 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Prevalence of Selected Risk Behaviors and Chronic Diseases --- Behavioral Risk Factor Surveillance System (BRFSS), 39 Steps Communities, United States, 2005Fred Ramsey, MS1
Corresponding author: Ann Ussery-Hall, MPH, Division of Adult and Community Health, National Center for Chronic Disease Prevention and Health Promotion, CDC, 4770 Buford Hwy, N.E., MS K-93, Atlanta, GA 3041-3717. Telephone: 770-488-8636; Fax: 770-488-8488; E-mail: aussery@cdc.gov. AbstractProblem: Behavioral risk factors (e.g., tobacco use, poor diet, and physical inactivity) can lead to chronic diseases. In 2005, of the 10 leading causes of death in the United States, seven (heart disease, cancer, stroke, chronic lower respiratory diseases, diabetes, Alzheimer's disease, and kidney disease) were attributable to chronic disease. Chronic diseases also adversely affect the quality of life of an estimated 90 million persons in the United States, resulting in illness, disability, extended pain and suffering, and major limitations in daily living. Reporting Period Covered: 2005. Description of the System: CDC's Steps Program funds 40 selected U.S. communities to address six leading causes of death and disability and rising health-care costs in the United States: obesity, diabetes, asthma, physical inactivity, poor nutrition, and tobacco use. In 2005, a total of 39 Steps communities conducted a survey to collect adult health outcome data. The survey instrument was a modified version of the Behavioral Risk Factor Surveillance System (BRFSS) survey, a community-based, random-digit--dialing telephone survey with a multistage cluster design. The survey instrument collected information on health risk behaviors and preventive health practices among noninstitutionalized adults aged >18 years. Results: Prevalence estimates of risk behaviors and chronic conditions varied among the 39 Steps communities that reported data for 2005. The proportion of the population that achieved Healthy People 2010 (HP 2010) objectives also varied among the communities. The estimated prevalence of obesity (defined as having a body mass index [BMI] of >30.0 kg/m² as calculated from self-reported weight and height) ranged from 15.6% to 44.0%. No communities reached the HP2010 objective of reducing the proportion of adults who are obese to 15.0%. The prevalence of diagnosed diabetes (excluding gestational diabetes) ranged from 4.3% to 16.6%. Eighteen communities achieved the HP2010 objective to increase the proportion of adults with diabetes who have at least an annual foot examination to 75.0%; five communities achieved the HP2010 objective to increase the proportion of adults with diabetes who have an annual dilated eye examination to 75.0%. The prevalence of reported asthma ranged from 7.0% to 17.6%. Among those who reported having asthma, the prevalence of having no symptoms of asthma during the preceding 30 days ranged from 15.4% to 40.3% for 10 communities with sufficient data for estimates. The prevalence of respondents who engaged in moderate physical activity for >30 minutes at least five times a week or who reported vigorous physical activity for >20 minutes at least three times a week ranged from 42.0% to 62.2%. The prevalence of consumption of fruits and vegetables at least five times a day ranged from 15.6% to 30.3%. The estimated prevalence among respondents aged >18 years who reported having smoked >100 cigarettes in their lifetime and who were current smokers on every day or some days at the time of the survey ranged from 11.0% to 39.7%. One community achieved the HP2010 objective to reduce the proportion of adults who smoke to 12.0%. Among smokers, the prevalence of having stopped smoking for >1 day as a result of trying to quit smoking during the previous 12 months ranged from 47.8% to 63.3% for 31 communities. No communities reached the HP2010 objective of increasing smoking cessation attempts by adult smokers to 75%. Interpretation: The findings in this report indicate variations in health risk behaviors, chronic conditions, and use of preventive health screenings and health services. These findings underscore the continued need to evaluate intervention programs at the community level and to design and implement policies to reduce morbidity and mortality caused by chronic disease. Public Health Action: Steps BRFSS data can be used to monitor the prevalence of specific health behaviors, diseases, conditions, and use of preventive health services. Steps Program staff at the national, state, local, and tribal levels can use BRFSS data to demonstrate accountability to stakeholders, monitor progress in meeting program objectives, focus programs on activities with the greatest promise of results, identify opportunities for strategic collaboration, and identify and disseminate successes and lessons learned. IntroductionBehavioral risk factors (e.g., tobacco use, poor diet, and physical inactivity) can lead to chronic diseases (e.g., diabetes, asthma, and obesity) (1). In 2005, of the 10 leading causes of death in the United States, seven (heart disease, cancer, stroke, chronic lower respiratory diseases, diabetes, Alzheimer's disease, and kidney disease) were attributable to chronic diseases, and chronic diseases affect the quality of life of an estimated 90 million U.S. residents (2). The estimated direct and indirect annual costs of diabetes, asthma, and obesity are $132 billion for diabetes (2,3), $16.1 billion for asthma (4), and $118 billion for obesity (5). Diabetes, asthma, and obesity largely can be prevented and controlled through the modification of certain interrelated risk behaviors (e.g., exercising regularly, eating a healthy diet, and avoiding tobacco use and exposure). To respond to the chronic disease burden, CDC's Steps Program uses a population-based approach that addresses multiple determinants of health. Key elements of this approach include implementing evidence-based interventions, responding to community needs, reaching diverse population groups, working across multiple sectors (e.g., schools, work sites, health care, and the community), and creating nontraditional partnerships (e.g., with transportation and cooperative extension services). All of these elements serve to accelerate positive health changes in communities and reduce chronic disease. CDC's Steps Program operates a cooperative agreement that provides funding to 40 communities nationwide to support evidence-based community interventions. Interventions focus on six priority areas, comprising three health conditions or diseases (obesity, diabetes, and asthma) and three related risk behaviors (physical inactivity, poor nutrition, and tobacco use). Communities were selected as part of a Request for Funding announcement (RFA) designed to ensure inclusion of populations disproportionately affected by chronic disease and associated risk factors; inclusion of geographic areas with high age-adjusted rates of chronic disease and associated risk factors; geographic distribution of Steps programs nationwide; and inclusion of communities of varying sizes, including rural, suburban, and urban communities. Steps sites include small cities and rural communities (with sites coordinated at the state level), large cities and urban communities, and tribal communities. As part of the RFA, grantees participate in the Steps Behavioral Risk Factor Surveillance System (BRFSS) to collect data on health conditions and diseases and on related risk factors at the community level and track Steps Program health outcomes and behaviors over time. This report provides baseline data for Steps communities; additional years of data will be used to make community to community, national, and HP2010 comparisons. Data are reported for 39 Steps communities* that reported data for 2005 on the six priority areas. MethodsThe Steps BRFSS survey instrument is a modified version of the 2005 BRFSS national survey and includes standardized questions related to the three Steps-specific disease outcomes (diabetes, asthma, and obesity) and the three related risk factors (physical inactivity, poor nutrition, and tobacco use). A multistage cluster design based on random-digit--dialing methods was used to select a representative sample of the civilian, noninstitutionalized population aged >18 years. To ensure coordinated efforts and efficient use of resources, 39 Steps communities used BRFSS infrastructure and capacity already in place at the national, state, and local levels to collect data. The survey instrument included standard 2005 BRFSS questions (available at http://www.cdc.gov/brfss) related to the six priority areas. Data collection procedures or processes varied by community because of each community's particular characteristics. For example, certain Steps communities conducted a stand-alone survey whereas others coordinated data collection with the state or local BRFSS. Several Steps communities adapted their data collection methods to respond to local cultural needs. For the majority of Steps communities, CDC provided technical assistance, data cleaning, weighting, and analysis of surveillance data. Questionnaire The 2005 Steps BRFSS questionnaire comprised three parts: 1) core questions, 2) optional supplemental modules containing sets of questions on specific topics (e.g., diabetes, health-related-quality of life, and arthritis management), and 3) state-added questions. The 2005 Steps BRFSS questionnaire asked core and optional questions related to risk factors associated with obesity, diabetes, and asthma and the accompanying underlying risk factors of physical inactivity, poor nutrition, and tobacco use. Questions from the following Core Sections of the 2005 BRFSS National Survey were used: Healthy Days, Health Care Access, Diabetes, Asthma, Tobacco Use, Demographics, Fruits, Vegetables, and Physical Activity. In addition, certain questions from the following Optional Modules were part of the survey: Diabetes Self-Management, Adult Asthma History, and Smoking Cessation. Additional information about the national BRFSS standard questions is available at http://www.cdc.gov/brfss/questionnaires. Data Collection and Processing A total of 39 Steps communities* collected data in 2005 using trained interviewers to administer the survey via a computer-assisted telephone interviewing (CATI) system; 30 communities forwarded their data to CDC for data reliability checks and preparation for analyses, and nine communities conducted individual analyses and reported the results to CDC. Six of the nine communities that conducted their own analysis sent weighted data to CDC to produce estimates. For each community, data were collected either monthly or at a single point in time. Data Weighting and Analysis Upon completion of data collection, 30 communities submitted data to CDC, which edited and aggregated the data files to create a sample for each community. For this analysis, each sample was weighted to the respondent's probability of selection and to the age- and sex-specific population or to the age-, sex-, and race-specific population data, using current population estimates provided by the community or 2005 intercensal estimates provided by Claritas, Inc. (San Diego, California), a private data vendor that uses census projections as part of its process for developing yearly population estimates. These sampling weights then were used to calculate community-level prevalence estimates. Detailed weighting and analytic methodologies used for BRFSS have been documented previously (6). Statistical Analyses SAS® (release 9.1.3) and SUDAAN® were used in the analyses to account for the complex sampling design and to calculate prevalence estimates, standard errors, and 95% confidence intervals (CIs) (7,8). Statistics for selected communities were reported as "not available" if the unweighted sample size for the denominator was <50 or the CI half width was >10. Because those data are not included in this report, the number of communities represented for each indicator varies (range: 20--39). Data Presented The tables in this report contain the weighted percentage, sample size, standard error, and CIs. Data for three of the communities that conducted their own data analysis are reported without standard errors. Standard errors are reported for the six communities that conducted their own data analysis and sent their data to CDC to produce estimates from the weighted data set that they provided. When comparable, national BRFSS median prevalence estimates and Healthy People 2010 (HP2010) goals are presented (9,10). National prevalence estimates are not available for questions from BRFSS optional modules. For several questions, comparative HP2010 goals are not available because the results cannot be compared with the BRFSS indicators. ResultsOverweight and Obesity Prevalence of Overweight and Obesity Among Adults Aged >18 Years Self-reported weight and height were used to calculate body mass index (BMI) (weight [kg]/height [m2]). Being overweight or obese was defined as having a BMI of >25.0 kg/m2; obesity alone was classified as BMI of >30.0 kg/m2. The estimated prevalence of respondents aged >18 years being overweight or obese ranged from 35.4% (95% CI = 33.0--37.9) in Cleveland, Ohio, to 75.5% (95% CI = 64.7--83.9) in Colville Confederated Tribes, Washington (median: 60.8%) (Table 1). The 2005 nationwide BRFSS median was 61.3%; this median was exceeded by 19 Steps communities. Prevalence of Obesity Among Adults Aged >18 Years Overall, the estimated prevalence of obesity (BMI >30.0 kg/m2) among respondents aged >18 years ranged from 15.6% (95% CI = 13.5--17.6) in Teller County, Colorado, to 44.0% (95% CI = 36.3--51.6) in Inter-Tribal Council, Michigan (median: 24.6%) (Table 2). The HP2010 objective is to reduce the proportion of adults who are obese to 15.0%. The 2005 nationwide BRFSS median was 24.4%; this median was exceeded by 20 communities, and no communities achieved the HP2010 objective† (objective no. 19.2) to reduce the proportion of adults who are obese to 15.0%. Diabetes Overall Rate of Diabetes Overall, the estimated prevalence of diabetes among respondents aged >18 years who reported ever having been told by a doctor that they have diabetes (other than during pregnancy) ranged from 4.3% (95% CI = 2.4--6.2) in St. Paul-Ramsey County, Minnesota, to 16.6% (95% CI = 10.1--23.1) in Inter-Tribal Council, Michigan (median: 8.1%) (Table 3). The nationwide 2005 BRFSS median was 7.3%; this median was exceeded by 25 Steps communities. Foot Examination Among Adults Aged >18 Years with Diabetes Among 25 Steps communities, the estimated prevalence among respondents aged >18 years who reported having ever been told by a doctor that they have diabetes (excluding women who were told only when pregnant) and who reported having a clinical foot examination during the preceding 12 months ranged from 60.4% (95% CI = 50.8--70.0) in Santa Clara County, California, to 93.6% (95% CI = 88.7--98.6) in Inter-Tribal Council, Michigan (median: 79.7%) (Table 4). The HP2010 objective (objective no. 5-14) is to increase the proportion of adults with diabetes who have at least an annual foot examination to 75.0%. Dilated Eye Examination Among Adults Aged >18 Years with Diabetes Among 21 Steps communities, the estimated prevalence among respondents aged >18 years who reported having ever been told by a doctor that they have diabetes (excluding women who were told only when pregnant) and who reported having received a dilated eye examination during the preceding 12 months ranged from 63.2% (95% CI = 53.5--72.9) in Cleveland, Ohio, to 81.9% (95% CI = 74.2--89.7) in Boston, Massachusetts (median: 72.0%) (Table 5). The HP2010 objective (objective no. 5.13) is to increase the proportion of adults with diabetes who have an annual dilated eye examination to 75.0%. Glycosylated Hemoglobin Measurement at Least Twice a Year Among Adults Aged >18 Years with Diabetes Among 22 Steps communities, the estimated prevalence among respondents aged >18 years who reported having ever been told by a doctor that they have diabetes (other than during pregnancy) and who reported having received a glycosylated hemoglobin measurement ("A1c") at least twice a year ranged from 54.8% (95% CI = 45.8--63.8) in Cleveland, Ohio, to 89.8% (95% CI = 83.5--96.0) in Inter-Tribal Council, Michigan (median: 69.8%) (Table 6). Self--Blood Glucose Monitoring Among Adults Aged >18 Years with Diabetes Among 22 Steps communities, the estimated prevalence among respondents aged >18 years who reported ever having been told by a doctor that they have diabetes (other than during pregnancy) and who reported self--blood glucose monitoring at least twice daily ranged from 28.2% (95% CI = 19.2--37.1) in Austin, Texas, to 46.8% (95% CI = 37.5--56.1) in Philadelphia, Pennsylvania (median: 40.2%) (Table 7). Self--Foot Examination Among Adults Aged >18 Years with Diabetes Among 20 Steps communities, the estimated prevalence among respondents aged >18 years who reported ever having been told by a doctor that they have diabetes (other than during pregnancy) who reported checking their feet at least once daily for any sores or irritations ranged from 61.7% (95% CI = 52.7--70.7) in Chautauqua County, New York, to 79.2% (95% CI = 72.5--85.9) in Southeast Alabama (median: 74.6%) (Table 8). Asthma Symptom-Free Days Among Adults Aged >18 Years with Asthma Among 35 Steps communities, the prevalence of reported asthma ranged from 7.0% (95% CI = 4.3--9.7) in Santa Cruz County, Arizona, to 17.6% (95% CI = 15.2--20.0) in Philadelphia, Pennsylvania (Table 9). The Steps communities' median was 12.4%. The national BRFSS median was 12.6%; this median was exceeded by 18 Steps communities. Of persons with asthma who reported having had an episode of asthma or an asthma attack during the preceding 12 months, the prevalence of persons reporting having had no symptoms in the previous 30 days ranged from 15.4% (95% CI = 9.1--21.7) in Pueblo County, Colorado, to 40.3% (95% CI = 30.5--50) in St. Petersburg-Pinellas County, Florida. Among 10 communities, the median was 20.9% (Table 10). Physical Activity Among Adults Aged >18 Years Overall, the estimated prevalence among respondents aged >18 years who reported engaging in moderate physical activity for >30 minutes at least five times a week or who reported engaging in vigorous physical activity for >20 minutes at least three times a week ranged from 42.0% (95% CI = 38.7--45.3) in New Orleans, Louisiana, to 62.2% (95% CI = 59.0--65.3) in Jefferson County, New York (median: 51.1%) (Table 11). The nationwide 2005 BRFSS median was 49.1%; this median was exceeded by 22 Steps communities. Fruit and Vegetable Consumption Among Adults Aged >18 Years Overall, the percentage of respondents aged >18 years who reported eating fruits and vegetables at least five times a day ranged from 15.6% (95% CI = 13.7--17.5) in Cherokee Nation, Oklahoma, to 30.3% (95% CI = 27.6--33.0) in Salinas-Monterey County, California (median: 24.9%) (Table 12). The nationwide 2005 BRFSS median of 23.2% was exceeded by 27 Steps communities. Tobacco Use Cigarette Smoking Among Adults Aged >18 Years The estimated prevalence among respondents aged >18 years who reported having smoked at least 100 cigarettes in their lifetime and who were current smokers on every day or some days ranged from 11.0% (95% CI = 7.6--14.4) in Rochester-Olmstead County, Minnesota, to 39.7% (95% CI = 28.8--51.6) in Colville Confederated Tribes, Washington (median: 21.7%) (Table 13). The national 2005 BRFSS median was 20.6%; this median was exceeded by 24 Steps communities. The HP2010 objective (objective no. 27-1a) is to reduce the proportion of adults who smoke to 12.0%. Tobacco Use Cessation Attempts by Smokers Aged >18 Years Among 31 communities, the estimated prevalence among smokers aged >18 years who reported having stopped smoking for >1 day during the preceding 12 months because they were trying to quit smoking ranged from 47.8% (95% CI = 41.7--54.0) in Teller County, Colorado, to 63.3% (95% CI = 55.0--71.6) in DeKalb County, Georgia (median: 55.9%) (Table 14). The HP2010 objective (objective no. 27.5) is to increase smoking cessation attempts by adult smokers to 75.0%. DiscussionThe CDC Steps Program responds to community needs and works to affect change at the population level using a community-based approach. The program funds communities across the country to demonstrate how local initiatives across sectors (e.g., community, school, worksite, and health care) in collaboration with traditional and nontraditional partners (e.g., media outlets and departments of, transportation) can reduce the burden of chronic conditions such as obesity, chronic diseases such as diabetes and asthma, and the underlying risk factors of physical inactivity, poor nutrition, and tobacco use. The Steps Program's focus of joining the resources and perspectives of a wide range of sectors and entities dedicated to collaboration for health improvement draws on common interests and accelerates progress toward health promotion efforts. Such efforts create measurable improvements in community health through the selection, implementation, and evaluation of programmatic activities. The findings in this report indicate variations in the estimated prevalence of chronic conditions and diseases, health-risk behaviors, and use of preventive screening practices across Steps communities. With respect to achieving HP2010 objectives, 18 communities achieved the HP2010 objective to increase the proportion of adults with diabetes who have at least an annual foot examination to 75.0%; five communities achieved the HP2010 objective to increase the proportion of adults with diabetes who have an annual dilated eye examination to 75.0%; one community achieved the HP2010 objective to reduce the proportion of adults who smoke to 12.0%. No communities achieved the HP2010 objective to reduce the proportion of adults who are obese to 15.0% or achieved the HP2010 objective to increase smoking cessation attempts by adult smokers to 75.0%. Steps communities' use of BRFSS questions for community-specific surveys permits useful collection of data at the local level. The data presented in this report indicate that communities vary widely in prevalence rates of important chronic disease indicators. In part, this variability might reflect differences in state and local laws and policies, enforcement practices, availability of effective community interventions, prevailing behavioral and social norms, demographic and adult practices, characteristics of the population, and other social determinants of health. Going forward, collection of Steps BRFSS data will provide trend estimates that will permit making community-to-community, national, and HP2010 comparisons. These data also will provide useful information for programmatic decision-making at the community, local, and state levels and guide local health officials and decision-makers in program planning and evaluation. Steps Program staff and other public health and education practitioners can use these data to assess changes in these behaviors over time and assist in evaluating the effectiveness of Steps community programs. An examination of the variations among communities can identify which communities would benefit from additional targeted technical assistance related to effective community interventions and policies. Differences between communities also can alert program managers to the opportunity to learn from each other by taking advantage of the national network they have established within the Steps Program. Communities can use these data to identify, prioritize, and develop community-specific activities to further reduce obesity, diabetes, and asthma by increasing physical activity, encouraging healthy eating, and reducing tobacco use. Limitations The findings in this report are subject to at least five limitations. First, the Steps BRFSS survey queries only persons with landline telephone access and excludes persons who reside in households that lack telephone access or persons who use only cellular telephones; therefore, the data might not reflect the characteristics of persons who reside in households without landline telephones. Second, prevalence estimates are self-reported and thus the reported estimates might be subject to recall bias. Third, each Steps community has the option to modify BRFSS data collection methodology, which might preclude standardization in some cases. Fourth, the number of interviews varied widely (range: 490--2,247). Therefore, estimates for some communities are based on smaller sample sizes and might yield unstable estimates for rare events. Finally, Steps BRFSS does not collect information from institutionalized persons, thereby excluding persons residing in nursing homes, long-term--care facilities, and correctional institutions. ConclusionSteps BRFSS data enable public health authorities to monitor health risk behaviors over time and support focused prevention and intervention programs. Steps Program staff at the national, state, local, and tribal levels will use these data for decision-making, program planning, and enhancing technical assistance. The Steps Program works to achieve HP2010 objectives by using BRFSS data to enhance existing program activities, focus existing programs on activities with the greatest promise of results, identify opportunities for strategic collaboration, and disseminate lessons learned. References
* One Steps community, the Tohono O'odham Tribe, did not report data because BRFSS does not include persons residing in households without telephones, and this community's low telephone coverage precluded reaching the numbers required for standard sampling methodology. † The HP2010 objective refers to adults aged >20 years whereas Steps data are collected for adults aged >18 years. Table 1 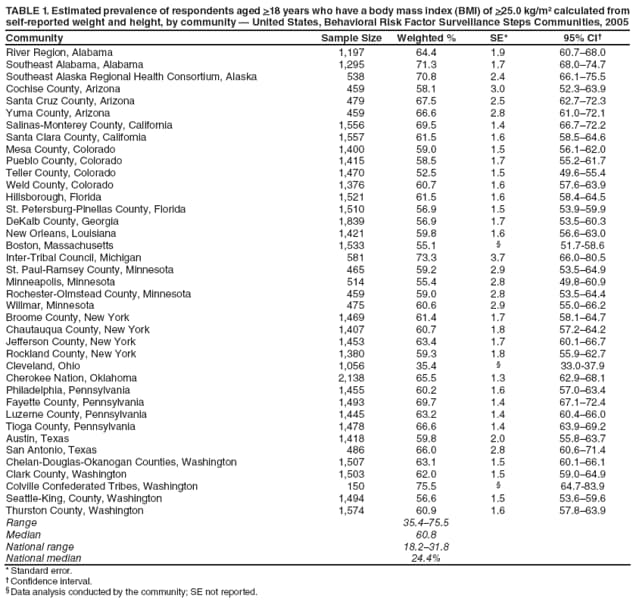 Return to top. Table 2  Return to top. Table 3 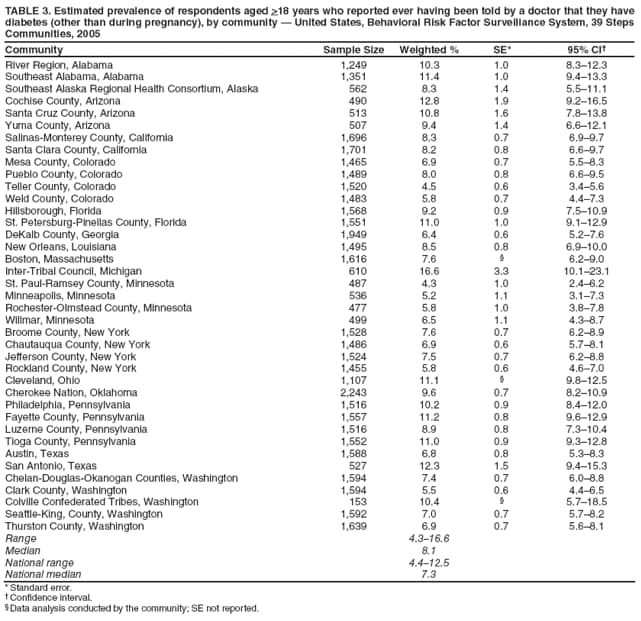 Return to top. Table 4  Return to top. Table 5  Return to top. Table 6  Return to top. Table 7  Return to top. Table 8  Return to top. Table 9  Return to top. Table 10  Return to top. Table 11 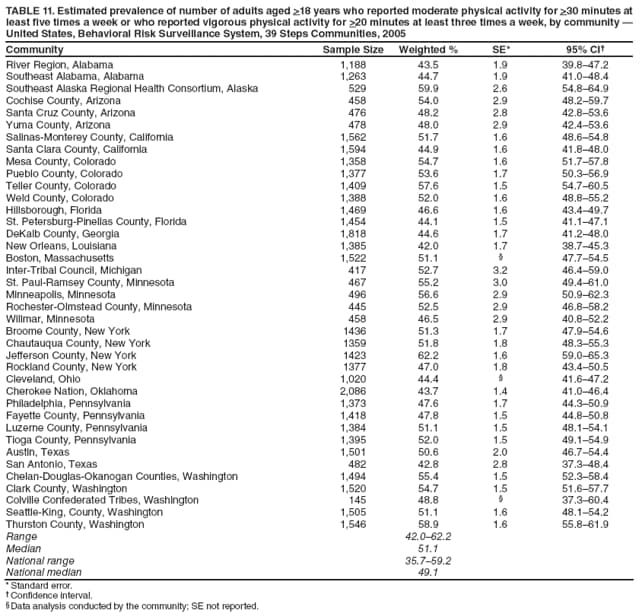 Return to top. Table 12  Return to top. Table 13  Return to top. Table 14  Return to top.
All MMWR HTML versions of articles are electronic conversions from typeset documents. This conversion might result in character translation or format errors in the HTML version. Users are referred to the electronic PDF version (http://www.cdc.gov/mmwr) and/or the original MMWR paper copy for printable versions of official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Date last reviewed: 10/17/2008 |
|||||||||
|