|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Hospital Admissions Syndromic Surveillance --- Connecticut, September 2001--November 2003Zygmunt F. Dembek, K. Carley, A. Siniscalchi, J. Hadler
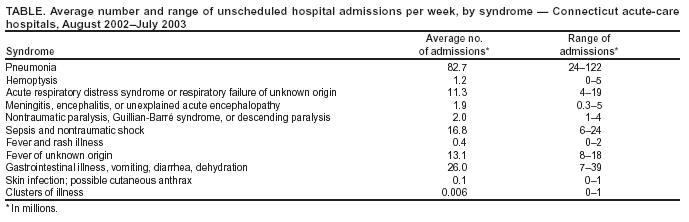
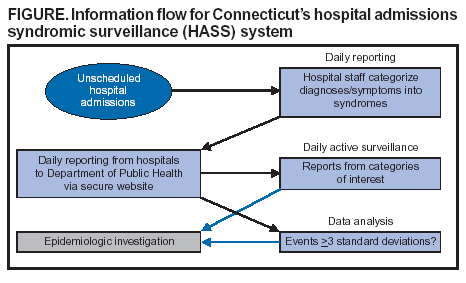
Corresponding author: Zygmunt F. Dembek, Epidemiology Program, Connecticut Department of Public Health, 410 Capitol Ave., MS # 11EPI, P.O. Box 340308, Hartford, CT 06134-0308. Telephone: 860-509-7994; Fax: 860-509-7910; E-mail: zygmunt.dembek@po.state.ct.us. AbstractOn September 11, 2001, the Connecticut Department of Public Health (CDPH) initiated daily, statewide syndromic surveillance based on unscheduled hospital admissions (HASS). The system's objectives were to monitor for outbreaks caused by Category A biologic agents and evaluate limits in space and time of identified outbreaks. Thirty-two acute-care hospitals were required to report their previous day's unscheduled admissions for 11 syndromes (pneumonia, hemoptysis, respiratory distress, acute neurologic illness, nontraumatic paralysis, sepsis and nontraumatic shock, fever with rash, fever of unknown cause, acute gastrointestinal illness, and possible cutaneous anthrax, and suspected illness clusters). Admissions for pneumonia, gastrointestinal illness, and sepsis were reported most frequently; admissions for fever with rash, possible cutaneous anthrax, and hemoptysis were rare. A method for determining the difference between random and systemic variation was used to identify differences of >3 standard deviations for each syndrome from a 6-month moving average. HASS was adapted to meet changing surveillance needs (e.g., surveillance for anthrax, smallpox, and severe acute respiratory syndrome). HASS was sensitive enough to reflect annual increases in hospital-admission rates for pneumonia during the influenza season and to confirm an outbreak of gastrointestinal illness. Follow-up of HASS neurologic-admissions reports has led to diagnosis of West Nile virus encephalitis cases. Report validation, syndrome-criteria standardization among hospitals, and expanded use of outbreak-detection algorithms will enhance the system's usefulness. IntroductionOn September 11, 2001, the Connecticut Department of Public Health (CDPH) developed and initiated a syndromic surveillance system based on unscheduled hospital admissions called HASS. The system's initial objective was to monitor for a concurrent terrorist event caused by Category A biologic agents (1,2). All hospitals were required to submit standardized reports to CDPH regarding the number of patients admitted the previous day with acute respiratory or neurologic problems and perceived illness clusters among newly admitted patients. Another objective was to evaluate the spatio-temporal limits of identified outbreaks and other public health threats. MethodsHASS DescriptionAll 32 acute-care hospitals within Connecticut are required to report to CDPH on a standardized form the number of unscheduled admissions from the previous day. Reporting is required for 11 syndromic categories, including pneumonia, with a subcategory for health-care workers with clinical responsibilities; hemoptysis; respiratory distress syndrome, with a subcategory for health-care workers with clinical responsibilities; acute neurologic illness, including meningitis, encephalitis, or unexplained acute encephalopathy; nontraumatic paralysis; nontraumatic shock, including sepsis; fever with rash; fever of unknown cause; acute gastrointestinal illness, including vomiting, diarrhea, or dehydration; skin infection indicating possible anthrax; and apparent illness clusters. HASS has been modified to meet changing disease surveillance needs as follows:
Initially, hospitals reported to CDPH by fax or e-mail. In May 2003, a secure website with the report form was inaugurated. Since October 2003, all 32 acute-care hospitals have reported their data by using the secure website. Each hospital has access to its data on the website. CDPH investigates all detected or reported disease clusters and all cases of selected syndromes. Case follow-up is routine for the following syndromic categories:
AnalysisThe HASS data set is transformed into an Excel™ spreadsheet and analyzed with SAS® for Windows™ Version 8e (3) by using the Shewhart method (4) of analysis to determine the difference between random and systemic variation. A 3-standard-- deviation difference (i.e., statistically significant) is calculated by using a 6-month moving average of all data collected. This analysis is performed for each syndrome for all hospitals combined and for hospitals in each of the three largest of Connecticut's eight counties (Figure). A CDPH epidemiologist inspects data daily. Analysis is conducted weekly, whenever a peak in rates is noted, whenever disease-surveillance questions occur (e.g., when an outbreak is detected through routine reporting mechanisms), after unusual events (e.g., the August 2003 electrical blackout), or when determining whether influenza activity has increased. System ExperienceDuring August 2002--July 2003, unscheduled admissions were reported most frequently for pneumonia (an average of 82.7 admissions/million population/week), followed by acute gastrointestinal illness (26.0), sepsis and nontraumatic shock (16.8), fever of unknown origin (13.1), and respiratory distress (11.3) (Table). Syndromes reported least commonly were disease clusters (0.006), possible cutaneous anthrax (0.1), fever and rash illness (0.4), and hemoptysis (1.2). No significant difference was found by day of the week for admission rates for the most frequent syndromic categories. During August 2002--July 2003, a total of 59 spikes in activity >3s were noted. All spikes were detected from county-specific (not statewide) analysis. By syndrome category, all were either gastrointestinal (35) or pneumonia (24). All gastrointestinal spikes were limited, single-day events. With one exception (a January 2002 1-day spike correlated with a norovirus outbreak affecting 116 persons), no spikes were associated with known gastrointestinal outbreaks. Spikes in pneumonia clustered during the winter months and were likely caused by seasonal influenza. During November 2002--November 2003, a total of 58 cases of fever and rash illness were reported and subsequently investigated to rule out smallpox. These cases had other diagnoses, including viral syndrome, serum sickness, meningococcemia, pustular psoriasis, uticaria, toxic shock syndrome, scarlet fever, tickborne disease, staphylococcal infection, parvovirus, human immunodeficiency virus infection, and chickenpox. During May--November 2003, two cases of acute respiratory distress and nine cases of pneumonia among health-care workers with clinical responsibilities were reported to HASS and investigated. None met then-current CDC or World Health Organization criteria for suspected SARS (5). Individual hospitals have reported four illness clusters since HASS's inception, all gastrointestinal illness of unknown etiology. Laboratory-based surveillance detected 15 different gastrointestinal illness clusters. No increase in gastrointestinal illness was observed in Connecticut hospitals serving those areas affected by the Northeast power blackout during or after August 14--15, 2003. A health director who regularly monitored HASS data in his municipality discovered the first two of Connecticut's 17 confirmed human West Nile virus cases during 2002. He requested investigation of two late-summer neurologic syndrome reports. Both patients had encephalitis and subsequently tested positive for West Nile virus infection. DiscussionCDPH chose to design and implement a system based on hospital admissions for multiple reasons. Hospital admissions measure severe illness; the biologic agents of greatest concern (Category A) all cause illness severe enough to require hospitalization. Obtaining additional clinical, follow-up, and laboratory information on these patients is possible because they are hospitalized in a known place and are monitored. HASS is easy and inexpensive to implement and modify, requiring no special computer equipment or programming and 10--15 minutes/day for most hospitals to review the previous day's admissions and prepare and submit data. It can be readily implemented statewide, a desirable feature in a state with discrete population centers (compared with a densely populated area such as New York City). HASS requires someone at each hospital to be aware of admission patterns, increasing the potential to recognize and report unusual events. Finally, unlike systems based on outpatient visits, HASS enables detection and investigation of outbreaks as limited as a single case (e.g., smallpox or SARS). Baseline information is now available on the frequency of admissions for a range of syndromes. The system is sensitive enough to reflect important community events (e.g., concurrent increases in a monitored syndrome in city or county hospitals). A sizable laboratory-reported gastrointestinal outbreak was also evident with HASS. Admission rates for pneumonia have been observed to vary by season and increase markedly during an active influenza season. CDPH has increased confidence that HASS can be used for statewide surveillance and to monitor an outbreak that results in hospitalizations. HASS has been used successfully to identify and rapidly investigate individual cases of relatively unusual syndromes (e.g., the detection of two cases of West Nile virus encephalitis by following up on reports of encephalitis in one hospital). Investigation of cases of fever with rash has identified chickenpox. Continued investigation of admissions for fever and rash illness is a reasonable way to conduct enhanced smallpox surveillance. HASS has important limitations. First, it is insensitive to slight changes in the syndromes most frequently reported (i.e., pneumonia, gastrointestinal illness, and sepsis). Second, HASS has yet to detect an outbreak not also detected by other means. Third, it is insensitive to outbreaks that primarily produce outpatient illness. Fourth, because it depends on patient admissions, identifying an outbreak with a time lag between symptom onset and admission (e.g., anthrax) can be delayed by 1--2 days when compared with an outpatient syndromic surveillance system. Finally, because HASS obtains only case counts rather than individual demographic data, increases in illness among a demographic subset of the population (e.g., children or women) cannot be detected without obtaining additional information. References
|
|||||||||
This page last reviewed 9/14/2004
|