 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Update: Influenza Activity --- United States and Worldwide, 2003--04 Season, and Composition of the 2004--05 Influenza VaccineDuring the 2003--04 influenza season, influenza A (H1), A (H3N2), and B viruses co-circulated worldwide, and influenza A (H3N2) viruses predominated. Several Asian countries reported widespread outbreaks of avian influenza A (H5N1) among poultry. In Vietnam and Thailand, these outbreaks were associated with severe illnesses and deaths among humans. In the United States, the 2003--04 influenza season began earlier than most seasons, peaked in December, was moderately severe in terms of its impact on mortality, and was associated predominantly with influenza A (H3N2) viruses. This report 1) summarizes information collected by World Health Organization (WHO) and National Respiratory and Enteric Virus Surveillance System (NREVSS) collaborating laboratories, state and local health departments, health-care providers, vital statistics registries, and CDC and 2) describes influenza activity in the United States and worldwide during the 2003--04 influenza season and the composition of the 2004--05 influenza vaccine. United StatesInfluenza viruses were first isolated in Texas during outbreaks in early- to mid-October. The national percentage of respiratory specimens testing positive for influenza and the proportion of outpatient visits to sentinel physicians for influenza-like illness (ILI)* increased substantially in November and peaked in mid-December. Influenza A (H3N2) viruses were most commonly isolated, with a small number of influenza B and influenza A (H1) viruses identified. Viral Surveillance. During September 28, 2003--May 22, 2004, WHO and NREVSS collaborating laboratories in the United States tested 130,577 respiratory specimens for influenza viruses (Figure); 24,649 (18.9%) were positive. Of these, 24,393 (99.0%) were influenza A viruses, and 249 (1.0%) were influenza B viruses. Among the influenza A viruses, 7,191 (29.5%) were subtyped; 7,189 (99.9%) were influenza A (H3N2) viruses, and two (0.1%) were influenza A (H1) viruses. The proportion of specimens testing positive for influenza first increased to >10% during the week ending October 25, 2003 (week 43), peaked at 35.2% during the week ending November 29 (week 48), and declined to <10% during the week ending January 17, 2004 (week 2). The peak percentage of specimens testing positive for influenza during the previous four seasons had ranged from 23% to 31% and peaked during late December to late February (1; CDC, unpublished data, 2004). As of June 15, 2004, CDC had antigenically characterized 1,024 influenza viruses collected by U.S. laboratories since October 1, 2003: 949 influenza A (H3N2) viruses, three influenza A (H1) viruses, one influenza A (H7N2) virus, and 71 influenza B viruses. Of the 949 influenza A (H3N2) isolates characterized, 106 (11.2%) were similar antigenically to the vaccine strain A/Panama/2007/99 (H3N2), and 843 (88.8%) were similar to the drift variant, A/Fujian/411/2002 (H3N2). Of the three A (H1) isolates that were characterized, two were H1N1 viruses, and one was an H1N2 virus. The hemagglutinin proteins of the influenza A (H1) viruses were similar antigenically to the hemagglutinin of the vaccine strain A/New Caledonia/20/99. Of the 71 influenza B isolates that were characterized, 66 (93%) belonged to the B/Yamagata/16/88 lineage and were similar antigenically to B/Sichuan/379/99, and five (7%) belonged to the B/Victoria/2/87 lineage and were similar antigenically to the corresponding vaccine strain B/Hong Kong/330/2001. ILI Surveillance. The weekly percentage of patient visits to U.S. sentinel physicians for ILI exceeded baseline levels† (0--2.5%) during the weeks ending November 15, 2003--January 10, 2004 (weeks 46--1) and peaked at 7.6% during the week ending December 27, 2003 (week 52). During the previous four influenza seasons, the peak percentage of patient visits for ILI ranged from 3.3% to 7.1% and peaked during late January and February (CDC, unpublished data, 2004). State-Specific Activity Levels. Widespread influenza activity was first reported by Texas for the week ending October 18, 2003, and peaked during the week ending December 20 (week 51), when 45 states reported widespread and four states reported regional influenza activity§. No states reported widespread, regional, or local influenza activity during the weeks ending March 20--April 10, 2004 (weeks 11--14). One state reported regional activity for the weeks ending April 17, April 24, and May 8 because of nursing home outbreaks in more than two counties (weeks 15, 16, and 18). The peak number of states reporting widespread or regional activity during the previous four seasons ranged from 35 to 44 states (CDC, unpublished data, 2004). Pneumonia- and Influenza-Related Mortality. As measured by the 122 Cities Mortality Reporting System, the percentage of deaths in the United States attributed to pneumonia and influenza (P&I) exceeded the epidemic threshold¶ during 9 consecutive weeks (weeks ending December 20--February 14). The percentage of P&I deaths reached a peak of 10.3% during the weeks ending January 10--17, 2004 (weeks 1 and 2). During the previous four influenza seasons, the peak percentage of P&I deaths ranged from 8.1% to 11.2% (1; CDC, unpublished data, 2004). Pediatric Mortality. As of May 31, 2004, a total of 152 influenza-associated deaths in U.S. residents aged <18 years were reported to CDC by 40 states. All patients had influenza virus infection detected by rapid antigen testing, viral culture, or other laboratory methods. These data are provisional and subject to change as more information becomes available. WorldwideDuring October 2003--May 2004, influenza A viruses circulated widely. Influenza activity began in October, which was earlier than usual in North America and Western Europe; the reported impact was more severe than the previous three seasons. Influenza A (H3N2) viruses predominated in most countries, whereas influenza A (H1) and B viruses circulated at low levels in most parts of the world. Influenza A (H3N2) viruses predominated and were associated with outbreaks in Asia (Hong Kong and Japan), Europe (Belgium, Croatia, Denmark, Finland, France, Germany, Israel, Italy, Latvia, Norway, Portugal, Romania, the Russian Federation, Spain, Sweden, Switzerland, Ukraine, and the United Kingdom), and North America (Canada). H3N2 viruses also were reported in Africa (Algeria, Egypt, Madagascar, Morocco, and Senegal), Asia (China, India, Malaysia, the Philippines, Qatar, Republic of Korea, Saudi Arabia, Singapore, Taiwan, Thailand, and Vietnam), the Caribbean (Jamaica), Europe (Austria, Belarus, Bulgaria, Czech Republic, Greece, Hungary, Iceland, Ireland, Kyrgyzstan, the Netherlands, Poland, Serbia and Montenegro, Slovakia, and Turkey), Latin America (Argentina, Brazil, Chile, Colombia, Guyana, Nicaragua, Paraguay, Peru, and Uruguay), North America (Mexico), and Oceania (Australia, Guam, New Caledonia, and New Zealand). The majority of H3N2 viruses were similar to the A/Fujian/411/2002 drift variant. Influenza A (H1) viruses circulated at low levels in most parts of the world, and outbreaks were reported in Europe (Iceland, Ukraine, and the United Kingdom). Influenza A (H1N1) and (H1) viruses for which the neuraminidase was not characterized were isolated in Africa (Morocco and Senegal), Asia (China, Japan, Republic of Korea, Malaysia, Singapore, and Taiwan), Europe (Belarus, Denmark, France, Greece, Italy, Portugal, the Russian Federation, Sweden, and the United Kingdom), Latin America (Brazil, Chile, and Peru), and North America (Canada). Influenza A (H1N2) viruses were isolated in Africa (Senegal), Europe (France, Iceland, Norway, and Portugal), Latin America (Brazil, Chile, and Peru), and North America (Canada). Influenza B viruses were not reported in association with outbreaks but were isolated in Africa (Madagascar), Asia (China, Hong Kong, Japan, Malaysia, Republic of Korea, Taiwan, and Thailand), the Caribbean (Jamaica), Europe (Belarus, Czech Republic, Finland, France, Hungary, Ireland, Italy, Norway, the Russian Federation, Sweden, Switzerland, and the United Kingdom), Latin America (Brazil, Chile, Colombia, Panama, Paraguay, and Peru), North America (Canada and Mexico), and Oceania (Australia and Guam). Human Infections with Avian Influenza VirusesIn December 2003, one confirmed case of avian influenza A (H9N2) virus infection was reported in a child aged 5 years in Hong Kong. The child had fever, cough, and nasal discharge in late November, was hospitalized for 2 days, and fully recovered. The source of this child's H9N2 infection is unknown. During January--March 2004, a total of 34 confirmed human cases of avian influenza A (H5N1) virus infection were reported in Vietnam and Thailand. The cases were associated with severe respiratory illness requiring hospitalization and a case-fatality proportion of 68% (Vietnam: 22 cases, 15 deaths; Thailand: 12 cases, eight deaths). A substantial proportion of the cases were among children and young adults (i.e., persons aged 5--24 years). These cases were associated with widespread outbreaks of highly pathogenic** H5N1 influenza among domestic poultry. During March 2004, health authorities in Canada reported two confirmed cases of avian influenza A (H7N3) virus infection in poultry workers who were involved in culling of poultry during outbreaks of highly pathogenic H7N3 on farms in the Fraser River Valley, British Columbia. One patient had unilateral conjunctivitis and nasal discharge, and the other had unilateral conjunctivitis and headache. Both illnesses resolved without hospitalization. During the 2003--04 influenza season, a case of avian influenza A (H7N2) virus infection was detected in an adult male from New York, who was hospitalized for upper and lower respiratory tract illness in November 2003. Influenza A (H7N2) virus was isolated from a respiratory specimen from the patient, whose acute symptoms resolved. The source of this person's infection is unknown. Composition of the Influenza Vaccine for the 2004--05 SeasonOn the basis of antigenic analyses of recently isolated influenza viruses, epidemiologic data, and postvaccination serologic studies in humans, the Food and Drug Administration's Vaccines and Related Biological Products Advisory Committee (VRBPAC) recommended that the 2004--05 trivalent influenza vaccine for the United States contain A/New Caledonia/20/99-like (H1N1), A/Fujian/411/2002-like (H3N2), and B/Shanghai/361/2002-like viruses. Because of the growth properties of the A/Wyoming/3/2003 and B/Jiangsu/10/2003 viruses, U.S. vaccine manufacturers are using these antigenically equivalent strains in the vaccine as the H3N2 and B components, respectively. The A/New Caledonia/20/99 virus will be retained as the H1N1 component of the vaccine. Reported by: WHO Collaborating Center for Surveillance, Epidemiology, and Control of Influenza. T Uyeki, MD, K Teates, MPH, L Brammer, MPH, A Klimov, PhD, K Fukuda, MD, N Cox, PhD, Div of Viral and Rickettsial Diseases, National Center for Infectious Diseases, CDC. Editorial Note:During the 2003--04 influenza season, influenza activity in the United States began and peaked earlier than usual and was more severe than the previous three seasons. Moreover, a substantial number of laboratory-confirmed, influenza-associated pediatric deaths were reported in the United States. Because no similar national data were collected previously, whether this number of pediatric deaths represents a change from previous seasons is unknown. One modeling study estimated that, during 1990--1999, approximately 92 influenza-related deaths occurred annually among children aged <5 years (2). In June 2004, the Council of State and Territorial Epidemiologists (CSTE) voted to make pediatric influenza-associated deaths a nationally notifiable condition. CDC is working closely with CSTE to implement reporting. Beginning with the 2004--05 influenza season, the Advisory Committee on Immunization Practices (ACIP) recommends that all children aged 6--23 months and close contacts of children aged 0--23 months receive annual influenza vaccination (3). ACIP continues to recommend that all persons aged >6 months with certain chronic underlying medical conditions, their household contacts, and health-care workers receive annual influenza vaccination (3). As the season progressed, A/Fujian/411/2002 (H3N2) viruses, which were antigenically distinguishable from the vaccine strain A/Panama/2007/99 (H3N2), became predominant, resulting in a less than optimal match. An initial study to assess the effectiveness of the 2003--04 influenza vaccine against ILI in health-care workers did not demonstrate effectiveness (4); however, preliminary analyses of three additional unpublished studies of influenza vaccine effectiveness among children and adults in the United States were presented at the ACIP meeting on June 23, 2004, and all demonstrated vaccine effectiveness. The season also was notable because several persons were infected by avian influenza viruses. The H7N2 case associated with an illness in November 2003 is the second confirmed case of human infection with avian influenza A (H7N2) virus reported in the United States. One previous case was reported in a person involved in culling activities, when an outbreak of H7N2 occurred among turkeys and chickens at commercial farms in Virginia during 2002 (5). In both cases, no person-to-person transmission of H7N2 viruses was evident, and both persons made a full recovery from their acute respiratory illnesses. The H9N2 case identified in Hong Kong in December 2003 was the first confirmed human case since 1998 and 1999, when H9N2 infections were identified in China and Hong Kong Special Administrative Region, respectively. All H9N2 infections were associated with uncomplicated ILI, and no evidence of person-to-person transmission of H9N2 viruses has been reported (6). The two confirmed cases of avian influenza A (H7N3) virus infections identified in Canada are the first reported with this virus and were associated with an outbreak of highly pathogenic H7N3 among poultry. Both cases were in poultry workers with direct contact with H7N3-infected poultry; additional information about these cases is available at http://www.who.int/csr/don/2004_04_05/en. These patients had mild illness, were treated with oseltamivir, and fully recovered. No evidence of person-to-person transmission was identified. The 34 confirmed human cases of avian influenza A (H5N1) virus infection in Vietnam and Thailand represent the largest human outbreak of H5N1. All human cases were associated with an unprecedented, widespread, ongoing epizootic of highly pathogenic H5N1 virus affecting domestic poultry at large and small farms, live bird markets, and backyard farms in Asia. Eight Asian countries have reported H5N1 poultry outbreaks, and >100 million domestic poultry have been culled; additional information is available at http://www.oie.int/downld/avian%20influenza/a_ai-asia.htm. Confirmed human H5N1 cases had severe illness and high mortality. The majority of cases occurred during January and February among children and young adults who had direct contact with live, sick, or dead poultry (7,8). Genetic analysis of some recent human H5N1 isolates from Vietnam and Thailand revealed that all genes were of avian origin, and the isolates were resistant to amantadine and rimantadine, but susceptible to oseltamivir. No evidence of efficient person-to-person transmission of H5N1 viruses has been identified to date. During 1997, an outbreak of H5N1 resulted in 18 cases and six deaths in Hong Kong, but human-to-human transmission was rare (9). In response to the confirmed human infections with avian influenza A (H5N1) viruses, WHO activated its Pandemic Plan Phase 0, Level 2 (additional information is available at http://www.who.int/csr/resources/publications/influenza/en/whocdscsredc991.pdf); CDC issued recommendations for evaluation, reporting, laboratory testing (10), and enhanced influenza surveillance for state health departments. H5N1 poultry outbreaks have been controlled in South Korea and Japan. However, the degree to which H5N1 poultry outbreaks in Cambodia, China, Indonesia, Laos, Thailand, and Vietnam have been controlled is uncertain. For this reason, CDC continues to recommend enhanced surveillance for suspected H5N1 cases among travelers with severe unexplained respiratory illness returning from H5N1-affected countries (additional information is available at http://www.phppo.cdc.gov/han/archivesys/viewmsgv.asp?alertnum=00204). Influenza vaccine manufacturers project that approximately 90--100 million total doses of influenza vaccine will be available for distribution during the 2004--05 season in the United States. These influenza vaccine projections are preliminary and could change as the season progresses. CDC has contracted to purchase up to 8 million doses of influenza vaccine for use in the public sector, including up to 3 million doses of preservative-free vaccine for children. CDC also has received $40 million through the Vaccines for Children program to purchase approximately 4--4.5 million doses of influenza vaccine for a national stockpile, which could be made available to state and local health departments and manufacturers for distribution. Acknowledgments This report is based on data contributed by participating state and territorial epidemiologists and state public health laboratory directors, World Health Organization (WHO) collaborating laboratories, National Respiratory and Enteric Virus Surveillance System collaborating laboratories, U.S. Influenza Sentinel Provider Surveillance System. WHO National Influenza Centers, WHO Global Influenza Programme, Geneva, Switzerland. A Hay, PhD, WHO Collaborating Center for Reference and Research on Influenza, National Institute for Medical Research, London, England. I Gust, MD, A Hampson, WHO Collaborating Center for Reference and Research on Influenza, Parkville, Australia. M Tashiro, MD, WHO Collaborating Center for Reference and Research on Influenza, National Institute of Infectious Diseases, Tokyo, Japan. W Lim, PhD, Government Virus Unit, Dept of Health, Hong Kong Special Administrative Region. Fraser Health Authority, British Columbia, British Columbia Centre for Disease Control, British Columbia Ministry of Health, Health Canada. B Ostrowsky, MD, A Huang, MD, Westchester County Dept of Health, New York; M Kacica, MD, B Wallace, MD, P Smith, MD, New York State Dept of Health. Div of Public Health Surveillance and Informatics, Epidemiology Program Office; National Immunization Program, CDC. References
* Defined as temperature of >100º F (>37.8º C) and either cough or sore throat in the absence of a known cause other than influenza. § Levels of activity are 1) no activity; 2) sporadic---isolated laboratory-confirmed influenza cases or laboratory-confirmed outbreak in one institution, with no increase in activity; 3) local---increased ILI in one region, or at least two institutional outbreaks (ILI or laboratory-confirmed influenza) in one region; virus activity is no greater than sporadic in other regions; 4) regional---increased ILI activity or outbreaks (ILI or laboratory-confirmed influenza) in at least two but fewer than half of the regions in the state; and 5) widespread---increased ILI activity or outbreaks (ILI or laboratory-confirmed influenza) in at least half the regions in the state. ¶ The expected seasonal baseline proportion of P&I deaths reported by the 122 Cities Mortality Reporting System is projected by using a robust regression procedure in which a periodic regression model is applied to the observed percentage of deaths from P&I during the previous 5 years. The epidemic threshold is 1.654 standard deviations above the seasonal baseline (1). † The national baseline was calculated as the mean percentage of patient visits for ILI during noninfluenza weeks plus two standard deviations. A noninfluenza week is a week during which <10% of specimens tested positive for influenza. Wide variability in regional data precludes calculating region-specific baselines and makes it inappropriate to apply the national baseline to regional data. National and regional percentages of patient visits for ILI are weighted on the basis of state population. ** Avian influenza (AI) viruses are classified into low pathogenic (LPAI) and high pathogenic (HPAI) forms on the basis of genetic sequence and the severity of illness they cause in infected birds. The majority of AI virus strains are LPAI and typically cause little or no clinical signs in infected birds; however, some LPAI virus strains can mutate under field conditions into HPAI viruses. Additional information is available at http://www.aphis.usda.gov/lpa/issues/ai_us/ai_us.html and http://www.oie.int/eng/avian_influenza/home.htm.
Figure 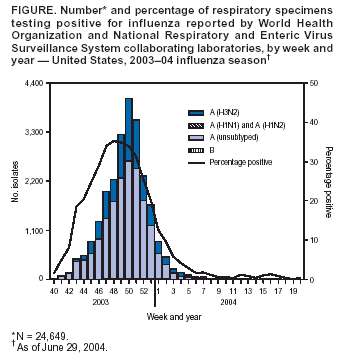 Return to top.
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 7/1/2004 |
|||||||||
This page last reviewed 7/1/2004
|