming, MD, State Epidemiologist, State Health Div, Oregon Dept of Human Resources. KA Senger, State Epidemiologist, South Dakota State Dept of Health. DM Simpson, MD, State Epidemiologist, Texas Dept of Health. CR Nichols, MPA, State Epidemiologist, Utah Dept of Health. Div of Viral and Rickettsial Diseases, National Center for Infectious Diseases, CDC. Editorial NoteEditorial Note: Clinical syndromes previously associated with hantavirus infections have been characterized by hemorrhagic features and by renal involvement (5). In comparison, the clinical manifestations of hantavirus infection in the United States have been distinguished by the predominance of respiratory symptoms and only limited renal involvement (6,7). No defined set of symptoms and signs reliably distinguishes HPS at the time of presentation from other forms of noncardiogenic pulmonary edema or adult respiratory distress syndrome. In addition to thrombocytopenia and hemoconcentration, other abnormalities have included leukocytosis, increased band forms on differential, hypoalbuminemia, and lactic acidosis. Efforts are ongoing both to identify clinical and laboratory features that distinguish HPS from other infections with similar manifestations and to develop improved diagnostic tests for rapid early diagnosis (7). Serologic tests in combination with PCR and IHC should be used in confirming the diagnosis of acute hantavirus infection. The prognosis is poorest in case-patients with shock and with severe lactic acidosis. Anecdotal reports suggest that periods of severe hypoxia or hypotension before stabilization in the intensive-care setting adversely affect survival. Supportive measures are the basis for therapy; severe hypoxia and overhydration should be avoided or prevented. Pressors or cardiotonic drugs should be employed to maintain perfusion without excessive fluid administration. Testing for alternative diagnoses should be done, and appropriate treatment to cover infections mimicking HPS should be administered early. Observed racial/ethnic differences and the age distribution of cases may reflect differences in activities that facilitate exposure to the rodent reservoir for this virus, usually in rural settings. For example, persons participating in agricultural activities near habitats of infected rodents may be at greater risk for infection. Previously isolated hantaviruses have demonstrated in vitro sensitivity to the investigational antiviral drug ribavirin. Based on this finding and evidence of activity of intravenous ribavirin therapy against Hantaan virus infection (8), intravenous ribavirin has been made available as an investigational agent through a CDC- sponsored open label protocol for patients with HPS. Whether treatment with ribavirin has had any beneficial effect on the course of HPS is unknown. Further plans for study of ribavirin are under consideration by a collaborative working group sponsored by the National Institute for Allergy and Infectious Diseases, National Institutes of Health. Physicians who want to enroll patients should contact the CDC Ribavirin Officer of the Day (telephone {404} 639-1510 weekdays or {404} 639-2888 evenings and weekends). Alternatively, physicians in the four-corners area may contact the enrolling coinvestigator in their state. Physicians must report patients meeting the screening criteria for HPS and submit appropriate clinical samples to state health departments to confirm the diagnosis. References
Screening Criteria for Hantavirus Pulmonary Syndrome in Persons
with Unexplained Respiratory Illness
===========================================================================
Potential case-patients must have one of the following:
-- a febrile illness (temperature greater than or equal to 101 F
{greater than or equal to 38.3 C}) occurring in a previously
healthy person characterized by unexplained adult respiratory
distress syndrome, OR bilateral interstitial pulmonary infiltrates
developing within 1 week of hospitalization with respiratory
compromise requiring supplemental oxygen,
OR
-- an unexplained respiratory illness resulting in death in
conjunction with an autopsy examination demonstrating
noncardiogenic pulmonary edema without an identifiable specific
cause of death.
Potential case-patients are to be excluded if they have any of
the following:
-- a predisposing underlying medical condition (e.g., severe
underlying pulmonary disease, solid tumors or hematologic
malignancies, congenital or acquired immunodeficiency disorders, or
medical conditions {e.g., rheumatoid arthritis or organ transplant
recipients} requiring immunosuppressive drug therapy {e.g.,
steroids or cytotoxic chemotherapy}).
-- an acute illness that provides a likely explanation for the
respiratory illness (e.g., recent major trauma, burn, or surgery;
recent seizures or history of aspiration; bacterial sepsis; another
respiratory disorder such as respiratory syncytial virus in young
children; influenza; or legionella pneumonia).
Confirmed case-patients must have the following:
-- at least one specimen (i.e., serum and/or tissue) available
for laboratory testing for evidence of hantavirus infection.
AND
-- in a patient with a compatible clinical illness, either
serology (presence of hantavirus-specific immunoglobulin M or
rising titers of immunoglobulin G), polymerase chain reaction for
hantavirus ribonucleic acid, or immunohistochemistry for hantavirus
antigen is positive.
===========================================================================
Return to top. Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 09/19/98 |
|||||||||
This page last reviewed 5/2/01
|
{kind=link}
{kind=link}