 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
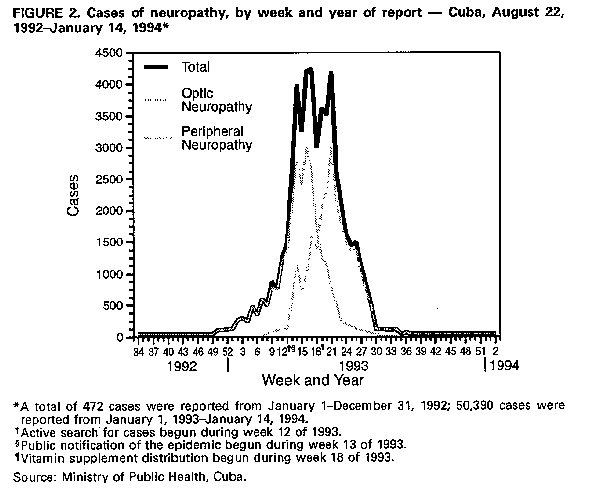
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. International Notes Epidemic Neuropathy -- Cuba, 1991-1994From January 1, 1992, through January 14, 1994, the Ministry of Public Health of Cuba (MINSAP) identified 50,862 cases of a neuropathy in residents of Cuba (1993 population: 10.8 million); affected persons had onset beginning July 1, 1991. The neuropathy has included an optic form -- characterized by subacute (i.e., 3-30 days) onset, decreased visual acuity, decreased color vision, and/or central or cecocentral scotomata -- and a peripheral form; both forms have been characterized by weight loss and easy fatigability. This report presents a preliminary summary of an investigation by MINSAP of this epidemic. In January 1992, physicians in Pinar del Rio, the westernmost province of Cuba (Figure_1, page 189), began to report cases of optic neuropathy, predominantly among adult men who used both tobacco and alcohol; the illnesses were diagnosed as tobacco- alcohol amblyopia. During January-June 1992, 14-36 cases of optic neuropathy were reported each month in rural areas of Pinar del Rio. During 1992, a total of 472 cases were reported in Cuba, including 340 (72%) from Pinar del Rio and 132 (28%) from five of the other 13 provinces. Physicians also reported cases with peripheral neurologic features -- including a predominantly sensory neuropathy and evidence of posterior spinal cord involvement -- with or without simultaneous optic neuropathy. In March 1993, MINSAP initiated intensive case-finding efforts through approximately 18,000 community-based family physicians by using clinical criteria for surveillance case ascertainment * (1). Persons whose clinical presentation met either the optic case definition or both the optic and peripheral case definitions were classified as having the optic form; those with only peripheral signs and symptoms were classified as having the peripheral form. The 50,862 cases accounted for a national cumulative incidence of 461.4 per 100,000 persons (566.7 for females and 368.5 for males). Of these, 26,446 (52%) had the optic form and 24,416 (48%), the peripheral form; the optic form predominated among males and the peripheral form, among females. Age-specific incidence rates were highest for persons aged 45-65 years (926.7 per 100,000) and lowest for children aged less than 15 years (4.2 per 100,000), persons aged greater than 65 years (290.9 per 100,000), and pregnant women. Cumulative incidence rates were highest in Pinar del Rio (1332.8 per 100,000) and lowest in Guantanamo, the easternmost province (65 per 100,000) (Figure_1). Within provinces, however, incidence rates varied widely by municipality. No fatal cases were reported, and resolution was partial to complete in many patients following parenteral treatment with B-complex vitamins. Oral supplements of B-complex vitamins and vitamin A had been provided by MINSAP through community-based family physicians to persons in Pinar del Rio province in March 1993 and to persons in other provinces in May 1993. The incidence of cases decreased during May-June 1993 (Figure_2). Preliminary results of case-control studies conducted by MINSAP in Isla de la Juventud province suggest that risk for illness was associated with tobacco smoking, lower body mass index, and lower intake of animal protein, fat, and foods that contain B-vitamins. Results of sural nerve biopsies indicated noninflammatory axonal neuropathy consistent with a nutritional, metabolic, or toxic etiology. The potential roles of neurotoxic agents and of the Inoue-Melnick agent (2), which has been isolated from many specimens of cerebrospinal fluid (CSF) of patients in Cuba, is still under investigation. Reported by: Ministry of Public Health of Cuba; National Center of Toxicology; Center of Genetic Engineering; Center of Neurosciences; National Center of Scientific Investigations; Coordinating Center for Clinical Trials; Center of Medical/Surgical Investigations; Hospital Hermanos Ameijeiras; Institute of Tropical Medicine Pedro Kouri; Carlos J Finlay Institute; National Institute of Hematology; National Institute of Hygiene, Epidemiology, and Microbiology; Institute of Nutrition and Food Hygiene; National Institute of Neurology; Civil Defense Investigations Laboratory, Havana. Pan American Health Organization, Washington, DC, and Havana. Emory Univ School of Medicine, Atlanta. Center for Food Safety and Applied Nutrition, Food and Drug Administration. Health Studies Br, Div of Environmental Hazards and Health Effects, and Nutritional Biochemistry Br, Div of Environmental Health Laboratory Sciences, National Center for Environmental Health; Maternal and Child Health Br, Div of Nutrition, National Center for Chronic Disease Prevention and Health Promotion; Office of the Director, Epidemiology Program Office; International Health Program Office, CDC. Editorial NoteEditorial Note: The preliminary findings of the investigation described in this report suggest the epidemic neuropathy in Cuba has been associated with nutritional deficiencies. Previous reports have documented the occurrence of a variety of syndromes of myeloneuropathy (including tropical spastic paraparesis, tropical ataxic neuropathy, optic neuropathy, and sensorineural hearing loss) in different tropical regions (3). Although the causes of these syndromes, in general, have been considered multifactorial, specific etiologic agents (e.g., cyanogenic glycosides from cassava {4,5} and human lymphotropic virus type I {6}) have been implicated in some reports. Epidemics of optic and peripheral neuropathy occurred among persons in prisoner-of-war camps in the Middle East and Southeast Asia during World War II (7). Isolated cases of B-vitamin- deficiency syndromes (e.g., beriberi and pellagra) were reported in these settings. However, cases of neuropathy not associated with signs of frank B-vitamin deficiency also were reported. The cause of neuropathies such as these was postulated, but not clearly established, to be related to B-vitamin-complex deficiency, possibly complicated by tropical malabsorption. The investigation of an epidemic of subacute myelo-optic neuropathy (SMON) in Japan during the 1960s implicated use of the antidiarrheal drug clioquinol as a cause of the problem (8); however, the Inoue- Melnick agent -- a virus not previously described -- was isolated from the CSF of many patients in Japan (2), and the role of this putative virus in the etiology of SMON remains undetermined. In Cuba, the apparent clinical response of patients with neuropathy to vitamin supplementation suggests that lifestyle and dietary patterns may be important in this epidemic. Economic difficulties in Cuba since 1989 have been associated with widespread changes in dietary and lifestyle patterns. For example, the consumption of some locally produced foods has increased; the availability of other foods, including meat, dairy products, oils, and fats, has been reduced; and some basic food items (e.g., rice and beans) have been rationed. Toxicity from cyanide or cyanoglycosides in cassava and tobacco can be exacerbated by relative deficiencies of B-vitamins and sulfur-containing amino acids, which are necessary for the detoxification of these compounds (9,10). In addition, because of decreased availability of fuel for transportation, alternative approaches to transportation (e.g., walking or bicycling) have increased personal energy expenditures, which are associated with depletion of B-complex vitamins. In the epidemic described in this report, the incidence of neuropathy was lower in children aged less than 7 years, persons aged greater than or equal to 65 years, and pregnant women -- groups that receive supplements of dairy products; therefore, the low incidence of neuropathy in these groups may reflect the increased consumption of dairy products and, among pregnant women, vitamin supplements. However, because the clinical and epidemiologic patterns of this epidemic of neuropathy differ from those of previously described epidemics associated with toxic etiologies or nutritional deficiencies, the continuing investigation must examine further the potential cause(s) of this problem. MINSAP, in collaboration with the Pan American Health Organization, CDC, the National Institutes of Health, the Food and Drug Administration, and Emory University, is continuing this investigation and is focusing on the role of potentially contributory factors, including dietary insufficiencies, ingested toxins, pesticide exposure, and underlying mitochondrial deoxyribonucleic acid abnormalities. References
For the optic form, major criteria were 1) decreased visual acuity (below 20/25), 2) decreased color vision (failure to identify two or more of the first eight Ishihara plates), 3) bilateral central or cecocentral scotomata, 4) decreased contrast sensitivity, and 5) bilateral loss of optic nerve fibers in the papillo-macular bundle; minor criteria were 1) temporal pallor of optic disk (1 month after symptom onset), 2) photophobia or ocular burning sensation, and 3) loss of horizontal smooth pursuit. A confirmed diagnosis required at least four major criteria. For the peripheral form, major criteria were 1) peripheral sensory symptoms (e.g., tingling, cramps, numbness, and/or burning sensation), 2) decreased perception of vibration or pin prick, and 3) altered deep tendon reflexes in lower limbs, generally with decreased or absent ankle reflex with or without patellar hyperreflexia; minor criteria were
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 09/19/98 |
|||||||||
This page last reviewed 5/2/01
|
{kind=link}
{kind=link}