
|
|
Volume 5:
No. 3, July 2008
REVIEW
Addressing the Threat of Chronic Diseases in Oman
Jawad A. Al-Lawati, MD, MPH, Ruth Mabry, MPH, Ali Jaffer Mohammed, MD, MRCGP(I)
Suggested citation for this article: Al-Lawati JA, Mabry R, Mohammed AJ. Addressing the threat of chronic diseases in Oman. Prev Chronic Dis 2008;5(3).
http://www.cdc.gov/pcd/issues/2008/
jul/07_0086.htm. Accessed [date].
PEER REVIEWED
Abstract
Introduction
The overall health status of the Omani population has evolved over the past 4 decades from one dominated by infectious disease to one in which chronic disease poses the main challenge. Along with a marked reduction in the incidence of infectious diseases, improvements in health care and socioeconomic status have resulted in sharp declines in infant and early childhood mortality and dramatic increases in life expectancy.
Methods
Focusing on the time period from 1990 through 2005, we reviewed relevant epidemiological studies and reports and examined socioeconomic indicators to assess the impact of the changing disease profile on Oman’s economy and its health care infrastructure.
Results
Over the next 25 years, the elderly population of Oman will increase 6-fold,
and the urbanization rate is expected to reach
86%. Currently, more than 75% of the disease burden in Oman is attributable to noncommunicable diseases, with cardiovascular disease
as the leading cause of death. The distribution of chronic diseases and related risk factors
among the general population is similar to that of industrialized nations: 12% of the population has diabetes, 30% is overweight, 20% is obese, 41% has high cholesterol, and 21% has
the metabolic syndrome.
Conclusion
Unless reforms are introduced to the
current health care system, chronic diseases will constitute a major drain on Oman’s human and financial resources, threatening the advances in health and longevity achieved over the past
4 decades.
Back to top
Introduction
The rising burden of noncommunicable diseases (NCDs) has been an increasing public health concern globally. In 2005, the World Health Organization (WHO) estimated that 61% of deaths (35 million) and 49% of the global burden of disease were attributable to NCDs
(1). Eighty percent of such deaths occurred in low- and middle-income developing countries
where health resources are limited
(2). If current trends continue, by 2030 chronic diseases will account for 70% of total global deaths and 56% of
the global disease burden (1).
Oman, located in the southeastern corner of the Arabian peninsula, has a land area of 309,000 square kilometers. In 1959, the country emerged from several wars between tribal factions in the interior and coastal areas
(3). The last conflict, which took place in the south, ended in 1982 with the forging of a treaty between Oman and Yemen. Since then, the country has maintained internal peace and stability and peace with its neighbors. In 1970, Sultan Qaboos bin Said assumed power and set the
country on the path of modernization. In less than 20 years, Oman acquired all the attributes of a modern state: running water, electricity, telephone, television, shopping malls, schools, university education, hospitals, and clinics
(4).
Like many developing countries, Oman bears a high burden of NCDs. Several studies have documented the distribution of risk factors associated with NCDs in this relatively small country
(5-9). We describe the rapid changes in the epidemiologic map of Oman from one dominated by first-generation diseases (i.e., infectious diseases) to the emergence of NCDs as the dominant feature of ill health.
Furthermore, we elaborate on the accompanying demographic, socioeconomic, and behavioral
risk factor changes that have contributed to the current epidemiologic transition.
Back to top
Methods
The Directorate General of Planning of the Omani Ministry of Health
routinely collects data for health planning purposes. Data on morbidity,
mortality, and use of health care services are compiled from primary-,
secondary-, and tertiary-care regional health institutions by a Health
Information Unit, headed by a statistician, in each of Oman’s 10 administrative
regions. These data are fed into electronic templates and sent to the central
Health Information Unit. There, information is reviewed and published as an annual health report. We reviewed these reports for the years 1990
through 2005.
In addition, the Oman Ministry of Health’s Research Department
designs and conducts national health surveys every 5 to 10 years to provide
decision makers with community-based data on certain variables, including
behavioral and biological risk factors for NCDs. We reviewed the report of the
Oman National Health Survey 2000 (10), the Joint Study Report on Mortality and
Health Transitions in Oman (3), several WHO consultants’ reports on primary care in
Oman (11,12), and the 1999 World Bank Cost-Effectiveness Review of the Health Sector
(13).
We also searched the National Library of Medicine’s MEDLINE database for
publications on chronic diseases pertinent to Oman.
Although the accuracy of the
health information data gathered by the Directorate General of Planning in the
Omani Ministry of Health has not been formally assessed, health information officers from various WHO member
states in the Eastern Mediterranean Region (EMR) have visited Oman several times
to learn from its health information systems. In
addition, the International Agency for Research on Cancer, a specialized WHO
agency, has examined Oman’s cancer registry data and has considered it
sufficiently reliable to be included in its publication, Cancer Incidence in
Five Continents (http://www.iacr.com.fr/statist.htm). Oman is
1 of only 2 countries among the 22 EMR member
states whose cancer data were included.
Back to top
Results
Demographic and economic profile
The total population of Oman is estimated to be 2.5 million, of which 1.8 million are Omani citizens. Nearly 54% of Omanis are
younger than 20 years, and only 3.5% are older than 60 years. Life expectancy increased by 25 years in a period of 35 years, from 49.3 years in 1970 to 74.3 years in 2005. The current annual population growth rate is 2.2%. By 2030, the total population will double
(14). Approximately 70% of the increase will occur in the group aged 15 to 64 years. Over the same period,
the number of Omanis aged 65 and older will increase 6-fold. Urbanization has risen from 11% in 1970 to 79% in 2005 and is projected to reach 86% by 2030
(15). A rapidly growing number of Omanis are leaving arable land and labor-intensive jobs and moving to the capital city of Muscat to work in less strenuous office-based or industrial jobs. These changing trends in urbanization
(i.e., the number of people living in urban areas) and employment lead inevitably to lifestyle changes that expose the population to increased biological and behavioral
risk factors.
Partially as the result of an intense birth control campaign begun in the 1990s, the total birth rate among women aged 15 to 45 years declined by almost 50% in 10 years, from 6.0
per woman in 1995 to 3.1 per woman in 2005. The World Bank classifies Oman as an upper-middle–income developing country, and WHO stratifies it as a
country with low child and adult mortality rates. The discovery of oil in Oman in 1964 and its commercial exploitation in 1967 has led to a steady increase in per capita income from U.S. $410
in 1970 to more than U.S. $12,000 in 2005.
Control of communicable diseases
Successful interventions have prevented or controlled communicable diseases in Oman, among them, the implementation of WHO’s Expanded Programme on Immunization (EPI), improvements in living conditions and basic sanitation, and provision of free health care services to all citizens. Immunization coverage has been maintained at nearly universal levels (greater
than 95%) for all vaccine-preventable diseases within the EPI, and polio and diphtheria have not been reported in the
country since 1990. These interventions have contributed to the rapid decline in mortality rates among infants (from 118/1000 live births in
1970 to 10.3/1000 live births in 2005) and children under age 5
years (181/1000 in 1970 to 11.0/1000 in 2005) (Figure 1) (16).
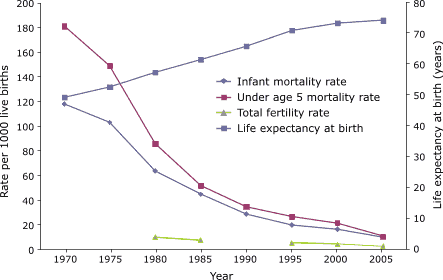
Figure 1. Trends in mortality among infants and children under age 5
years, life expectancy at birth, and total fertility rates, Oman 1970–2005
(16). Fertility data for the years 1970–1980 and 1985–1995 are not available.
[A tabular version of this figure is also
available.]
Within 11 years (1995–2005), the number of malaria cases in Oman dropped from
more than 32,000 to 544. All of the 544 cases were classified as imported cases, mostly from East Africa and the Indian subcontinent. A significant but slower decline
has occurred in the total number of cases of pulmonary tuberculosis, from 258
cases in 1985 to 131 cases in 2005 (16).
Rising tide of noncommunicable diseases
In 2002, NCDs in Oman accounted for more than 75% of hospital deaths and a similar percentage of disability-adjusted life years (DALYs) lost
(1). In 2005, 40% of inpatient and 55% of outpatient morbidity was attributed to chronic diseases, compared with 36% and 43% in 1995, an increase of 11% and 28%, respectively
(16). In 2002, cardiovascular disease (CVD) ranked first among the leading causes of death
(Figure 2) and third among causes of lost DALYs (Figure 3). The prevalence of hypertension (blood
pressure ≥140/90 mm Hg) among both sexes aged 20 years or older has risen from 27% in 1995 to 32% in 2000
(6,10).
Figure 2. Estimated deaths attributable to diseases and injuries, all ages, Oman, 2002
(17).
[A text description of this figure is also
available.]
Figure 3. Estimated disability-adjusted life years lost attributable to diseases and injuries, all ages, Oman, 2002
(17).
[A text description of this figure is also
available.]
According to the National Health Survey of 2000 (18), the prevalence of diabetes mellitus in Oman rose from 8.3% in 1991 to 11.6% in 2000 among adults aged 20 years or older. The survey, which employed identical methodology and diagnostic criteria for both years
(19), showed 7.1% of men and 5.1% of women had impaired fasting glucose. Only one-third of people with diabetes knew that they had the condition
(18). WHO estimates a 190% increase in the number of people living with diabetes in
Oman over the next 20 years, from 75,000 in 2000 to 217,000 in 2025 (20). Omanis also
have high rates of diabetes-related complications. More than 14% of people with diabetes in Oman were found to have diabetic retinopathy compared with 11.6% of Saudis and 6.7% of Indians
(21). Twenty-seven percent of Omanis with type 2 diabetes had microalbuminuria
(22). More than 50% of amputations in Oman are attributed to diabetes mellitus
(16).
Data from the National Cancer Registry show approximately 900 new cases of cancer reported annually in Oman. Malignant neoplasms are the second leading cause of death and the third cause of lost DALYs in Oman. The annual age-adjusted incidence of cancer ranges from 70 to 110 per 100,000 population. Non-Hodgkin’s lymphoma, leukemia, and gastric cancer are the most common cancers among men, and breast cancer and leukemia are the most common among women. Unlike the United States and other
parts of the world, lung cancer is only the fourth most common malignancy among men, likely because smoking was not introduced widely in Oman until after 1970.
High burden of risk factors
Although pockets of malnutrition still exist (2.2% of children under age 5
years have protein-energy malnutrition), 30% of Omani adults are overweight (body mass index [BMI] 25.0 to 29.9 kg/m2) and 20% of adults are obese (BMI ≥ 30.0 kg/m2)
(23). The rate of private car ownership is as high as 69% among Omanis (24). Data on food imports (Table) indicate an increasing trend of per capita consumption of refined sugar, dried and evaporated whole milk, chicken, cheese, and chocolate products over the past decade,
while fruit consumption has increased only slightly
(25).
The prevalence of high cholesterol (total serum cholesterol >5.2 mmol/L) was 41% in 2000
(10). Another survey of adults in the city of Nizwa in 2001 showed that more
than 35% of those surveyed had high total cholesterol, 25% had high triglyceride levels, and 77% had abnormal high-density lipoprotein
(8). The same survey indicated that 21% of adults had metabolic syndrome as defined by the National Institutes of Health Adult Treatment Panel III
(26). Similar rates of metabolic syndrome have been reported
among the U.S. adult population (27). More than 28% of adults in Nizwa reported no physical exercise during working hours, and 60% did not engage in any leisure time physical activity
(28).
Data on tobacco use show a 25% increase in per capita imports from 1993 to 2003 (Table)
(25). Currently, more than 13% of Omani adults are smokers, 13.4% of men and 0.5% of women. In the Oman component of the Global Youth Tobacco Survey (GYTS 2003), 27% of boys and 9% of girls aged 13 to 15 years were current users of some form of tobacco
(29). Waterpipe smoking is gaining popularity among youth, with 15% of boys and 3% of girls reporting this form of smoking
in 2003
(30). Curbing tobacco use has been an
important area of work for the Oman Ministry of Health, and Oman is party to the WHO Framework Convention on Tobacco Control.
To combat the surge of behavioral risk factors, a community-based demonstration project aimed at reducing NCDs and their associated risk factors was established in the city of Nizwa in 2001, and a similar project is currently underway in the eastern city of Sur. The WHO Healthy Cities Program
(31) has been under way in the eastern region of Kalhat for more than 10 years.
Within the Oman Ministry of Health there is a directorate for control of noncommunicable diseases and another for community-based initiatives, both of which address common chronic conditions such as diabetes. These agencies ensure availability of Arabic-speaking diabetes specialists in every region of Oman.
Small diabetes clinics, run by family physicians on specific days of the week, have been established in most primary health care (PHC) centers. Management guidelines to treat diabetes and
hypertension have been developed and are updated regularly.
Back to top
Discussion
The health care system of Oman faces formidable challenges in its efforts to prevent chronic diseases from eroding the achievements of the past
4 decades. First, increases in the population will lead to an estimated 210% increase in the demand for health care by 2025, and treatment of CVD alone will account for 21% of total health care expenditures
(32). Furthermore, the Omani health system currently suffers from overuse of health services, both by patients, with 5.6 visits per person
per year, and by physicians, with 70% of tests requested being unnecessary (33). Second, patients’ expectations for quality of care and better health outcomes are
increasing; continuing with the current modest standards of clinical care may erode the public’s confidence in the national health system. Third, the current rate of increase in the cost of health care is a cause of great concern for sustainability of health care services, especially given the rapid rate at
which costs are increasing. Although Oman’s per capita expenditure on health
(U.S. $220) is lower than that of neighboring Arab Gulf states (U.S. $665 in United Arab Emirates and
U.S. $539 in Bahrain) (34), health care expenditures increased by 64% from 1995 to 2005. Clearly, improving care for chronic diseases would put incrementally increased financial demands on an already resource-constrained health care system. Fourth, there is a great need to shift health care services from acute
and episodic treatment to treatment that meets the ongoing needs of people with chronic conditions, with greater focus on health promotion and chronic disease prevention.
Despite the fact that preventive health care services were emphasized in every 5-year plan of the Oman Ministry of Health, until recently health care policy makers
have focused on meeting public demand for health facilities and services by
providing curative clinical services to the newly developing regions of Oman. One positive aspect of this has been the availability of secondary-care services in all regions of Oman. Another has been the rapid expansion of
the PHC centers network throughout the country. However, the current primary care system is still geared more to combating infectious diseases, providing immunizations, and providing prenatal care rather than to meeting needs arising from the growing burden of NCDs. Most primary care physicians and nurses are not educated beyond their basic training to deal with common complex diseases like diabetes, hypertension, asthma, and psychiatric conditions. Drugs necessary to treat common conditions
such as hyperlipidemia (statins), hypertension (angiotensin-converting enzyme inhibitors), depression, and other common chronic conditions are dispensed not in primary care facilities where most people access health care, but mostly in secondary and tertiary care facilities. Antiobesity and tobacco-cessation medications have yet to be added to the
national formulary and can be obtained only through private-sector pharmacies at appreciably higher costs.
Two of the major risk factors propelling the current epidemic of NCDs, namely tobacco and obesity, can be curbed through implementation of appropriate strategies, such as the WHO Global Strategy on Diet, Physical Activity, and Health
(35). Furthermore, the call by Strong et al (2), to set a target to reduce deaths from chronic diseases by an annual rate of 2% deserves due consideration and integration into Oman’s national health goals.
Decision makers and health planners need to have greater political commitment to the provision of services for people with chronic diseases.
Commitment is most likely to be forthcoming if more evidence is produced nationally demonstrating the increasing burden of NCDs. Greater commitment to providing chronic disease services will result from national research and from continuous dialogue between advocates of chronic disease control and policy makers. Greater emphasis on health promotion will
enable people, both the chronically ill and the healthy, to increase control over their health
and to improve it.
Finally, various departments of the government make polices and decisions that inevitably have an impact on major risk factors and, ultimately, on the health of the nation. However, collaboration and joint planning among government sections are still rudimentary and need to be strengthened through development of a national planning framework under the leadership of the Ministry of National Economy. Preventive health programs would have better outcomes if public polices on taxation, trade,
food, urban planning, and the like are evidence-based and set with due consideration of public health.
Oman faces an epidemic of chronic NCDs. Oman’s rapid socioeconomic development coupled with demographic trends over the past 37 years reflects positively on Oman’s health indicators, most notably on the increase in life expectancy at birth. However, such achievements may be overshadowed by the dramatic rise of chronic diseases, including cardiovascular disease, diabetes and other obesity-associated syndromes, chronic renal failure, and cancer, which are
costly to treat. If the achievements in the health of the nation accomplished over the past
4 decades are to continue, there must be concerted efforts and coordinated policies on the part of government with greater emphasis on proven, cost-effective primary prevention services that focus on lifestyle and behavior change.
Back to top
Author Information
Corresponding Author: Jawad A. Al-Lawati, MD, MPH, Department of Non-communicable Diseases Control, Ministry of Health, P. O. Box 393, Muscat 113, Oman. Telephone: +968 2469-6187. E-mail: jallawat@yahoo.com.
Author Affiliations: Ruth Mabry, Technical Officer, World Health Organization, Country Office, Oman; Ali Jaffer Mohammed, Advisor, Directorate General of Health Affairs, Oman.
Back to top
References
- Projections of mortality and burden of disease
to 2030. Geneva (CH): World Health Organization; 2007. http://www.who.int/healthinfo/statistics/bodprojections2030/en/index.html. Accessed March
29, 2007.
- Strong K, Mathers C, Leeder S, Beaglehole R.
Preventing chronic
diseases: how many lives can we save? Lancet 2005;366(9496):1578-82.
- Hill AG, Muyeed AZ, Al-Lawati JA. The mortality and health transition in
Oman: patterns and processes. Muscat (OM): World Health Organization,
Regional Office for the Eastern Mediterranean, UNICEF Oman; 2000. http://www.unicef.org/evaldatabase/index_14179.html. Accessed March
29, 2007.
- Smith R.
Oman: leaping across the centuries. BMJ 1988;(6647):540-4.
- Asfour MG, Lambourne A, Soliman A, Al-Behlani S, Al-Asfoor D, Bold A, et
al.
High prevalence of diabetes mellitus and impaired glucose tolerance in the
Sultanate of Oman: results of the 1991 national survey. Diabet Med
1995;12(12):1122-5.
- Hassab AA, Jaffer A, Hallaj Z.
Blood pressure patterns among the Omani
population. East Mediterr Health J 1999;5(1):46-54.
- Al Riyami AA, Afifi M.
Clustering of cardiovascular risk factors among
Omani adults. East Mediterr Health J 2003;9(5-6):893-903.
- Al-Lawati JA, Mohammed AJ, Al-Hinai HQ, Jousilahti P.
Prevalence of the
metabolic syndrome among Omani adults. Diabetes Care 2003;26(6):1781-5.
- Khatib O.
Noncommunicable diseases: risk factors and regional strategies
for prevention and care. East Mediterr Health J 2004;10(6):778-88.
- Al-Riyami A, Afifi M, Al-Kharusi H, Morsi M. National Health Survey, study
of lifestyle risk factors. Muscat (OM): Ministry of Health, Research
Department; 2000.
- The first primary health care review mission report (Oman). Muscat (OM):
World Health Organization, Regional Office for the Eastern Mediterranean; 2004.
- The second primary health care review mission report (Oman). Muscat (OM):
World Health Organization, Regional Office for the Eastern Mediterranean; 2006.
- The World Bank Human Development Sector. Cost effectiveness review of
health sector. Muscat (OM): Ministry of Health; 1999.
- Demographic and social statistics.
New York (NY): United Nations Statistics Division; 2007. http://unstats.un.org/unsd/default.htm. Accessed
February 27, 2007.
- Globalis. Oman: urban population. Arendal (NO): Norwegian Ministry of
Foreign Affairs, Norwegian Agency for Development Cooperation; 2007.
http://globalis.gvu.unu.edu/indicator_detail.cfm?Country=OM&IndicatorID=30. Accessed
February 26, 2007.
- Annual health report. Muscat (OM): Directorate General of Planning; 2005.
http://www.moh.gov.om/. Accessed July 12, 2007.
- Global burden of disease statistics. Geneva (CH):
World Health Organization; 2002. http://www.who.int/evidence/bod/en/. Accessed
February 19, 2007.
- Al-Lawati JA, Al Riyami AM, Mohammed AJ, Jousilahti P.
Increasing
prevalence of diabetes mellitus in Oman. Diabet Med 2002;19(11):954-7.
- Al-Lawati JA, Mohammed AJ.
Diabetes in Oman: comparison of 1997 American Diabetes Association
classification of diabetes mellitus with 1985 WHO classification. Ann
Saudi Med 2000;20(1):12-15.
- The world health report 1997: conquering
suffering, enriching humanity. Geneva (CH): World Health Organization; 1997.
http://www.who.int/whr/1997/en/index.html.
- Khandekar R, Al Lawati J, Mohammed AJ, Al Raisi A.
Diabetic retinopathy in
Oman: a hospital based study. Br J Ophthalmol 2003;87(9):1061-4.
- Al-Futaisi A, Al-Zakwani I, Almahrezi A, Al-Hajri R, Al-Hashmi L, Al-Muniri
A, et al.
Prevalence and predictors of microalbuminuria in patients with type
2 diabetes mellitus: a cross-sectional observational study in Oman. Diabetes
Res Clin Pract 2006;72(2):212-5.
- Al-Lawati JA, Jousilahti PJ.
Prevalence and 10-year secular trend of
obesity in Oman. Saudi Med J 2004;25(3):346-51.
- Results of the family income and expenditure
survey. Muscat (OM): Ministry of National Economy; 2001. [Report in Arabic].
- Key
statistics of food and agriculture external trade. Rome (IT): Food and
Agricultural Organization of the United Nations; 2007.
http://www.fao.org/es/ess/toptrade/trade.asp?lang=EN&country=221.
- Third report of the National Cholesterol
Education Program (NCEP) expert panel on detection, evaluation, and treatment
of high blood cholesterol in adults (adult treatment panel III). Bethesda (MD): National Institutes
of Health; 2001.
- Ford ES, Giles WH, Dietz WH.
Prevalence of the metabolic syndrome among US
adults: findings from the third National Health and Nutrition Examination
Survey. JAMA 2002;287(3):356-9.
- Summary report of the Nizwa Healthy Lifestyle Project
survey 2001. Muscat (OM): Ministry of Health; 2002.
- Al Riyami AA, Afifi M.
Smoking in Oman: prevalence and characteristics of
smokers. East Mediterr Health J 2004;10(4-5):600-9.
- Helmi SA, Al-Lawati J, Al Shuaili I. Report on the results of the Global
Youth Tobacco Survey in Oman. Muscat (OM): Sultanate of Oman; 2003.
http://www.cdc.gov/tobacco/global/GYTS/reports/emro/2003/oman_report.htm.
- Healthy cities in Gulf Cooperation Council countries. Report of a consultation
Cairo, 13–16 April 2002. Muscat (OM): World Health Organization, Regional
Office for the Eastern Mediterranean; 2003. http://www.emro.who.int/cbi/pdf/CBI007.pdf.
Accessed February 19, 2007.
- Gulf Cooperation Council health care 2025. New York (NY): McKinsey &
Company; 2006.
- Abri SM, West DJ Jr, Spinelli RJ.
Managing overutilization, quality of
care, and sustainable health care outcomes in Oman. Health Care Manag
(Frederick) 2006;25(4):348-55.
- Khoja TA. Health indicators for the Council for Cooperation Council
States. No. 10. Riyadh (SA): Executive Board of the Health Ministers' Council
for GCC States; 2004. www.sgh.org.sa. Accessed June 12,
2007.
- Global strategy on diet, physical activity and
health. Geneva (CH): World Health Organization; 2007. http://www.who.int/dietphysicalactivity/en/. Accessed February
19, 2007.
Back to top
|
|
