 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
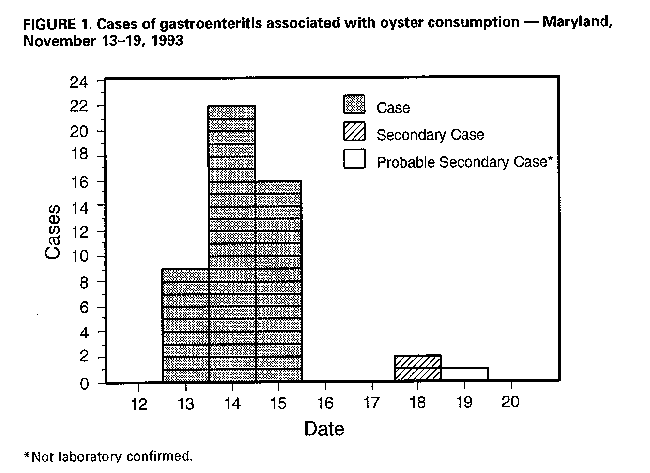
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Multistate Outbreak of Viral Gastroenteritis Related to Consumption of Oysters -- Louisiana, Maryland, Mississippi, and North Carolina, 1993On November 17, 1993, the state health departments of Louisiana, Maryland, and Mississippi notified CDC of several outbreaks of gastroenteritis occurring in their states since November 12. Preliminary epidemiologic investigations identified consumption of oysters as the primary risk factor for illness. On November 16, the Louisiana Department of Health and Hospitals (LDHH) had identified the Grand Pass and Cabbage Reef harvesting areas off the Louisiana coast as the source of oysters associated with outbreaks in Louisiana and Mississippi. Tagged oysters associated with outbreaks in Maryland were traced to the same oyster beds. The oysters harvested from these areas had been distributed throughout the United States. On November 18 and 19, the LDHH and CDC notified state epidemiologists of the potential for oyster-associated illness; outbreaks of oyster-associated gastroenteritis subsequently were identified in Florida and North Carolina. Collaborative investigations by state health officials, the Food and Drug Administration (FDA), and CDC were initiated to determine the magnitude and characteristics of the multistate outbreak, identify the etiologic agent, and trace the oysters. This report summarizes the preliminary findings of the ongoing investigation. * As of December 2, the investigation had identified 23 separate clusters of ill persons in four states. These clusters have accounted for acute gastroenteritis in at least 180 persons who consumed oysters in a variety of settings, ranging from an individual family meal to a 3-day festival attended by 19,000 persons. Similar clinical features of gastroenteritis predominated in all clusters. In Maryland, where 90 ill persons were identified, clinical features included diarrhea (83 {92%}), vomiting (64 {71%}), nausea (60 {67%}), abdominal cramps (55 {61%}), and fever (40 {44%}). For ill persons from Louisiana, Maryland, and Mississippi, the median incubation period was 34 hours (n=146 persons), and median duration of illness was 37 hours (n=137). Raw or steamed oysters were the only food associated with illness; attack rates among the 23 groups ranged from 43% to 100%. Oysters from 20 of 23 outbreaks were traced to the implicated harvest area; oysters or their tags were not available from the other three clusters. Three persons were hospitalized, and at least four cases of secondary transmission have been reported. In one Maryland cluster, associated with a 3-day event beginning on November 12, primary cases first occurred on November 13; secondary cases first occurred on November 18 (Figure_1). Stool specimens were examined by electron microscopy (EM) and reverse transcription-polymerase chain reaction (RT-PCR) methods. Small round structured viruses or Norwalk-like viruses were detected by EM and confirmed by RT-PCR in 13 of 26 stool specimens from ill persons in Louisiana, Maryland, Mississippi, and North Carolina. Oysters associated with several of the outbreaks are being analyzed for the presence of Norwalk-like viruses by RT-PCR. In addition to the notification of state and territorial epidemiologists by LDHH and CDC on November 18 and 19, four public health measures were implemented to prevent further outbreaks associated with the contaminated oysters. First, on November 16, LDHH implemented National Shellfish Sanitation Program (NSSP) procedures for shellfish harvesting closures and recall procedures for oysters from the implicated harvest area (1). Second, on November 18, public health officials in Maryland, North Carolina, and Virginia initiated investigations to identify, detain, and recall all Grand Pass and Cabbage Reef oysters harvested during November 9-11 that had reached the retail markets in their states. Third, on November 23, FDA issued a statement advising consumers that all oysters harvested before November 16 from the Grand Pass and Cabbage Reef areas should not be consumed. Fourth, on November 24, CDC issued a follow-up memorandum to all state and territorial epidemiologists and public health laboratory directors alerting them to the outbreaks and instructing appropriate handling of laboratory specimens if additional outbreaks are suspected. The continuing investigation in Louisiana, Maryland, Mississippi, and North Carolina includes efforts to trace contaminated oysters from the implicated harvest area through large distributors to retailers and consumers. Reported by: C Conrad, Seafood Sanitation Program; K Hemphill, Molluscan Shellfish Program; S Wilson, L McFarland, DrPh, State Epidemiologist, Office of Public Health, Louisiana Dept of Health and Hospitals. K Coulbourne, Talbot County Health Dept, Easton; S Qarni, MD, Baltimore County Health Dept, Baltimore; S Poster, Harford County Health Dept, Bel Air; C Groves, MS, C Slemp, MD, E Butler, D Matuszak, MD, D Dwyer, MD, E Israel, MD, State Epidemiologist, Maryland State Dept of Health and Mental Hygiene. J Cirino, Bureau of Marine Resources; D Cumberland, L Pollack, MD, B Brackin, MPH, M Currier, MD, State Epidemiologist, Mississippi State Dept of Health. H Morris, Beaufort County Health Dept, Washington; M Bissett, S Evans, Craven County Health Dept, New Bern; B Respess, Pitt County Health Dept, Greenville; B Jenkins, J Maillard, MD, R Meriwether, MD, JN MacCormack, MD, State Epidemiologist, North Carolina Dept of Environment, Health, and Natural Resources. B Creasy, J Veazey, K Calci, S Rippey, PhD, G Hoskin, Food and Drug Administration. Div of Field Epidemiology, Epidemiology Program Office; Viral Gastroenteritis Section, Respiratory and Enteric Viruses Br, Div of Viral and Rickettsial Diseases, National Center for Infectious Diseases, CDC. Editorial NoteEditorial Note: Because oysters from the beds implicated in this outbreak were shipped to at least 14 states, ** public health officials, health-care providers, and the public should be informed of the possibility that consumption of oysters from these beds may be associated with clusters and isolated cases of acute gastroenteritis in their states. The cases of gastrointestinal illnesses identified by this investigation were recognized because they occurred as part of discrete clusters; however, it is likely that many isolated cases occurred but were not recognized or reported. For example, a previous study of persons who attended a national convention in Louisiana determined that the risk for acute gastroenteritis was higher among persons who consumed raw shellfish than among those who did not, even though no "outbreaks" were identified (2). Oysters can be traced to their harvest beds because of the regulation requiring sacks of oysters to carry a tag identifying their harvest date and the bed from which they were harvested (1). In this multistate outbreak, these tags facilitated the rapid identification and closing of contaminated beds, provided the link for illness occurring simultaneously in several states, and enabled a product recall. Investigations of shellfish-associated outbreaks of gastroenteritis have implicated a variety of pathogens, including Vibrio species, Salmonella typhi, Campylobacter species, hepatitis A, and Norwalk-like viruses. For most reported outbreaks, however, an etiologic agent is not identified; these outbreaks may be of viral origin (3). Gastrointestinal illness associated with the consumption of virally contaminated oysters characteristically is self-limited and not life-threatening. However, the likelihood of more severe disease may be increased for persons who are immunocompromised or have other chronic problems (e.g., alcoholism; hepatic, gastrointestinal, or hematologic disorders; cancer; diabetes; or kidney disease). The etiology of this multistate outbreak was determined rapidly because specimens were collected and handled appropriately and new PCR-based assays were available (4,5). To enable examination of specimens for viral agents in such outbreaks, the following methods are recommended: 1) collection of large-volume stool specimens in clean, dry containers during the first 48 hours of illness and storage at 39 F (4 C) and 2) collection of acute- (within 1 week of onset of illness) and convalescent-phase (3-4 weeks after onset) serum specimens. FDA, NSSP, and the Interstate Shellfish Sanitation Conference have developed guidelines to protect consumers by controlling the harvesting, handling, and processing of shellfish products (6). Additional efforts are required to develop new assays for screening for viral pathogens in these products before distribution to consumers and to evaluate the effectiveness of various food-preparation practices in decreasing the risk for infection associated with the consumption of molluscan shellfish. References
* Because the outbreaks in Florida have been linked to consumption of oysters from harvest areas other than the Louisiana coast, those outbreaks are not included in this report.
** Alabama, California, Florida, Illinois, Louisiana, Maryland,
Mississippi, Missouri, New Jersey, North Carolina, South Carolina,
Tennessee, Texas, and Virginia. Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 09/19/98 |
|||||||||
This page last reviewed 5/2/01
|
{kind=link}