 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Acute Hemorrhagic Conjunctivitis Outbreak Caused by Coxsackievirus A24 --- Puerto Rico, 2003Acute hemorrhagic conjunctivitis (AHC) is an epidemic form of highly contagious conjunctivitis and is characterized by sudden onset of painful, swollen, red eyes, with conjunctival hemorrhaging and excessive tearing. Since 1981, when AHC was first detected in the Western Hemisphere (1), three major epidemics had occurred until 2003, all affecting the Caribbean. During August--October 2003, a fourth epidemic occurred in Puerto Rico (2000 population: 3.8 million). This report summarizes the outbreak investigation conducted by the Puerto Rico Department of Health (PRDOH), which documented an estimated 490,000 persons with illness, including >51,000 cases reported by physicians; demonstrated laboratory evidence of Coxsackievirus A24 (CA24); and determined that school-aged children (i.e., aged 5--18 years) and those living in crowded urban areas were at highest risk. To control outbreaks of AHC, prevention methods (e.g., frequent hand washing and avoidance of sharing towels and bedding) should be targeted to groups at highest risk, and information should be disseminated after the first report of AHC in the area. For surveillance purposes, PRDOH defines a case of AHC as physician-diagnosed conjunctivitis. To monitor the level of conjunctivitis, all health-care providers in Puerto Rico are contacted weekly to determine case counts of conjunctivitis treated during the week; providers typically report an average of 500 cases. However, in August 2003, reports of conjunctivitis increased weekly to a peak of nearly 10,000 during mid-September; reports returned to baseline in late October (Figure). During August--October 2003, health-care providers reported 51,850 cases of conjunctivitis. Conjunctival swabs were obtained from a convenience sample of affected persons from five regions. The samples were sent to CDC, where, after testing negative for bacteria, they were tested for the presence of enterovirus RNA by using a 5-prime nontranslated region reverse transcriptase polymerase chain reaction (RT-PCR) assay. For positive specimens, the enterovirus was further characterized by RT-PCR amplification of the VP1 region of the virus and genetic sequencing and then identified as CA24 by comparison with reference sequences (2,3). Of 26 conjunctival swabs tested, 20 (77%) were positive for enterovirus; of these, 19 were identified as CA24 by VP1 sequencing. The remaining six conjunctival swabs were negative for enterovirus. To further assess disease burden, identify persons at high risk, and estimate economic impact associated with this outbreak, PRDOH contacted approximately 340 households by calling randomly selected listed telephone numbers. One adult in each household was asked about the number and ages of household members with conjunctivitis. Adults also were asked about their workdays lost and use of medical services. A total of 300 (88%) households participated in the survey, representing 902 household members; 114 (13%) reported having conjunctivitis during the outbreak period. The median age of household members was 21 years (range: 1--83 years). The attack rate was higher among school-aged children than among persons aged >19 years (24% versus 10%, respectively) (relative risk [RR] = 2.42; 95% confidence interval [CI] = 1.72--3.40), among those living in urban than in rural areas (16% versus 10%, respectively; RR = 1.6; 95% CI = 1.18--2.35), and among close contacts of infected persons than among persons living alone (41% versus 6%, respectively; RR = 7.47; 95% CI = 1.92--29.12). Fifty-four (18%) households had at least one member with conjunctivitis. The attack rate was lowest for one-member households and increased with household size (correlation coefficient = 0.90; p = 0.005) (Table). Of 34 households with more than one member with conjunctivitis, 20 (59%) had an index patient who was of school age; overall, index patients were significantly younger than secondarily infected patients (median ages: 22 years versus 30 years; p = 0.034). A total of 37 adult interviewees with conjunctivitis reported illnesses lasting a median of 7 days (range: 2--14 days); 24 (65%) sought medical care from a physician, nine (64%) of 14 employed interviewees missed work (median: 3 days; range: 0--10 days), and seven (87%) of eight students missed school (median: 2 days; range 0--10 days). Based on survey data, an estimated 490,000 persons (95% CI = 403,000--570,000) had conjunctivitis during August--October 2003, resulting in a combined 850 person-years of missed work (not including missed work for child care, which was not assessed) and 315,000 visits to physicians' offices. Combined, these factors were estimated to have cost Puerto Rico $30 million in lost worker production and health-care expenses during the 3-month period. Reported by: J Alonso-Echanove, MD, Y García-Guadalupe, MPH, J Rullán, MD, Puerto Rico Dept of Health. MA Pallansch, PhD, Div of Viral and Rickettsial Diseases, National Center for Infectious Diseases; F Alvarado-Ramy, MD, Div of Applied Public Health Training, Epidemiology Program Office; B Cauthen, MD, EIS Officer, CDC. Editorial Note:Since 1981, the Caribbean islands have had four major epidemics of AHC (1,4,5), including the outbreak described in this report. During the most recent previous outbreak in 1997, approximately 40,000 cases of AHC were reported in Puerto Rico (PRDOH, unpublished data, 1997). Immunity to the infection declines considerably within 7 years (6,7), and this loss of herd immunity to the virus might have permitted the widespread transmission observed during the 2003 outbreak. The outbreak described in this report began in South America in the spring of 2003, affecting an estimated 200,000 persons in Brazil (8). The outbreak then moved into Central America and began affecting multiple islands in the Caribbean during the summer, including Puerto Rico in August (9). No states or other territories of the United States reported outbreaks of AHC during August--October 2003 and, since November, no other countries or states have reported an increase in cases. AHC typically is caused by one of two enteroviruses (CA24 or enterovirus 70). This disease is transmitted person-to-person usually through contact with contaminated hands or through sharing of contaminated personal-care items. No specific treatment is available for AHC; however, the illness is self limiting, and severe complications are rare. Nonetheless, because of its extremely contagious nature, AHC can disrupt the local economy and require substantial health-care resources. This investigation documented increased health-care use and a substantial impact on workplace productivity in Puerto Rico, as measured by physician visits and combined years of work missed. The findings in this report are subject to at least four limitations. First, the survey derives estimates for the entire island on the basis of a small survey sample, which could allow for wide variability. Second, the survey findings might not be representative of the entire population because only 76% of households in Puerto Rico have telephones, and 12% of those contacted refused to participate. Because crowding was documented in this study to be a risk for developing conjunctivitis and crowding might be more common among those not reached through a telephone survey, the total number of affected persons might have been underestimated. Third, although the households were selected randomly, the survey of individual members within the household was based on a convenience sample that might allow for some biases in the estimations. Finally, the broad case definition of conjunctivitis might have captured some noninfectious cases of conjunctivitis, resulting in an overestimation of the total number of persons affected. However, based on the large number of conjunctivitis reports relative to the baseline reporting, these noninfectious cases likely represent a small proportion. Because the majority of adults are infected as a result of infection among their school-aged children, targeting future interventions to school-aged children can help to control spread. In addition to school-aged children, other groups at high risk (e.g., persons living in crowded urban areas and household contacts of infected persons) also should be targeted for prevention messages. Recommended control measures include encouraging careful and frequent hand washing and avoiding sharing towels, bedding, makeup, and other personal items with persons with conjunctivitis. Acknowledgments This report is based on contributions by J Santiago-Ramos, MA, R Toledo-Lopez, MPH, D Andreu-Pietri, MS, S Claudio-Luciano, B Santiago-Gonzales, M Reyes-Cruz, LM Santiago-Bibiloni, MPH; Puerto Rico regional epidemiologists and nurses; Puerto Rico Dept of Health. R Moolenaar, MD, Div of Applied Public Health Training, Epidemiology Program Office; S Peñaranda, WA Nix, MS Oberste, Div of Viral and Rickettsial Diseases, National Center for Infectious Diseases, CDC. References
Table  Return to top. Figure 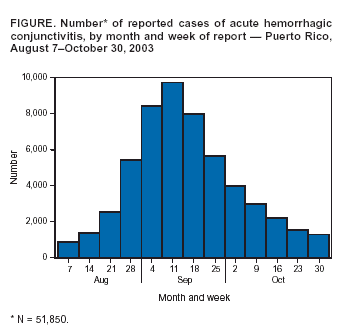 Return to top.
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 7/22/2004 |
|||||||||
This page last reviewed 7/22/2004
|