 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Hospital Admissions Syndromic Surveillance --Connecticut, October 2001-- June 2004James L. Hadler, A. Siniscalchi, Z. Dembek Corresponding author: James L. Hadler, Infectious Diseases Division, Connecticut Department of Public Health, MS#11FDS, Hartford, CT 06134-0308. Telephone: 860-509-7995; Fax: 860-509-7910; E-mail: james.hadler@po.state.ct.us. Disclosure of relationship: The contributors of this report have disclosed that they have no financial interest, relationship, affiliation, or other association with any organization that might represent a conflict of interest. In addition, this report does not contain any discussion of unlabeled use of commercial products or products for investigational use. AbstractIntroduction: The Connecticut Department of Public Health (CDPH) has continuously monitored daily nonelective hospital admissions through a syndromic surveillance reporting system (HASS) since September 2001. Admission diagnoses are categorized into 11 syndromes including one possible indicator of smallpox, fever with rash, and one possible indicator of influenza and pneumonia. Objectives: The objectives are to describe findings from systematic investigation of individual admissions attributed to fever and rash and to determine the utility of monitoring pneumonia admissions as an indictor of severe influenza activity during the 2003--04 influenza season. Methods: The incidence of admissions for fever and rash illness was determined for a 12- month period, and results of clinical discharge diagnoses were tabulated. Excess admissions for pneumonia by week during the influenza seasons beginning 2001--03 were determined and compared. Trends in admissions from the 2003--04 season were compared with trends from laboratory and sentinel physician surveillance. Results: A total of 57 admissions for fever and rash illness were reported from 32 acute-care hospitals and verified for an incidence of 1.7 per 100,000 population. Specific clinical diagnoses were made for 29. Many were compatible with the initial clinical presentation of smallpox. Excess admissions for pneumonia during the 2003--04 season occurred concurrently with sharp increases in positive laboratory reports and percentages of visits to physician's offices attributed to influenza-like illness. The 2003--04 influenza season had many more excess admissions than the 2001--02 and 2002--03 seasons. Conclusion: HASS is a useful surveillance tool for rapid detection of sentinel cases of smallpox. Monitoring excess pneumonia admissions during the influenza season appears to be an effective and specific method for determining levels of influenza activity and for quantification of influenza-related morbidity and impact on the hospital system. IntroductionSyndromic surveillance systems are being implemented and evaluated by federal, state, and local public health jurisdictions and by academic institutions to determine their ability to detect outbreaks of illness earlier than clinician and laboratory disease-specific reporting systems and their sensitivity to detect outbreaks that might otherwise be missed (1--6). In addition, they are being explored for their possible utility to help monitor and respond to potentially large-scale events with substantial morbidity (1--3,6). In response to the September 11, 2001, World Trade Center attacks, the Connecticut Department of Public Health (DPH) initiated a hospital admissions syndromic surveillance system (HASS) to monitor for a possible concurrent biologic attack (7). The system has been continued since then with two main objectives. The first is to increase the sensitivity and timing of detection of initial cases of smallpox and severe acute respiratory disease syndrome (SARS).This objective is carried out by monitoring individual admissions with selected unusual syndromes of concern (i.e., rash illness and fever [possible smallpox] and pneumonia in a health-care worker [possible SARS]). The second objective is to have a system with readily available data to assess the magnitude and geographic distribution of severe illness requiring hospital admission brought to attention by other systems (e.g., to monitor the impact and geographical distribution of influenza; to assess whether evidence exists of wider activity if a case of anthrax were diagnosed). Among current syndromic surveillance systems, the HASS is unique in two respects. First, it is intended to detect an initial, sentinel case of smallpox before a larger outbreak occurs. Second, it monitors hospital admissions rather than outpatient visits. The objectives of this study were twofold. The first is to describe the results of investigation of persons admitted with fever and rash illness to assess the utility and workload of HASS as a tool to monitor for possible smallpox.
The second is to examine trends in hospital admissions for pneumonia during the 2003--04 influenza
season to assess the utility of the HASS as an influenza surveillance tool. The 2003--04 influenza season was unusual in that influenza activity nationally and in Connecticut appeared early, became most intense during November and December, and was largely over by
mid-January (8,9). The season also was associated with excess mortality compared with the preceding 3 seasons (9).
Statewide, each of 32 acute-care hospitals reviews unscheduled admissions for the previous 24 hours, manually categorizes them on the basis of admission diagnosis into 11 syndromes, and reports this information daily through an Internet-based reporting system to DPH. The 11 syndromes include fever with rash and pneumonia. The public health response to the data received has several steps. First, active follow-up begins the day of report of admissions for rash illness and fever to determine the course of illness, evolving differential diagnosis, and whether testing is needed to rule out smallpox. Second, data is reviewed daily to weekly by syndrome to determine unusual levels of activity. Finally, a comprehensive review is conducted if issues are unresolved (e.g., examination of trends in pneumonia admissions during the influenza season to determine how long they remain elevated. To describe the experience with fever and rash illness, admission and follow-up data were reviewed for the 12-month period, July 2003--June 2004. The number of cases and incidence overall and by county were determined. The results of verification of cases as to whether they presented with both fever and rash and the final clinical diagnoses and their potential to mimic the typical clinical presentation of smallpox are described. To examine the utility of the HASS for monitoring influenza, weekly totals of admissions for pneumonia were examined for the state and three largest counties (each with 800,000--900,000
persons representing 77% of the state's population) for temporal trends during November 2003-March 2004. In addition, findings were compared with the weekly results from two other influenza monitoring systems operating at the same time and to weekly results of pneumonia admissions for the preceding 2 years for HASS. The two additional influenza surveillance systems in use included
required reporting to DPH of the results of all positive laboratory tests for influenza and a sentinel physician surveillance system in which volunteer physicians reported daily the total number of visits and the percentage attributed to influenza-like illness (ILI, defined
as temperature of >100°F [>38°C]) and either a cough or a sore throat. Finally, the burden of excess admissions for pneumonia each week and overall were tallied and compared over the 3 years. Excess admissions were
defined as the number of admissions for pneumonia above the annual weekly average.
Overall, 78 cases of fever and rash illness were reported from 32 hospitals in HASS. Of these, 57 were verified as fever with rash. Cases excluded usually had either fever or rash, but not both. The 12-month incidence was 1.7 per 100,000 population. The county-specific incidence for the three largest counties was consistent, ranging from 1.5--1.7. The incidence in the five smaller counties was wider, ranging from 0.8-3.5, with each having no more than 2--4 cases. By the time patients were discharged, 29 (51%) had a specific clinical diagnosis (Table 1). The most common diagnoses were drug hypersensitivity (11%), varicella (7%), and urticaria (4%). Cases were
diagnosed in which the initial presentation was similar to that of smallpox (e.g., fever with diffuse undifferentiated rash).
Throughout the 3 years, the average number of weekly admissions for pneumonia reported through the HASS was 305. For both the 2001--02 and 2002--03 influenza seasons, pneumonia admissions peaked in early January and then continued to be much higher than average either continuously (2001--02) or intermittently (2002--03) through most of February, with a decline to near baseline by early March (Figure 1). This pattern paralleled known influenza activity for these years (10), although it is unclear how many of the admissions were influenza-related. For the 2003--04 influenza season, the pattern was different and was characterized by a sharp increase in mid-December to a peak in early January that was much higher than peaks in either of the two preceding years, then a rapid decline to near baseline. The pattern for each of the three largest counties was similar to the overall pattern for all 3 seasons. On the basis of findings from two influenza surveillance systems and excess hospital admissions for the 2003-2004 influenza season, both the number of laboratory reports positive for influenza and the percentage of acute office visits due to ILI show increasing activity beginning in mid-November, followed by sharp increases in mid-December and peaks in late December (Figure 2). Activity then fell nearly as sharply as it rose in both systems. The excess number of pneumonia admissions paralleled the activity of these influenza-specific systems with a slight lag in reaching its peak and a more rapid return to baseline. For the 2003--04 season during the weeks of peak activity, approximately 350 extra pneumonia admissions
were reported per week, an index of surge capacity needed by hospitals (Figure 3). In addition, the 2003--04 influenza season
put an unusual seasonal stress on hospitals compared with the preceding two seasons.
Syndromic surveillance systems have attracted the interest of public health officials and academia, particularly in the context of monitoring for biologic terrorism (1,11,12). In the absence of specific biologic terrorism events since the anthrax attacks of 2001, the sensitivity and timeliness of syndromic surveillance to detect biologic terrorism events compared with clinician and laboratory reporting systems have not been determined. The sustainability of syndromic surveillance systems will depend on whether their cost is worth their usefulness. If there are no biologic terrorism attacks, sustainable syndromic surveillance systems for biologic terrorism will have to have added value to the clinician and laboratory reporting systems or have demonstrated alternative utility. On the basis of this analyses, HASS has demonstrated utility in monitoring for smallpox and has distinct added benefits to other forms of influenza surveillance. The initial manifestations of smallpox in a nonimmune person will probably be severe (i.e., prostrating febrile illness with generalized nondescript rash). The rash will not evolve to a more characteristic form for up to a week, but the severity of the initial febrile illness probably will result in a medical visit and hospital admission for observation and supportive treatment. On the basis of the diagnoses of the 57 cases described in this report, HASS clearly detects such serious febrile rash illness. Reports to HASS are timely because they occur the day after admission and enable immediate follow-up by public health epidemiologists even before a clinician is likely to suspect smallpox. In addition, HASS detects single cases and can assure that each is evaluated for possible smallpox. Although completeness of reporting was not formally measured, the even geographic distribution of fever and rash admissions suggests reporting might be relatively complete. In addition, HASS is an enhancement to clinician reporting of suspected smallpox. Although it identified 57 suspect cases, only two cases of illness were reported to DPH as possible smallpox during this period. One was an inpatient also detected by this system and found to have viral exanthem, and the other was an outpatient with chickenpox. Finally, the amount of epidemiology staff work for follow-up of each reported case is readily manageable, averaging about 4 hours for initial hospital contact and follow-up calls. Most of the time is spent making initial contact with the hospital and the managing physician. The 2003--04 influenza season provided an opportunity to examine the utility of HASS as an influenza monitoring tool. The findings of this report indicate that nearly all excess hospital admissions for pneumonia during the fall and winter of 2003--2004 were related to influenza. Nearly all excess activity occurred during November and December. No sustained excess pneumonia activity was reported after early January when winter respiratory disease, including influenza, is usually expected. On the basis of this experience, it is reasonable to assume that most excess severe pneumonia activity during any fall-winter season is most likely related to influenza. Other notable characteristics of HASS as an influenza surveillance tool are that it appears to be sensitive to high levels of influenza activity, and it provides a timely measure of the changing and overall burden influenza puts on hospitals. Finally, HASS provides data for assessing the overall severity of an influenza season. Connecticut intends to use HASS data prospectively throughout future influenza seasons to determine when the influenza season becomes severe (continuing and sustained increase in excess pneumonia admissions), when it peaks (continuing decrease in excess admissions) and its overall impact. HASS is meeting the objective to provide a context to evaluate levels of severe disease activity by syndrome, at least for pneumonia and in the context of influenza. Because of concerns about pandemic influenza and about hospital surge capacity, this system should continue to be worth the cost of operation. Although data collection is largely manual, it is simple, requiring <15 minutes per hospital per day. The Connecticut HASS is a unique surveillance system in the United States. CDC's Biosense system and most state and local health departments that have such systems are conducting syndromic surveillance on the basis of outpatient visits with a primary objective to identify outbreaks earlier. Limitations of HASS include its inability to detect predominantly outpatient outbreaks of illness and a lag time of one or more days between initial patient presentation to the health care system and admission to the hospital. However, the latter limitation might not be of as much practical impact as it is in theory. Users of outpatient syndromic surveillance systems are finding that it is very difficult to effectively set thresholds to identify levels of disease activity that merit full investigation, and that investigation of all but the largest sustained signals is very labor intensive and has little added value in the absence of a biologic terrorism attack (1,2). As a result, increases in syndrome-specific visits are monitored for one or more days to determine if they are sustained before initiating an investigation. In addition, these outpatient systems are limited in their ability to facilitate follow-up of individual cases. Furthermore, although outpatient systems have the potential to enable monitoring for the outpatient burden of influenza, numbers of outpatient visits do not directly measure the burden of severe illness. A hospital admission-based system such as that in Connecticut is of sufficient value relative to its cost that it should be tried and evaluated elsewhere. HASS might be of more practical longterm utility in meeting some biologic terrorism and public health preparedness surveillance objectives than syndromic surveillance systems that focus on outpatient visits. Acknowledgments The authors acknowledge Stephanie Petrahai and Albert DeLoreto for maintaining the influenza laboratory reporting database and sentinel physician influenza surveillance system respectively during 2003--04 influenza season, and Kenneth Carley for his assistance
with analysis of HASS data. In addition, we are indebted to the designated reporters to HASS at each of the 32 acute-care hospitals in Connecticut for their daily efforts to report and assist with follow-up of persons admitted with febrile rash illness.
Table 1 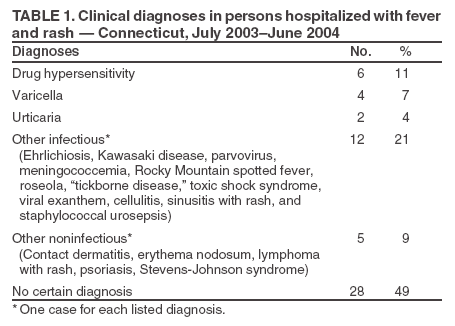 Return to top. Figure 1 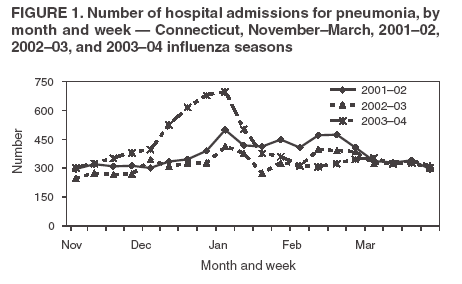 Return to top. Figure 2 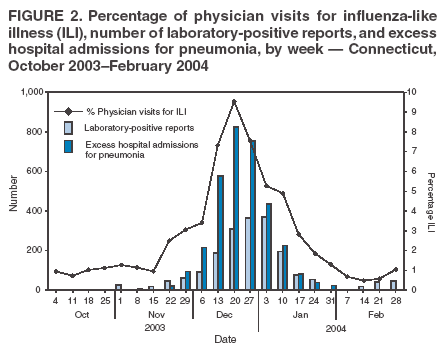 Return to top. Figure 3 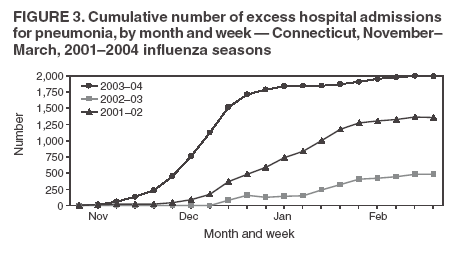 Return to top.
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Date last reviewed: 8/5/2005 |
|||||||||
|