|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
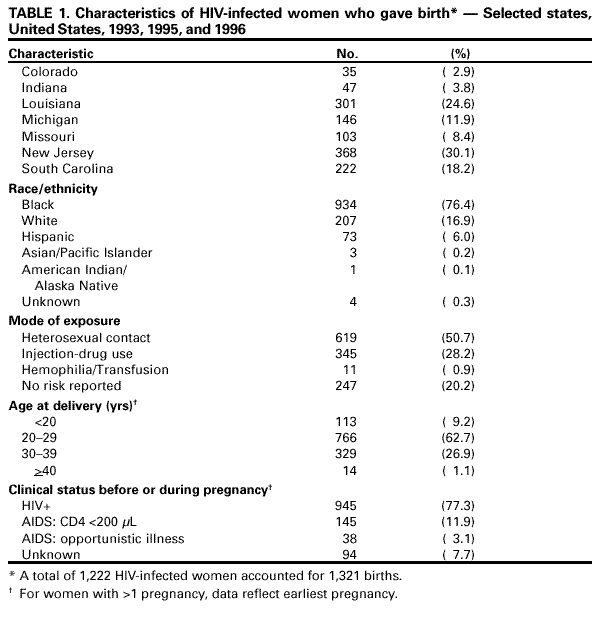
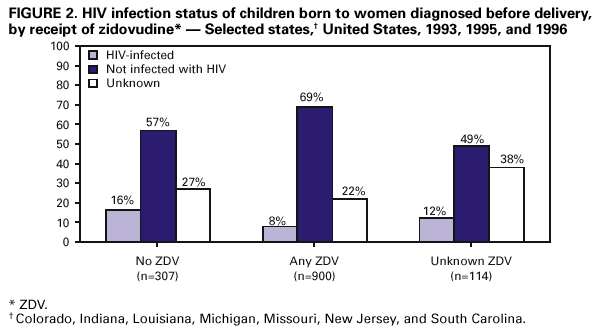
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Successful Implementation of Perinatal HIV Prevention GuidelinesA Multistate Surveillance EvaluationPascale M. Wortley, M.D., M.P.H. SummaryIn 1994, zidovudine (ZDV) was demonstrated to substantially reduce perinatal transmission of the human immunodeficiency virus (HIV). Guidelines regarding the use of ZDV to reduce transmission and regarding counseling and voluntary testing of pregnant women were issued in 1994 and 1995, respectively. Surveillance methods were used to evaluate the implementation of these guidelines and to understand reasons for continued perinatal transmission of HIV. Population-based enhanced perinatal surveillance was used in seven states to collect information regarding mother-infant pairs in 1993, 1995, and 1996. Birth registries and HIV/Acquired immunodeficiency virus (AIDS) registries were matched to determine the number of HIV-infected women with diagnosis before delivery. Supplemental epidemiologic information was collected for 1,321 pairs. The estimated total number of HIV-infected women giving birth each year was derived from the Survey of Childbearing Women, an anonymous serologic survey of the prevalence of HIV infection among women giving birth. From 1993 through 1996, the proportion of HIV-infected women with diagnosis before delivery increased from 70% to 80%. The proportion of women with a diagnosis who received ZDV prenatally increased from 27% to 83% and intrapartum, 6% to 75%; for neonates, the increase was from 8% to 77%. Overall, 14% of women received no or only one prenatal care visit. A total of 36% of women who used illicit drugs during pregnancy had not had prenatal care. Of the children who received any ZDV, 8% were infected compared with 16% of those who received no ZDV. ZDV, used for treating pregnant HIV-infected women, has been rapidly adopted in clinical practice and has reduced the transmission of HIV. To achieve continued declines in perinatal transmission of HIV infection, continued progress is needed in the following areas: a) increases in the proportion of women who receive prenatal care and an HIV diagnosis; and b) implementation of rapid testing methods (when licensed rapid tests are available) or rapid turnaround of standard tests (expedited EIA tests). BACKGROUNDAdult women accounted for 17% of U.S. cases of acquired immunodeficiency virus (AIDS) reported to CDC through June 2000. Most (78%) of the women reported with AIDS are members of racial/ethnic minority populations. During the 1990s, women, minorities, and persons infected through heterosexual contact represented a growing proportion of annual AIDS diagnoses. Because women might transmit the human immunodeficiency virus (HIV) infection perinatally to their infants (prenatally, during labor and delivery, or postpartum during breastfeeding), the HIV/AIDS epidemic in children closely paralleled the epidemic in women until the mid-1990s. In February 1994, zidovudine (ZDV) was demonstrated to be effective in reducing perinatal transmission of HIV infection (1). In August 1994, the U.S. Public Health Service published guidelines regarding the use of ZDV to prevent perinatal transmission of HIV infection; guidelines regarding routine counseling and voluntary testing were published in 1995 to promote timely testing and treatment of HIV-positive pregnant women (CDC unpublished data, U.S. Public Health Service Task Force Recommendations for Use of Antiretroviral Drugs in Pregnant HIV-1-infected Women for Maternal Health and Interventions to Reduce Perinatal HIV-1 Transmission in the United States; <http://www.hivatis.org>) (2,3). In collaboration with state and local health department HIV/AIDS surveillance programs, CDC implemented enhanced surveillance strategies in selected states to determine the extent to which testing and ZDV treatment are occurring in clinical practice and to identify barriers to the universal implementation of the guidelines. The surveillance strategies were designed to enhance the completeness of ascertainment of mother-infant pairs and to collect relevant epidemiologic data from multiple sources. Key objectives included determining the proportion of HIV-infected pregnant women who received the diagnosis of HIV before delivery, the proportion of those who were offered ZDV, and the proportion of children who were infected. In addition, supplemental information (e.g., information concerning prenatal care use) was collected to help identify barriers to the full implementation of the prevention guidelines. The enhanced population-based surveillance was conducted statewide in the participating states as an extension of routine perinatal HIV/AIDS surveillance activities. The data have provided state and local prevention programs with information needed to guide efforts to maximize the reduction of HIV perinatal transmission. The data also provided the scientific basis for current recommendations of the Institute of Medicine to make HIV voluntary testing a routine part of prenatal care (4). As a result, in the United States, intensive programmatic efforts are being implemented in geographic areas heavily affected by the HIV epidemic with the goal of eliminating perinatal HIV transmission. Etiologic Factors Current program efforts for perinatal HIV prevention focus on a cascade of events that must occur in sequence to achieve maximum reductions in HIV transmission from mother to child. Pregnant women must access prenatal care, ideally early during pregnancy. Their prenatal-care provider must counsel women regarding the benefits of knowing their HIV status for their own health and for the health of their babies. Health-care providers must offer women the opportunity for voluntary HIV testing. Pregnant women must accept testing and return to receive their test results. For those women who are found to be HIV-infected, their health-care provider must offer antiretroviral treatment using ZDV (currently often part of a combined antiretroviral regimen), and the woman must accept and adhere to treatment during the recommended intervention periods, antenatally and intrapartum, as well as consent to treatment for her newborn. Mothers and babies must receive ongoing care postpartum. To monitor factors associated with the implementation of voluntary testing and treatment guidelines, the study in this report describes enhanced perinatal surveillance activities undertaken in seven states during the period following the publication of the guidelines. The indicators of prevention effectiveness (e.g., proportions in prenatal care, proportions tested prenatally, and proportions receiving ZDV) are compared for the period immediately preceding (1993) and following (1995--1996) the guidelines that were published during 1994. METHODSEnhanced Perinatal HIV/AIDS Surveillance State and local health departments that conduct surveillance of adult and pediatric HIV infection seek to identify perinatally exposed infants, collect demographic and clinical information (including HIV diagnostic tests, birth history, and maternal and newborn ZDV receipt), and follow up with infants until sufficient laboratory information is available to classify them as infected or not infected, based on the recently expanded case definitions (5). The seven states that collected data on 1993 (i.e., the baseline year before publication of the 1994 findings of the Pediatric AIDS Clinical Trials Group 076 [PACTG 076] that ZDV treatment of pregnant women and newborns reduced the risk for HIV transmission), 1995, and 1996 births were Colorado, Indiana, Louisiana, Michigan, Missouri, New Jersey, and South Carolina. All seven states had HIV reporting in place for at least 3 years before initiating the matching of case and birth registries and had required reporting of all prevalent HIV cases in adult and adolescent women when HIV reporting was implemented. Cases were ascertained by soliciting case reports from institutions and health-care providers as well as laboratory reports of tests diagnostic of HIV infection. Enhanced surveillance consisted of a) increased efforts to completely ascertain mother-infant pairs by matching birth registries to HIV/AIDS registries; and b) the abstraction of information on pairs from all available medical charts, including the mother's prenatal care chart, HIV clinic chart, labor and delivery chart, the child's birth chart, and the child's HIV clinic chart. The information collected included not only the information required for the surveillance case report form but more detailed information on prenatal care, illicit drug use during pregnancy, additional information on ZDV prescription, reasons for discontinuing ZDV, characteristics of labor and delivery, and the mother's disease status. Determining the Proportion of HIV-infected Women With Diagnosis Before Delivery In the participating states, birth registries for 1993, 1995, and 1996 were matched to women reported with HIV/AIDS. HIV-infected women in the mother-infant pairs were considered to have received the diagnosis before delivery if the date of their first HIV- positive test result (in the HIV/AIDS registry) preceded the child's date of birth. The number of HIV-infected women who gave birth during each year and whose HIV infection had been diagnosed before delivery was derived from the total number of matches (including previously identified mother-infant pairs and pairs identified through the registry match) provided. The estimated total number of HIV-infected women who gave birth each year was obtained from the Survey of Childbearing Women (SCBW) when available. The SCBW was an anonymous population-based seroprevalence survey of routinely collected blood specimens from newborns tested for maternal HIV antibody (6). New Jersey and South Carolina had SCBW data for 1993--1996; Colorado, Michigan, and Louisiana had data for 1993--1995; Missouri for 1993 and 1994; and Indiana for 1994. Data from the most recent year were used when data were not available for a given year. These seven states represented approximately 15% of HIV-infected women who gave birth nationwide in 1995. Supplemental Data Collection In six of seven states (all except New Jersey), all HIV-infected women who gave birth during 1993, 1995, and 1996 and whose HIV infection was diagnosed before delivery, and whose children were born during those years were eligible for supplemental chart abstraction. In New Jersey, because of the large number of mother-infant pairs, supplemental data in 1993 and 1996 were limited to women who gave birth during July through December of those years; for 1995, all pairs were eligible. Thus, the total number of pairs eligible for chart abstraction was smaller than the total number of women with diagnosis before delivery. Supplemental data were also collected for mother-infant pairs where mothers were tested at or after delivery. RESULTSIn the participating states during 1993, 1995, and 1996, women for whom HIV infection had been diagnosed before delivery (ascertained through enhanced surveillance) accounted for 1,769 births. In addition, supplemental data were collected for 143 of 348 pairs in those instances when mothers were diagnosed at delivery or later. The matching of birth registries and HIV/AIDS registries to find more mother-infant pairs resulted in an additional 11%--20% of pairs compared with standard surveillance practices. Based on SCBW, an estimated 2,350 births to HIV-infected women were reported in these states during 1993, 1995, and 1996. A total of 2,117 pairs of an estimated total of 2,350 or 90% ascertainment of infants born to HIV-infected women was found. In the seven states, among the estimated births to HIV-infected mothers, the proportion with a diagnosis of HIV before giving birth was 70% (585/831) in 1993 (median: 79%; range: 47%--87%); 76% (595/779) in 1995 (median: 77%; range: 58%--100%); and 80% (589/740) in 1996 (median: 83%; range: 50%--95%). The proportions of women with diagnosis before delivery and who were first tested during pregnancy were 51% for 1993, 44% for 1995, and 47% for 1996. A total of 1,534 pairs that included mothers who had an HIV diagnosis before delivery were eligible for abstraction (464 in 1993, 595 in 1995, and 475 in 1996). Supplemental data were collected in addition to data on the case report form for 1,321, or 86% of eligible pairs (413 [89%] in 1993; 487 [82%] in 1995; 421 [89%] in 1996). The supplemental data for 1,321 mother-infant pairs represented a total of 1,222 women, 99 of whom had two births. The proportion of eligible pairs for whom supplemental data was obtained differed by state (range: 77%--94%; median: 90%). Three states (Louisiana, New Jersey, and South Carolina) accounted for 73% of women; black women accounted for 76%; women infected through heterosexual contact accounted for 51%; women aged 20--29 years accounted for 63%; and women for whom AIDS had been diagnosed before or during pregnancy accounted for 15% (Table 1). A substantial increase occurred in the use of prenatal, intrapartum, and neonatal ZDV and in the proportion of mothers and their HIV-exposed infants who received ZDV during all three periods between 1993 and 1995; a smaller increase occurred between 1995 and 1996 (Chi square for trend p<0.05) (Table 2). In 1996, among women who had 2--4, 5--9, and >9 prenatal care visits, 84%, 89%, and 95%, respectively, were offered ZDV prenatally. The median week for initiation of ZDV was week 20, and 14% of women were prescribed ZDV during the first trimester. ZDV was refused by 39 (5%) of 824 pregnant women, and this proportion differed little by state or by year. Women who were injection-drug users were more likely to refuse ZDV than other women (13/179 [7%] versus 17/581 [3%]; p<0.05). Of the women who were prescribed ZDV, based on chart notations, 33 (4%) of 785 stopped taking it before delivery. Overall, 14% of women received no or minimal prenatal care (0--1 prenatal care visit), and 19% initiated prenatal care in the third trimester (Table 3). The proportion of women with no or minimal prenatal care differed by state, and a lack of prenatal care was much more common among women who had used drugs during pregnancy than among women who had not used drugs during pregnancy (36% versus 5%). Differences of this magnitude were observed in six of seven states; in one state, only a small proportion of women received no prenatal care in both groups. The proportion of women receiving prenatal ZDV and the proportion who used drugs during pregnancy varied according to the number of prenatal care visits (Figure 1). The proportion of HIV-infected women (28%) who used drugs during pregnancy (based on chart notation or positive toxicologic test result) was stable over time but differed substantially among states. Among 45 women tested at or within 7 days of delivery, 71% received no or minimal prenatal care, and 67% had used drugs during pregnancy. Among 85 women tested >7 days after delivery, 27% received no or minimal prenatal care, and 26% had used drugs during pregnancy. Among women who had received no or minimal prenatal care, the proportion who had used drugs during pregnancy was 72%, 77%, and 61%, respectively, for those tested before or during pregnancy, at delivery, or later. No changes occurred from 1993 through 1996 in the proportion of deliveries that were performed by cesarean delivery or by elective cesarean delivery (before labor); in addition, no changes occurred in the proportion of women with ruptured membranes for >4 hours (Table 3). The proportion of women who had a tubal ligation during each year remained stable but was larger for women with >2 previous live births (36%) compared with women with 1 or no previous live births (25% and 13%, respectively; p<0.05). Women tested at delivery or later (n=143) were less likely to have a tubal ligation (12%; p<0.05) and more likely to have ruptured membranes for >4 hours (39%; p<0.05). Of the children who received any ZDV (prenatal, intrapartum, or neonatal), 8% were infected compared with 16% of those who did not receive ZDV (Figure 2). The rate was 12% for those for whom ZDV use was unknown, suggesting that at least some children might have received ZDV. Recommendations for Prevention In these seven states, the implementation of the guidelines to use ZDV to prevent perinatal transmission of HIV infection was rapid and has been effective at reducing perinatal HIV transmission. The large proportion of pregnant women who already had a diagnosis before delivery in 1993 undoubtedly contributed to the rapid response to the findings from PACTG 076 and the Public Health Service guidelines on ZDV use. By 1996, all except an estimated 20% of HIV-infected women had received a diagnosis before delivery. Given the large proportion of women who are treated according to recommendations and studies demonstrating that transmission can be reduced to even lower levels through the use of combination antiretroviral treatment and obstetric procedures (e.g., elective cesarean delivery) (2,7,9), eliminating perinatal HIV transmission is theoretically possible in the United States. Certain segments of the population (e.g., women who do not receive a diagnosis before or during pregnancy, women with little or no prenatal care, and women who use drugs during pregnancy), however, might not benefit from these advances. A preliminary review of data from pediatric HIV surveillance for 1997, 1998, and 1999 indicated that the levels of ZDV prescription increased from 1996 through 1997 and remained stable through 1999 (CDC, unpublished data) (10). The proportion (16%) of infected infants among those who did not receive ZDV was lower in these states than for participants in PACTG 076 (25%); characteristics of mothers (e.g., stage of illness and obstetric factors) likely played an important role. Continued increases in the proportion of women who receive effective antiretroviral therapies will be necessary to further reduce perinatal transmission and will depend on the success of efforts to increase testing, access to and use of prenatal care, and the use of rapid testing and short-course treatments for women who are first seen in labor. Because women who use drugs during pregnancy disproportionately receive inadequate or no prenatal care, targeted interventions such as community-based outreach are being implemented in 16 states to promote increased access to care and testing among pregnant women who might not otherwise receive prenatal care. In 1997, a total of 63%--87% of women in 14 states had received HIV counseling during pregnancy, and 58%--81% had been tested for HIV infection (11). Compared with 1996, increases were modest, and preliminary data from 1998 suggest that only modest increases continued (CDC, unpublished data). Surveys of health-care providers indicate that they are more likely to offer HIV testing only to women they consider at risk, although they tend to agree that all pregnant women should be tested for HIV. When providers recommend that pregnant women be tested, acceptance rates are high (12,13). Some health-care providers also consider pretest counseling according to standard practice guidelines to be a barrier to offering the test universally. The Institute of Medicine recommended the integration of HIV testing into the standard prenatal test battery and the adoption of a national policy of universal prenatal testing (4). The national policy of universal prenatal testing is described in the revised draft guidelines which a) recommend HIV testing for all pregnant women and b) affirm that informed consent is essential, including providing the patient with the right to refuse testing (4,14). A lack of prenatal care has been a long-standing problem in certain population subgroups (15) and might be a more difficult barrier to overcome, possibly becoming the leading reason for continued transmission in some geographic areas. Recent studies have demonstrated the effectiveness of short-course ZDV and single-dose nevirapine to the mother at delivery and to the neonate (16,17). As a result, evaluations are being conducted regarding the feasibility of rapid testing and the use of intrapartum antiretroviral therapy for women whose HIV status is unknown at the time of labor (18). Tubal ligation rates were high but consistent with findings from a study of contraceptive choices among HIV-infected women, which indicated that 27% of HIV-infected women chose tubal ligation compared with 15% of demographically similar women who were not infected (19). The smaller proportion of women having a tubal ligation among those who did not know their HIV status at the time of delivery is also consistent with previous findings. Enhanced pediatric surveillance methods can provide more complete data to estimate the number of HIV-infected pregnant women giving birth. In many areas, such data will be valuable as a proxy for the SCBW data, which are no longer collected but were used previously as a basis for HIV prevalence estimates in the population (20). In addition, if new HIV diagnoses in pregnant women can be assessed for recency of infection using developmental assays that can distinguish incident infections from prevalent infections, enhanced perinatal surveillance methods might contribute to development of a population-based approach to estimating HIV incidence in the United States (21). These data have several limitations. First, uncertainty regarding the number of HIV-infected women who gave birth during 1996 in most states that lacked SCBW data is a limitation. Using 1995 data as a proxy for 1996 might systematically bias the results. For example, if the number of infected women giving birth in 1996 was larger than in 1995, the calculated percentage tested would be too small or vice versa. In addition, state-level fluctuations were observed, especially in states with smaller numbers of infected women; therefore, the aggregate estimate is likely more stable than state-level estimates. Second, the proportion of infected women with a diagnosis before delivery might be an underestimate because women who had not been reported could not be included in the registry matching. Second, the proportion of infected women with a diagnosis before delivery might be an underestimate: although the completeness of HIV reporting is estimated to be >85% (22), women who had not been reported could not be included in the registry match. Third, supplemental information could be collected only on 86% of the charts eligible for review. Women whose charts were not abstracted because they were more difficult to find possibly were less likely to have received ZDV. Finally, supplemental data were incomplete for the pairs with mothers who were tested at or after delivery. Research Agenda Based on findings from this study, an important component of CDC's initiative to eliminate perinatal transmission is targeting outreach to women who use illicit drugs. The outreach is designed to increase timely access to and use of prenatal care in this population. Research to accomplish this goal includes the development of effective social marketing tools. Additional research is under way to identify effective methods of training health-care providers to increase the offering of HIV testing. Programmatic research is needed to develop effective case management methods for HIV-infected pregnant women that achieve sustained access to and use of prevention and treatment services for women and children. These efforts must include behavioral risk reduction and substance abuse treatment and prevention. Finally, for women whose HIV status is unknown at the time of labor and delivery, research is focused on developing and implementing rapid HIV testing strategies to provide antiretroviral treatment to prevent HIV transmission. CONCLUSIONTo monitor the outcomes of perinatal testing and treatment programs, enhanced perinatal surveillance is needed in all states to assess perinatal prevention needs and to monitor the effect of prevention programs (5,23). Enhanced surveillance, initially conducted in the states mentioned in this report, has recently been extended to 22 states in conjunction with a CDC initiative to eliminate perinatal transmission of HIV. The surveillance system can adapt rapidly, providing an efficient means of collecting relevant information as clinical developments occur. As the perinatal transmission of HIV continues to decrease, surveillance data will continue to play a central role in specifying the reasons for continuing transmission and in identifying the areas where transmission continues (24). AcknowledgmentsThe authors thank the following persons from the Surveillance to Evaluate Prevention (STEP) Project Group for their contributions in preparing this report: Penny Studebaker, Colorado Department of Public Health and Environment; Jean Brancazio-Pearl, Indiana State Department of Health; Karen Corson, Ph.D., Gale Terry, Louisiana Department of Health; Hollie Malamud, M.P.H., Eve Mokotoff, Michigan Department of Community Health; Linda Bell, Missouri Department of Health; Diane Abatemarco, Ph.D., John Beil, M.P.H., Linda Dimasi, M.P.A., New Jersey Department of Health; and Norma Harris, Ph.D., JoAnn Lafontaine, M.P.H., South Carolina Department of Health and Environmental Control. References
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 5/10/2001 |
|||||||||
This page last reviewed 5/10/2001
|