 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Increase in Coccidioidomycosis --- Arizona, 1998--2001Coccidioidomycosis is a systemic infection caused by inhalation of airborne spores from Coccidioides immitis, a fungus found in soil in the southwestern United States and in parts of Mexico and Central and South America (1). Infection occurs usually following activities or natural events that disrupt the soil, resulting in aerosolization of the fungal arthrospores (2). Clinical manifestations occur in 40% of infected persons and range from an influenza-like illness (ILI) to severe pneumonia and, rarely, extrapulmonary disseminated disease (3). Persons at higher risk for disseminated disease include blacks, Filipinos, pregnant women in their third trimester, and immunocompromised persons (4). During 2001, the Arizona Department of Health Services (ADHS) reported a coccidioidomycosis incidence of 43 cases per 100,000 population, representing an increase of 186% since 1995 (3). To characterize this increase, CDC analyzed data from the National Electronic Telecommunications System for Surveillance (NETSS) and the Arizona Hospital Discharge Database (AHDD), and environmental and climatic data, and conducted a cohort study of a random sample of patients with coccidioidomycosis. This report summarizes the findings of this investigation, which indicate that the recent Arizona coccidioidomycosis epidemic is attributed to seasonal peaks in incidence that probably are related to climate. Health-care providers in Arizona should be aware that peak periods of coccidioidomycosis incidence occur during the winter and should consider testing patients with ILI. Surveillance and HospitalizationsCoccidioidomycosis became a nationally reportable disease at the southwest regional level through NETSS in 1995, at which time a case definition was adopted that required laboratory confirmation*. During 1997, laboratory reporting of coccidioidomycosis became mandatory in Arizona, after which a marked increase was noted in the number of reported cases. However, incidence continued to increase in subsequent years. NETSS data for 1998--2001 were analyzed to calculate incidence by using U.S. Census 2000 data for denominators. During 2001, a total of 2,203 cases were reported to ADHS (rate: 43 cases per 100,000 population), compared with 1,551 cases in 1998 (rate: 33). Persons aged >65 years had the highest incidence (79 during 2001), although incidence in all age groups increased. The youngest age groups experienced the largest increase in incidence during the surveillance period: during 2001, incidence of coccidioidomycosis among patients aged <20 years increased 121%, from approximately five in 1998 to 11 in 2001. Analysis by season demonstrated peak periods of disease incidence during the winter months (November--February) (Figure 1). The baseline rate between peak periods was stable, indicating that the seasonal periods were responsible for the overall annual increase in reported cases. AHDD was reviewed to identify patients with a primary or secondary discharge diagnosis of coccidioidomycosis (International Classification of Diseases, Ninth Revision codes 114.0--114.3 and 114.5--114.9). Hospitalizations caused by coccidioidomycosis increased substantially during the study period. During 2001, a total of 598 persons were discharged with a primary or secondary diagnosis of coccidioidomycosis, compared with 69 persons during 1998; 154 (26%) of the 598 hospitalized patients had disseminated coccidioidomycosis. Persons aged >65 years comprised 34% of all hospitalized patients during the study period and had the highest rate of hospitalization (29 per 100,000 population during 2001). Cohort StudyTo explain peak periods and to further characterize the epidemic, CDC conducted a cohort study of patients from NETSS who had coccidioidomycosis to evaluate host factors, exposures, and outcomes. Patients reported with coccidioidomycosis were divided into four groups based on inclusion in peak or nonpeak periods and year of disease. Of 208 randomly selected persons contacted by telephone, 196 (94%) completed a questionnaire (range per group: 43--56 persons). No statistically significant differences were found between groups related to host risk factors or exposures that could explain the large peak seasons. Geographic Information SystemsGeographic Information Systems (GIS) software was used to identify areas of high incidence in Maricopa County, the most populous county in Arizona. Locations of patients identified in NETSS and AHDD were plotted by postal code by using Arc View v3.2, and incidence was calculated by using U.S. Census 2000 data. The highest incidence of coccidioidomycosis for both NETSS cases and hospitalizations occurred in areas surrounding metropolitan Phoenix (Figure 2). These areas have experienced substantial construction activity according to building permit data provided by the Maricopa County Association of Governments. Seasonal variations in construction activity approximated by building permits were not significantly associated with cases (Table). Environment and ClimateArizona has been experiencing dry weather conditions recently. Environmental and climatic data were analyzed in relation to incidence of disease, and Poisson regression was performed to construct a model that might predict seasonal peaks. Many climatic variables were significantly associated with increased incidence of disease, including drought indices (Palmer Z Index and Palmer Drought Severity Index), wind velocity, mean temperature, dust (measured by concentration of suspended particulate matter <10 microns), and rain (Table). Poisson regression analysis indicated a high correlation (R-squared = 0.75) between incidence of disease and 1) cumulative rain during the preceding 7 months, 2) the average temperature during the preceding 3 months, 3) dust during the preceding month, and 4) the amount of rain during the preceding 2 months in proportion to the preceding 7 months. The projected cases based on the model were compared with the actual cases in Maricopa County (Figure 1). The model accurately mirrored peak seasonal periods during 1998--1999, in particular the large peak beginning in November 2001. In addition, the model accurately described the absence of a seasonal peak during winter 2000--01. Reported by: K Komatsu, V Vaz, C McRill, T Colman, Arizona Dept of Health Svcs; A Comrie, Univ of Arizona Dept of Geography, Tucson. K Sigel, T Clark, M Phelan, R Hajjeh, Div of Bacterial and Mycotic Diseases, National Center for Infectious Diseases; B Park, MD, EIS Officer, CDC. Editorial Note:Coccidioidomycosis is the fourth most common infectious disease reported to ADHS; only gonorrhea, chlamydia, and chronic hepatitis C are more frequent (ADHS, unpublished data, 2002). The findings in this report indicate that the incidence of coccidioidomycosis in Arizona has increased substantially since 1998, affecting all age groups. In addition, hospitalizations for coccidioidomycosis have increased, indicating an increase in the numbers of persons with severe disease. Although seasonality of coccidioidomycosis in Arizona has been suggested previously, this study is the first to confirm the pattern (5,6). In addition, this study documents peak incidence periods during November--February; improved timeliness and completeness of reporting because of mandatory laboratory reporting since 1997 might have helped reveal the seasonal pattern. Seasonal fluctuations could not be explained by differences in the prevalence of the various host risk factors or exposures but were significantly associated with climatic and environmental factors. A climate model incorporating some of these factors recreated the seasonal outbreaks in Maricopa county and predicted that large outbreak seasons might occur during winter seasons following prolonged drought periods, especially in conjunction with hot and dusty conditions. These conditions, which might facilitate aerosolization of arthrospores, have been described in studies of coccidioidomycosis epidemics in California (7). Dry and dusty conditions continue in Arizona, suggesting that another large peak season might occur this winter. Preliminary data for 2002 indicate that the number of total cases already exceeds 3,000, considerably surpassing 2001 levels (ADHS, unpublished data, 2002). Although coccidioidomycosis is not readily preventable, a better understanding of its epidemiology can assist in developing more effective prevention and education strategies and help with earlier diagnosis and appropriate medical management. Health-care providers should consider testing for coccidioidomycosis in any patient who has moved or traveled recently to Arizona and who has ILI, especially during the winter months. Dust reduction measures, such as paving roads or wetting soil at construction sites, are currently in place and might be useful in preventing further cases. Persons at risk for severe disease should avoid activities that might increase their exposure to dust. These persons might benefit from development of a vaccine that confers long-term immunity (6). References
* The laboratory criteria for diagnosis are cultural, histopathologic, or molecular evidence of the presence of Coccidioides spp; a positive serologic test for coccidioidal antibodies in serum or cerebrospinal fluid by 1) detection of coccidioidal IgM by immunodiffusion, enzyme immunoassay (EIA) latex agglutination, or tube precipitin or 2) detection of rising titer of coccidioidal IgM by immunodiffusion, EIA, or complement fixation; or a coccidioidal skin test conversion from negative to positive after the onset of clinical signs and symptoms. Figure 1  Return to top. Figure 2 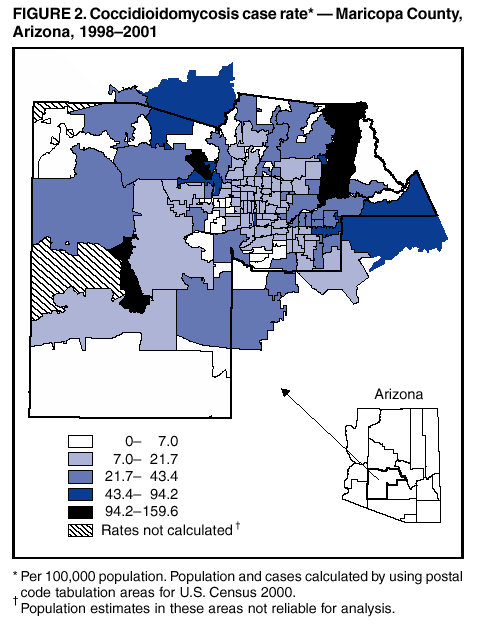 Return to top. Table  Return to top.
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 2/13/2003 |
|||||||||
This page last reviewed 2/13/2003
|