 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Surveillance for World Trade Center Disaster Health Effects Among Survivors of Collapsed and Damaged BuildingsRobert M. Brackbill, PhD,1 Lorna E. Thorpe,
PhD,2 Laura DiGrande, MPH,2 Megan Perrin,
MPH,2 James H. Sapp, II,
MS,1 David Wu, MS,2 Sharon Campolucci,
MSN,1 Deborah J. Walker, PhD,2
Corresponding author: Robert M. Brackbill, PhD, World Trade Center Health Registry, New York City Department of Health and Mental Hygiene, 125 Worth St., CN #6, New York, NY 10013. Telephone: 212-788-5331; Fax: 212-788-4127; E-mail: rbrackbi@health.nyc.gov. AbstractProblem/Condition: Survivors of collapsed or damaged buildings from the attack on the World Trade Center (WTC) were among those most exposed to injury hazards, air pollution, and traumatic events. Reporting Period: This report summarizes data from health outcomes collected during interviews conducted from September 5, 2003, to the close of the World Trade Center Health Registry (WTCHR) enrollment on November 20, 2004. Description of System: WTCHR will be used to monitor periodically the mental and physical health of 71,437 enrollees for 20 years. The analysis is limited to 8,418 adult survivors of collapsed buildings (n = 5,095) and buildings with major or moderate damage (n = 3,323), excluding those who were involved in rescue and recovery. Results: A total of 62.4% of survivors of collapsed or damaged buildings were caught in the dust and debris cloud that resulted from the collapse of the WTC towers, and 63.8% experienced three or more potentially psychologically traumatizing events. Injuries were common (43.6%), but few survivors reported injuries that would have required extensive treatment. More than half (56.6%) of survivors reported experiencing new or worsening respiratory symptoms after the attacks, 23.9% had heartburn/reflux, and 21.0% had severe headaches. At the time of the interview, 10.7% of building survivors screened positive for serious psychological distress (SPD) using the K6 instrument. After multiple adjustments, data indicated that survivors caught in the dust and debris cloud were more likely to report any injuries (adjusted odds ratio [AOR] = 3.9; p<0.05); any respiratory symptom (AOR = 2.7; p<0.05); severe headaches (AOR = 2.0; p<0.05); skin rash/irritation (AOR = 1.7; p<0.05); hearing problems or loss (AOR = 1.7; p<0.05); heartburn (AOR = 1.7; p<0.05); diagnosed stroke (AOR = 5.6; p<0.05); self-reported depression, anxiety, or other emotional problem (AOR = 1.4; p<0.05); and current SPD (AOR = 2.2; p<0.05). Adjustment for SPD did not diminish the observed associations between dust cloud exposure and physical health outcomes. Building type and time of evacuation were associated with injuries on September 11, 2001 and reported symptoms; building type (collapsed versus damaged) also was associated with mental distress. Interpretation: Two to three years after September 11, survivors of buildings that collapsed or that were damaged as a result of the WTC attack reported substantial physical and mental health problems. The long-term ramifications of these effects are unknown. Many survivors were caught directly in the dust and debris of collapsing towers, a dense cloud of particulate matter that might have produced or exacerbated these health effects. Public Health Action Recommended: Long-term follow-up of building survivors and all other persons enrolled in WTCHR should be maintained, with particular attention to those persons exposed to the dust cloud. Some of these findings might lead to building designs that can minimize injury hazards. IntroductionThe terrorist attack on the World Trade Center (WTC) on September 11, 2001, resulted in exposure to potentially harmful debris and environmental contaminants and potential psychological effects related to traumatic events. The collapse of the two WTC towers after they were struck by airplanes released pulverized steel, glass, cement, and other debris into the immediate environment. The fires started by the crashes of the two airplanes, which each carried approximately 90,000 L of jet fuel, released smoke and fumes, including polycyclic aromatic hydrocarbons, volatile organic compounds, lead, dioxin, and furans (1), creating a mixed cloud of dust, smoke, and debris. The collapse of each tower and neighboring buildings released into the immediate environment a highly alkaline mix of mostly large particles (i.e., 98.0% of particles >10 µm) of concrete, glass, plastic, paper, and other building materials and the pulverized contents of the WTC buildings (2). The fires in the 16-acre pile of rubble burned for approximately 3 months, during which time many persons returned to work in lower Manhattan (2). Many occupants of the WTC towers and other nearby buildings witnessed one or more of the events of the attack and were caught in the dense clouds of dust, smoke, and debris created by the collapse of each of the WTC towers. These building occupants also were among those most likely to lose friends, co-workers, and family members in the attack. As a result, building survivors were at high risk for injury, respiratory complications, and psychological distress. Previous studies have reported both respiratory problems and psychological effects from the attacks of September 11, in other populations affected by the attacks (3,4). Shortly after the disaster, the New York City Department of Health and Mental Hygiene (DOHMH) proposed the formation of a registry of persons who were exposed to the WTC disaster. In July 2002, the Agency for Toxic Substances and Disease Registry (ATSDR) received funding from the Federal Emergency Management Agency (FEMA) to collaborate with DOHMH in the creation of the World Trade Center Health Registry (WTCHR). ATSDR was authorized by the Comprehensive Environmental Response Compensation and Liability Act (CERCLA) of 1980 to identify high-priority substances that are hazardous to health and to establish registries to monitor persons exposed to these substances. For example, under CERCLA, ATSDR formed the National Exposure Registry, which focused on exposure to four chemicals (benzene, dioxin, trichloroethylene, and trichloroethane) from household drinking water (5). WTCHR is the largest environmental health registry created in the United States (6). Populations recruited for WTCHR included survivors of collapsed and damaged buildings, pedestrians, and other persons in downtown Manhattan and in the immediate vicinity of the WTC site on September 11; rescue, recovery, and clean-up workers; residents; and school children and school staff in downtown Manhattan. WTCHR is designed to track the physical and mental health status of a large group of highly exposed persons for up to 20 years through regular health surveys, in-depth studies, and matching with cancer registries and vital records. This report focuses on persons who were survivors of buildings or structures damaged or destroyed on September 11. The objectives of this study were to assess the physical and mental health conditions and symptoms reported by building survivors, especially those who had been occupants of collapsed buildings (e.g., WTC-1 and WTC-2) using data from the WTCHR baseline interviews conducted during September 5, 2003--November 20, 2004, and to examine relations between reported experiences and exposures and health outcomes. Health outcomes include injuries on September 11, new and worsening respiratory and nonrespiratory symptoms and conditions after September 11, and mental health symptoms during the 30 days preceding the interviews. MethodsDevelopment of Registry Eligibility CriteriaResearchers developed registry eligibility criteria to identify a subgroup of persons with the most direct exposure to the events of September 11 and its aftermath. Various factors included proximity by time and place to the WTC attack, probability of exposure to the dust and debris cloud, and exposure to fires and fumes from burning debris at the WTC site during the months after the attack. Using these criteria, researchers constructed four broad eligibility groups: 1) persons who were south of Chambers Street in Manhattan on September 11, 2001 (including persons who were in collapsed or damaged buildings or structures, persons in other buildings, and persons in transit or outdoors) (estimated denominator: 362,092); 2) workers/volunteers involved in rescue, recovery, clean-up, and other activities at the WTC site, at the Staten Island Recovery WTC Operations Center, or on transport barges from the WTC site at least one shift anytime during September 11, 2001--June 30, 2002 (estimated denominator: 91,469); 3) persons whose primary residence was south of Canal Street in Manhattan on September 11, 2001 (estimated denominator: 57,511); and 4) school children enrolled and staff employed at schools south of Canal Street on September 11 (estimated denominator: 15,167) (Figure 1). Potential enrollees were screened for eligibility on the basis of these criteria in the WTCHR baseline interview (7,8). Identification and Recruitment of RegistrantsResearchers recruited registrants for enrollment into WTCHR primarily through local and regional media and outreach to eligible persons and groups. Lists of names and associated contact information of potentially eligible persons were voluntarily provided by different entities such as employers and governmental agencies. In addition, persons could enroll by calling a toll-free number or could preregister on a WTCHR Website. Persons who preregistered on the web site were contacted several days later and interviewed by telephone. A total of 232 lists were obtained, representing 135,450 potential registrants. Of the 232 lists, 144 included rescue, recovery, and clean-up workers and volunteers; 76 included building occupants; nine included students and school staff; and three included residents south of Canal Street in lower Manhattan. A list containing 95,442 names of persons who had received security clearance at WTC buildings 1--7 was an important source for contacting building survivors (8). Data Collection and ProcessingData were collected using web-based, computer-assisted telephone interviewing (CATI) or computer-assisted in-person personal interviewing (CAPI). Of the 71,437 persons who completed the WTCHR baseline interviews, 43,487 were persons who were south of Chambers Street on September 11, 30,665 were workers and volunteers involved in rescue, recovery, and clean-up, 14,665 were residents south of Canal Street, and 2,646 were school children enrolled and staff employed at schools south of Canal Street. The sum of these numerators is greater than 71,437 because 28% of registrants were members of more than one eligibility group. Interviews for 67,527 (95%) were completed by telephone, and interviews for 3,910 (5%) were completed in person. The questionnaire was programmed in four languages: English, Spanish, Mandarin, and Cantonese. Registrants whose primary language was not one of the pretranslated languages (n=315) were interviewed by using a translation service provided by a vendor. Proxy interviews were conducted for adults if the potential registrant was either deceased after September 11 (n = 160) or was seriously physically or mentally disabled and unable to perform his or her own interview (n = 375). For persons aged <18 years at the time of interview, parents or guardians answered the questions for their children during the interview (n = 2,565). A total of 3,100 proxy interviews were completed. Respondents were monitored for indications of distress during the interview by scoring their answers to mental health indicators in the interview and by observing their behavior (e.g., crying or trembling voice). If a respondent's answers or behavior indicated emotional distress, the interviewer took actions (e.g., suggesting taking a break, stopping the interview, providing a referral, or making a telephone call to the Mental Health Association of New York's LifeNet counseling service). The WTCHR baseline instrument was designed to take approximately 30 minutes to administer. The interview included the following:
A limited number of questions (e.g., demographics, cause of death, and contact information) were completed by proxy for eligible persons who died after September 11. The baseline questionnaire was pilot tested. On the basis of the results of the pilot testing, the questionnaire was revised to make it more efficient and to clarify some questions (7). Case DefinitionAnalyses in this report are restricted to adult survivors (aged >18 years at the time of interview and were office workers and visitors) who were present between the time of the first airplane impact and noon on September 11, in any one of the 38 primarily nonresidential buildings or structures (Table 1) that were damaged or that collapsed as a result of the September 11 attack.* Rescue, recovery, and clean-up workers who entered the collapsed or damaged buildings after the attack started were excluded from this analysis because this group had other types of exposures (e.g., extended periods of work at the WTC site digging and removing debris) that need to be considered in a separate analysis. Exposure CharacterizationThe following information from the baseline interview was used to characterize exposures among survivors of collapsed or damaged buildings: being caught in the dust and debris cloud that resulted from the collapse of the buildings, including length of time in the cloud; type of building (e.g., collapsed versus damaged) and floor† occupied before evacuation; time of evacuation on the morning of September 11§; and personally witnessing potentially traumatizing events (e.g., seeing an airplane hit either one of the WTC towers, a building collapse, persons running away, someone who was injured or killed, or persons falling or jumping from the WTC towers). Buildings were categorized as collapsed or partially collapsed with major or moderate damage on the basis of a rating system developed by FEMA (Table 1) (10). For analysis, data on survivors of collapsed or partially collapsed buildings were grouped as occupants of "collapsed buildings," and data on survivors of buildings with major or moderate damage were grouped as occupants of "damaged buildings." This report describes the relations between various exposures. Health MeasuresDuring the WTCHR baseline interview, respondents were asked about specific injuries on September 11, respiratory and nonrespiratory symptoms before and after September 11, and diagnosed conditions before and after September 11. The questions did not limit reporting of injuries or symptoms to those for which respondents sought treatment at an emergency department (ED) or other health-care facility. Respondents were asked about specific types of injuries sustained on September 11, including eye injury/eye irritation; sprain or strain; cut, abrasion, or puncture; fracture or dislocation; burn; concussion, head injury, or loss of consciousness; and other types of injuries. Respondents were not asked if their injuries were treated in EDs. Information about symptoms after September 11 was elicited by asking, "Since 9/11, have you had any of the following symptoms….?"¶ Symptoms on the list of new or worsening respiratory symptoms after September 11 included wheezing; shortness of breath; persistent cough; throat irritation; and sinus problems, nose irritation, and postnasal irritation. Symptoms on the list of new or worsening nonrespiratory symptoms included hearing problem or hearing loss; severe headaches; heartburn, indigestion, or reflux; and skin rash or irritation. Information about specific diagnosed conditions was elicited by asking, "Have you ever been told by a doctor, nurse, or health professional that you had…" for specified conditions. The wording of the interview questions was similar to that used in the Behavioral Risk Factor Surveillance System (11). A separate question was asked to clarify whether the respondent had the condition before or after September 11.** Self-reported, newly diagnosed conditions after September 11 included asthma, emphysema, hypertension, coronary heart disease, angina, heart attack, diabetes, stroke, and cancer or malignancy of any kind. All injury, symptom, and condition data were self-reported. Medical record reviews, clinical interviews, or medical examinations were not conducted to validate reported physical or mental health outcomes. Mental health outcomes for which data were collected included self-reported new or worsening depression, anxiety, or other emotional problems. A validated psychometric scale was used to assess SPD (12,13). The scale used to determine SPD was the K6 scale, a psychometrically validated epidemiologic screening measure used in the National Health Interview Survey since 1997 (13). The K6 is highly correlated with diagnostic measures of major depressive disorder, generalized anxiety disorder, schizophrenia, and other mental disorders listed in the Diagnostic and Statistical Manual of Mental Disorders, 4th Edition (13,14). In this analysis, the proportion of respondents who scored above a cut-off of 13 (sum of six questions each coded 0--4 points) on the K6 scale were reported. This level indicates SPD.†† Data AnalysisSAS® (version 9.1) (15) was used for data management and for computing frequency distributions, prevalences, adjusted odds ratios (AORs), and 95% confidence intervals (CIs). Denominators used for prevalence calculations excluded missing answers for each physical and mental outcome measure. Unconditional multiple logistic regression was used to compute AORs to assess the association of health symptoms or conditions with selected exposures. Exposures included being present in the dust and debris cloud versus not; occupying a collapsed building versus a damaged building; and evacuating before or after the collapse of WTC-2, the first building to collapse. The floor occupied at the time of the attack was included only in the analysis of injuries among survivors of WTC-1 or WTC-2. Inconsistencies between self-reported locations and exposures that were identified were counted as invalid. For example, some interview respondents said they occupied floors that did not exist in specific buildings; other respondents gave a time of evacuation that was after the time that the building had collapsed. In the logistic regression, the mode of recruitment of respondents (i.e., from a list or self-identified) and the existence of SPD in a respondent was controlled for because persons who self-identified might be more likely to have health problems or concerns than those who did not self-identify or enroll (16), and a respondent's level of psychological distress might differentially influence reporting of exposures and health problems. AORs were adjusted for sex, age on September 11, and race/ethnicity (except for a small number of instances when the sample size was too small for stratification by all adjustment variables). In addition, in the logistic regression model for respiratory health symptoms, smoking status at the time of the interview was included. ResultsThe number of survivors from one of the 38 buildings and structures destroyed or damaged on September 11, was 62,092 (8). Of these, 10,393 (17%) were enrolled in the WTCHR through achieving contact with those eligible from lists and interviewing others who self-identified. The American Association for Public Opinion Research (AAPOR) response rate for this group was 45.2% (17).§§ Lists were used to contact 32.4% of the adult building survivors (n = 3,367); the remainder were identified when they called a toll free number or accessed the WTCHR Web site. Data were analyzed for 8,418 adult survivors of 38 buildings, including six collapsed, four partially collapsed, and 28 damaged buildings. Rescue, recovery, or clean-up workers (n = 1,770); children (n = 58) who were building survivors; and survivors for whom age or building type was unknown (n = 147) were excluded. Of the 8,418 adult building survivor enrollees, 5,095 (60.5%) had been occupants of totally or partially collapsed buildings (i.e., survivors of collapsed buildings), and 3,323 (39.5%) had been occupants of damaged (major or moderate damage) or noncollapsed buildings (i.e., survivors of damaged buildings) (Figure 2). Of those who were occupants of collapsed buildings, 3,960 (72.4%) enrollees had been in WTC-1 or WTC-2. Demographic CharacteristicsOf the 8,418 survivors, 55.8% were from New York City, 26.8% were from New Jersey, 14.3% were from New York State (excluding New York City), 1.0% were from Connecticut, and 2.0% were from other states or countries (Table 2). Of the 4,659 survivors who were New York City residents, 34.9% lived in the borough of Manhattan, 28.0% lived in Brooklyn, 20.9% lived in Queens, 8.8% lived on Staten Island, and 7.3% lived in the Bronx. The enrollees were more likely to be male (54.2%) than female (45.8%). The majority of (55.8%) were aged 25--44 years on September 11, 2001. A total of 63.3% were non-Hispanic white, 81.3% had at least some college education, and 47.5% had a household income between $35,000 and $100,000 in 2002 (Table 3). Demographic characteristics of survivors of collapsed and damaged buildings were generally similar, except that enrolled survivors of collapsed and damaged buildings had a higher proportion of men (57%) and persons from New Jersey (32%) than enrolled survivors of damaged buildings (50% and 19%, respectively). Exposure AssessmentA total of 62.4% of survivors were caught in the dust and debris cloud; survivors of collapsed buildings reported little difference from survivors of damaged buildings in regard to dust cloud exposure (Table 3). Survivors of damaged buildings were in the dust and debris cloud for a longer time (median: 45 minutes) than survivors of collapsed buildings (median: 30 minutes). The majority of (80.8%) WTCHR enrollees who were survivors of collapsed buildings began evacuating before the second airplane hit, compared with 32.1% of survivors from damaged buildings. Overall, 90.9% of all registrants from these buildings reported that they began evacuating their building before the collapse of WTC-2. Almost all enrollees who evacuated damaged and destroyed buildings (94.7%) witnessed at least one event that had potential for inducing psychological trauma (Table 3); nearly two thirds of building survivors (63.8%) personally witnessed three of the five events (Table 3). The majority of building survivors reported that they witnessed someone who was injured or killed (59.4%) and persons falling or jumping from the WTC towers (61.1%). Among the 5,095 enrollees from collapsed buildings, 11.5% reported that they were located on the 76th floor or higher; slightly more than one third (38.4%) reported that they were below the 10th floor (Table 3). Among the 3,323 survivors from damaged buildings, half (49.1%) reported that they were below the 10th floor and 3.9% reported that they were above the 42nd floor during the morning of September 11. Among the latter group, the highest floor occupied was the 58th floor of the Millennium Hotel. The damaged buildings on average had fewer floors (range of number of floors: 3--58; median number of floors: 22; mean number of floors: 24) than collapsed buildings (range: 1--110; median: nine; mean: 36). Injuries Sustained on September 11Of the building survivors, 43.6% reported sustaining an injury. The most commonly reported injuries were eye injury/eye irritation (31.6%); sprain or strain (13.6%); and cut, abrasion, or puncture wound (9.7%). Few survivors reported sustaining more serious injuries (e.g., burns, broken bones, or head injuries) (Table 4). After adjusting for demographics, mode of recruitment, and level of SPD, the likelihood of sustaining any injury on September 11, was 3.9 times (p<0.05) greater among survivors caught in the dust and debris cloud than among survivors who were not in the dust cloud and debris cloud (56.2% versus 22.8%) (Table 4). Survivors who were in the dust and debris cloud were 5.3 times (p<0.05) more likely to have reported eye injury/eye irritation (43.8% versus 11.6%). Being in the dust and debris cloud also was associated with all other types of injury (Table 4). Compared with dust and debris cloud exposure, the other exposures assessed in this report (type of building, time of evacuation, and floor or level of WTC-1 or WTC-2) were less consistently associated with sustaining an injury on September 11 (Tables 4 and 5). For example, survivors of collapsed buildings had only a slightly higher likelihood of any injury (45.5% versus 42.3%; AOR = 1.2; p<0.05) compared with survivors of damaged buildings. Survivors of collapsed buildings did have a twofold greater likelihood of less prevalent, but more serious, injuries such as fractures (2.7% versus 1.1%; AOR = 2.3; p<0.05) or head injury (2.1% versus 0.7%; AOR = 2.8; p<0.05) (Table 4). Evacuating after the collapse of WTC-2 increased the risk for any injury (54.4% versus 42.2%; AOR = 1.5; p<0.05); eye injury or irritation (46.2% versus 29.7%; AOR = 1.9; p<0.05); and cut, abrasion, or puncture (12.9% versus 9.4%; AOR = 1.4; p<0.05). In addition, injuries were examined by the floor that survivors (n = 3,690) occupied in WTC-1 and 2 before evacuation (Table 5). Mid-level floors 10--42 were used as reference floors because injuries were concentrated on the lower and upper levels of WTC-1 and 2. The airplanes struck WTC-1 near floors 93--100 and WTC-2 near floors 77--84 (18). Compared with survivors on mid-level floors, survivors on lower floors (basement, mezzanine, concourse, and lobby) were 1.4 times (p<0.05) more likely to sustain any injury, and survivors on higher floors (76 and above) were 1.9 (p<0.05) times more likely to sustain any injury (Table 5). Burns were 3.4 (p<0.05) times more likely to occur among survivors who were on uppermost floors (76 and above), and 3.8 (p<0.05) times more likely to occur among survivors who were on the lowest floors than among those on mid-level floors. Concussion, head injury, or loss of consciousness was more likely to occur among survivors who were on lower or uppermost floors (e.g., floors 2--9) (AOR = 4.6, p<0.05) (Table 5). Sprain or strain injuries were also more likely to occur among survivors who were on uppermost floors. Respiratory Symptoms and Conditions After September 11The majority of (56.6%) survivors of collapsed or damaged buildings reported one or more new or worsening respiratory symptoms after September 11, including symptoms of sinus problems, nose irritation, and postnasal irritation (38.1%); shortness of breath (35.1%); wheezing (28.5%); throat irritation (28.0%); and persistent cough (27.0%) (Table 6). Two percent of survivors reported newly diagnosed asthma, and 0.2% of survivors reported newly diagnosed emphysema after September 11. After adjusting for demographics, mode of recruitment, level of SPD, and smoking status, building survivors who reported being in the dust and debris cloud were significantly more likely (66.6% versus 39.6%; AOR = 2.7; p<0.05) to have had new or worsening respiratory symptoms compared with those who were not in the dust and debris cloud (Table 6). Being in the dust and debris cloud was associated (AORs >2.0; p<0.05) with all symptoms and conditions except emphysema. Among new or worsening respiratory symptoms, wheezing had the highest likelihood of occurring among those who were in a dust and debris cloud (36.4% versus 15.6%; AOR = 2.6; p<0.05). Survivors who were in a dust and debris cloud were also 2.1 (p<0.05) times as likely (2.5% versus 1.1%) to report newly diagnosed asthma than were those who reported not being in the dust and debris cloud. Time of evacuation and building type were associated with self-reported respiratory symptoms but not with self-reported newly diagnosed asthma or emphysema (Table 6). For these exposures, AORs tended to be smaller than those found for the dust and debris cloud (Table 6). Survivors who evacuated after the collapse of WTC-2 were 1.6 times (p<0.05) more likely to have any respiratory symptoms (70.0% versus 54.7%) than did those who evacuated before the collapse. In addition, survivors of collapsed buildings were likely to have significantly fewer respiratory symptoms (53.2% versus 62.1%; AOR = 0.8; p<0.05) than did survivors of damaged buildings (Table 6). Nonrespiratory Symptoms and Conditions After September 11Nonrespiratory problems after September 11 were less prevalent than respiratory problems. Only two new or worsening nonrespiratory symptoms had a prevalence that exceeded 20%: heartburn, indigestion, or reflux (23.9%) and severe headaches (21.0%) (Table 7). At the time of interview, hypertension was the most frequently reported new diagnosis of a nonrespiratory condition among survivors (4.9%), followed by cancer or malignancy of any kind (1.4%) and diabetes (1.1%). Similar to the findings related to injuries and respiratory problems, presence in the dust and debris cloud was consistently associated with new or worsening nonrespiratory symptoms after September 11 (Table 7). These symptoms included heartburn, indigestion, or reflux (28.5% versus 16.3%; AOR = 1.7; p<0.05); severe headaches (26.2% versus 12.3%; AOR = 2.0; p<0.05); skin rash or irritation (14.2% versus 7.0%; AOR = 1.7; p<0.05); and hearing problem or hearing loss (10.1% versus 4.8%; AOR = 1.7; p<0.05). In addition, newly diagnosed conditions tended to be more prevalent among survivors exposed to the dust and debris cloud, but the association was significant only for stroke (0.4% versus 0.1%; AOR = 5.6; p<0.05) (Table 7). Because of the small number of cases, the latter model included only mode of recruitment and sex as covariates. Time of evacuation was associated with new or worsening heartburn, indigestion, or reflux (28.1% versus 23.3%; AOR = 1.2; p<0.05), and frequent headaches (26.5% versus 20.1%; AOR = 1.4; p<0.05) (Table 7). Survivors of collapsed buildings were slightly more likely to report a new or worsening hearing problem or hearing loss (8.8% versus 7.0%; AOR = 1.2; p<0.05) and newly diagnosed hypertension (5.2% versus 4.3%; AOR = 1.3; p<0.05) than were survivors of damaged buildings. Survivors of collapsed buildings were less likely to report skin rash or irritation than were survivors of damaged buildings (10.5% versus 12.8%; AOR = 0.8; p<0.05). Building type was not associated with the other newly diagnosed conditions (Table 7). Overall, the associations between the various types of exposures and injuries and physical health were minimally affected by the inclusion of mode of recruitment and level of psychological distress in the multiple logistic regression models. Mental Health ConditionsIn a self-reported assessment of mental health, 5,383 building survivors (64.7%) reported experiencing new onset of depression, anxiety, or emotional problems after September 11, and 10.7% of survivors were determined to have probable SPD at the time of the interview (Table 8). Presence in the dust and debris cloud had the strongest association with self- reported new depression, anxiety, or emotional problems (68.5% versus 58.5%; AOR=1.4; p<0.05) and probable SPD (13.6% versus 5.8%; AOR = 2.2; p<0.05). In addition, survivors of collapsed buildings were more likely to report new depression, anxiety, or other emotional problems (66.7% versus 61.7%; AOR = 1.5; p<0.05) and probable SPD (11.8% versus 9.0%; AOR = 1.5; p<0.05) than were survivors of damaged buildings. Time of evacuation was not associated with either mental health outcome. This analysis did not take into account witnessing traumatic events. DiscussionOngoing surveillance of disaster-related health effects is a key source of information for emergency preparedness and response planning. WTCHR enables researchers to develop a comprehensive picture of the physical and mental health status of persons who were exposed to the September 11 WTC attacks and their aftermath. This initial report describes the self-reported experiences, physical health, and mental health of approximately 8,000 adult survivors who were in buildings that collapsed or that were damaged as a result of the September 11 disaster. Approximately two thirds of these survivors were caught in the dust and debris cloud created by the collapse of the WTC towers, approximately two thirds experienced three or more potentially psychologically traumatizing events, and approximately 40% reported sustaining an injury. A high prevalence of self-reported new or worsening respiratory problems and some nonrespiratory problems was identified, including heartburn and severe headaches after September 11. In addition, approximately 10% of survivors had probable SPD 2--3 years after the event. The experience of being caught in the dust and debris cloud was substantially associated with most of the self-reported physical and mental health outcomes. Time of evacuation and type of building damage (whether collapsed or damaged) were less consistently associated with these outcomes. The relation between exposures and physical health were not confounded by reported level of psychological distress or mode of recruitment (list versus self-identification), as indicated by minimal change in the direction or magnitude of AORs. The association between presence in the dust and debris cloud and higher rates of injuries and respiratory symptoms among building survivors is plausible. For example, survivors could have had immediate eye irritation or injury from particles blown into their eyes when they encountered the dust and debris cloud. They might have sustained musculoskeletal injuries (e.g., strain and sprain injuries or broken bones) while stumbling, falling, and navigating their way through the dust and debris cloud. The respiratory symptoms related to WTC dust that survivors reported might have been exacerbated by the highly alkaline mix of mostly large particles (i.e., 98.0% of particles >10 µm) of concrete, glass, plastic, paper, and other building materials in the dust and debris cloud (19). This material can cause mucus membrane irritation in the upper airways of exposed persons (3). No studies are known to have reported the extent of injuries among survivors who were in buildings affected by the September 11 disaster. A rapid assessment of 790 ED cases treated in five Manhattan hospitals identified primarily inhalation-related injuries or eye irritation among persons who were in buildings or on the street during the attack or after the collapse of WTC-2 and -1 (20). Similar to the pattern of injuries reported by WTCHR building survivors, a relatively small percentage (14%) of persons in the rapid assessment study had serious injuries, including fractures, burns, concussion, or crush injuries (20). Other studies have reported a high prevalence of respiratory and nonrespiratory symptoms among both office workers and residents in lower Manhattan after September 11 (21,22). However, those studies did not specifically examine building survivors, nor did they report any association between symptoms and being in the dust and debris cloud. For example, one study conducted 4 months after September 11 indicated that high percentages of federal employees in an office building several blocks from the WTC reported symptoms such as eye irritation (62%), cough (56%), shortness of breath (28%), and wheezing (21%) (21). In comparison with federal employees in Dallas, the prevalence of cough in the New York City sample was twice as high, the prevalence of shortness of breath was six times higher, and the prevalence of wheezing was four times higher. Another survey conducted 8--16 months after September 11, documented a three to four times higher prevalence of cough (41%), wheezing (28%), and shortness of breath (27%) among residents who lived within a 1-mile radius of the WTC site than among a comparison group of residents who lived approximately 5 miles from the WTC site (22). No information was reported about direct exposure to the dust and debris cloud on September 11. First responders also have been reported to have a high prevalence of documented health problems (23--26). Firefighters and police officers who arrived before the first building collapsed or soon afterward on September 11 had the most serious health problems (23--25). For example, 8% of firefighters who arrived at the scene on September 11 became ill with the "WTC cough," defined as a persistent cough so debilitating that persons who had it required at least 4 weeks of medical leave, compared with 2% of firefighters who arrived later (23). In addition, a higher percentage of police who arrived before the first building collapse had an abnormal spirometry examination (41%) compared with those who arrived during the time between the two collapses (29%) or in the following days (25%) (25). In addition to serious respiratory problems, 87% of firefighters with "WTC cough" had persistent heartburn or gastroesophageal reflux disorder, which also was related to the time of arrival at the WTC site (23, 26). A potential relation was identified between dust cloud exposure on September 11 and newly diagnosed stroke. Because only 0.2% of all survivors reported a new diagnosis of stroke after September 11, this finding is considered preliminary and warrants future monitoring. The finding might be a detection artifact resulting from more frequent visits to doctors by survivors (27). Biologic plausibility for stroke is suggested by studies indicating that fine particulate air pollution is a risk factor for cause-specific cardiovascular disease mortality through mechanisms that probably include pulmonary and systemic inflammation (28--31) and by other studies indicating stress-induced stroke (32,33). In contrast to chronic fine particulate air pollution exposure, exposure to the dust and debris cloud on September 11 was an acute exposure to mostly large particles (3). A study that compared visits to hospital emergency departments within a 50-mile radius of New York City within the 60 days before and after September 11 indicated a 49% increase in visits for myocardial infarction (MI) (34). Higher psychological stress associated with events on September 11 might have resulted in the increased incidence of MIs. Other exposure variables (type of building damage [collapsed versus damaged], floor occupied, and time of evacuation) also were associated with injuries on September 11. For example, survivors of collapsed buildings had a higher risk for fractures and head injuries compared with survivors of damaged buildings. Concussions or head injuries and burns were also more likely to occur among survivors who were on lower and upper floors of WTC-1 or WTC-2, where they might have encountered falling and burning debris. The relation between building floor and serious injuries (e.g., injuries requiring hospitalization) suggests the need for further research on evacuation procedures and building design issues to minimize injury hazards. Regarding less serious injuries, survivors who began evacuating after the collapse of WTC-2 were more likely to report eye irritation or eye injuries and cuts or puncture wounds, suggesting that these specific injuries occurred because of air-suspended dust and debris in the areas these survivors had to transverse. Survivors from the lowest floors of WTC-1 or 2 reported more cuts and eye injury or irritation than did survivors on the uppermost floors, possibly because of falling debris after the airplanes struck the towers. Sprain or strain injuries reported among survivors who were occupants of the WTC towers' upper floors might have been caused by an increased chance of pulling muscles or falling short distances while evacuating. Survivors from upper floors also were exposed longer to injury hazards under difficult circumstances compared with occupants on lower floors (35). Interpretation of data on eye injuries is limited because the baseline interview included eye irritation and eye injury in the same question. Type of building damage also was associated with respiratory and nonrespiratory health problems. For example, respiratory symptoms were more likely to have been reported among survivors of damaged buildings than among survivors of collapsed buildings. This finding is consistent with the fact that the former were more likely to have begun evacuating after the WTC towers collapsed and had a greater median time in the dust and debris cloud (45 minutes) compared with the latter (30 minutes). Other unmeasured differences between occupants of the two building types (e.g., location of the survivor during and after the collapse of the buildings) also might help explain this finding. Reported diagnosis of hypertension and self-report of hearing problem or loss were more likely to have been reported by survivors of collapsed buildings than by survivors of damaged buildings. Although increases in diagnosed conditions such as these might be a product of increased detection, a review of literature on prospective studies of development of hypertension and psychological factors indicates a small but consistent gradient of increased prevalence of hypertension among persons who had measurable psychological distress (36). In addition to experiencing psychological distress, the September 11 building survivors probably were subjected to acute exposures to intense noises during the attack and the collapse of the WTC buildings. Exposure to noise is related to increased heart rate and blood pressure, but the majority of studies have evaluated long-term exposure to noise rather than an acute event (37). Both findings need to be confirmed with a medical evaluation study. Two to 3 years after September 11, the prevalence of probable SPD among building survivors was high (10.7%) and nearly twice the prevalence of SPD documented in New York City adults during a similar period (6.4% in 2002 [38] and 5% in 2003 [39]). A survey of New York City residents conducted 6 months after September 11, 2001, reported a high prevalence of adverse mental health effects among persons exposed to the September 11 disaster (4). Specifically, 15% of adults who were directly affected by the WTC attacks (i.e., persons who were in the WTC complex or who were injured during the attacks, lost possessions, had a friend or relative killed, lost a job as a result of September 11, or were involved in rescue efforts) had probable PTSD compared with 7.4% of all New York City adult residents. To better understand the full psychological impact of the terrorist attacks on September 11, the first biennial WTCHR follow-up survey will be conducted in early 2006 to assess previous history of mental health conditions and life events before and after September 11. It will be important to examine specific mental health conditions among registrants and to assess the witnessing of traumatizing events as a risk factor. A separate report accounting for witnessing of traumatic events will document probable PTSD among building survivors as determined on the basis of the WTCHR baseline interview. Future monitoring of the impact of September 11 will be important to assess the resiliency of survivors. Limitations and StrengthsWTCHR baseline data have proven useful for describing self-reported exposures and health effects among survivors of collapsed or damaged buildings 2--3 years after September 11. However, the findings were subject to several limitations. First, the total number of building survivors is unknown, and estimating the size of this subpopulation was difficult because of the need to use multiple and sometimes conflicting sources of information. An estimated 62,092 persons were in one of the 38 collapsed or damaged buildings on September 11. This estimate was based on a combination of data provided by individual businesses and estimates published in the media (8). However, the resulting coverage rate of 16.7% (10,393 of 62,092) is probably an underestimate because a primary election on September 11 might have reduced the number of persons present in collapsed and damaged buildings on the morning of September 11 to <62,000. Second, the majority of the building survivor enrollees were in the self-identified group, resulting in potential bias. Such persons might have been more likely to have had symptoms or concerns about their exposure and their health than were those persons who were eligible but who did not self-identify or enroll. This effect has been observed in other environmental studies in which persons who believed they had experienced a dangerous exposure tended to over-report health problems (16). To reduce potential bias from self-selection, WTCHR researchers attempted to obtain lists of all potentially eligible survivors. The best available recruitment list, an extensive list of 95,442 persons who had been issued a security badge to any one of the WTC buildings, was not complete or up to date, a problem that limited recruitment of building survivors. However, the security badge list did yield 1,716 completed interviews of building survivors; other lists yielded an additional 1,216 interviews. Physical and mental health symptoms tended to be higher among WTCHR enrollees who self-identified than among those recruited from lists; however, adjusting for mode of recruitment did not modify the observed relation between exposures and physical and mental health symptoms. Third, the relatively low response rate for survivors of collapsed and damaged buildings (44.3%) is an artifact resulting from an inflated denominator. The denominator includes an estimated 6,100 persons on the security badge list who might have been eligible but for whom contact was not successful. After removing the 6,100 persons from computation of the response rate, the rate then becomes approximately 75% for the remaining 8,418 primarily self-identified completed interviews. The higher response rate is a result of a relatively low refusal rate (14%) during the interview and a high eligibility rate (85%), especially among persons who self-identify. Fourth, the WTCHR baseline interviews were conducted 2--3 years after the events of September 11. Recall by survivors about their experiences that day could have been affected by many factors, including the severity of their symptoms and the level of trauma experienced (40). To reduce recall bias, the WTCHR baseline survey asked respondents several times during the interview about their location and time proximity relative to different activities/events on September 11. Fifth, the baseline interview asked registrants whether they had new or worsening physical health symptoms since September 11. Enrollees were not asked about when these symptoms first occurred, how long they lasted, their severity, or their persistence. Therefore, the physical health symptoms reported represent a composite of symptoms of varying duration, severity, and persistence. Two other outcomes included in this report---injuries sustained on September 11 and current psychological problems---are more precisely defined as occurring either on September 11 (injuries) or during the last 30 days (SPD). Planned WTCHR biennial follow-up surveys will determine the extent to which self-reported physical and mental health symptoms persist among registrants. Sixth, the baseline interview question used to assess exposure to the dust and debris cloud had a "yes" or "no" answer, without clarification of how the respondent interpreted being in a dust and debris cloud. Further analysis of location and time data from the baseline survey will enable a more refined characterization of the gradient of exposure by intensity and duration. The first biennial survey will also include a section clarifying the nature of the respondents' exposure to the dust and debris cloud on September 11. Finally, exposure registries do not routinely collect concurrent data from unexposed persons because no clearly stated hypothesis or defined outcome suggests what characteristics the comparison group should have (5). Whereas WTCHR did not include a sample of nonexposed persons, the cohort does have enrollees who experienced a gradation of exposures. Therefore, even in the absence of a true nonexposure group, the effects of different exposure types (e.g., presence in the dust and debris cloud, type of building, and time of evacuation) on physical and mental health in this survivor population were evaluated. In addition, being in the dust and debris cloud was associated with health outcomes, although the likely gradient of exposures within the group exposed to the dust and debris cloud was not assessed. The use of comparison groups will be part of in-depth WTCHR studies focused on specific subpopulations, exposures, and health conditions, for which desired attributes of a comparison group are known and required in the study design. Despite these limitations, WTCHR has a number of strengths that make it an important tool for understanding the long-term health effects of the September 11 disaster among building survivors and other enrollees. WTCHR has a large number of enrollees across a diverse set of highly exposed subpopulations, including building survivors (n = 8,418), residents (n = 14,665), school children and school staff (n = 2,646), and rescue and recovery workers (n = 30,665). These subpopulations have experienced exposures that provide a basis for in-depth studies. Notably, the sizes of WTCHR subpopulations are much larger than those used in any September 11 study that has been reported. For example, the National Institute of Standards and Technology (41) report on survivor behavior during evacuation was based on a sample of 800 persons. In comparison, WTCHR has approximately 4,000 enrollees who were survivors of the WTC towers and a large sample of survivors from other collapsed or damaged buildings. WTCHR is a useful resource for future studies related to the WTC disaster. Designed to follow enrollees for at least 20 years, a sufficient length of time for induction of long-latency cancers, WTCHR will be used to conduct active tracing to maintain up-to-date contact with all enrollees for ongoing surveillance and in-depth studies. Notably, the majority of (91%) registrants agreed at the time of the baseline interview to be contacted by the NYC DOHMH about future studies related to the WTC disaster. Approximately 60% of registrants provided their e-mail addresses to the WTCHR. WTCHR has been used to establish a mechanism for external researchers to gain DOHMH approval for informing registrants about opportunities to enroll in other WTC-related studies (42). In addition, the proportion of enrollees who use e-mail and who have access to the Internet is expected to increase over time, creating a more viable cohort for regular surveillance, updating of contact information, and in-depth studies. Summary and Public Health RecommendationsThis report provides the most comprehensive assessment to date of survivors of damaged and collapsed buildings, including WTC-1 and 2. The findings included a high prevalence of self-reported injuries on September 11 and a high prevalence of new or worsening respiratory and nonrespiratory symptoms after September 11. The prevalence of psychological distress among building survivors during the 30-day period before the interview, which was conducted 2--3 years after the event, was substantial compared with New York City survey estimates. Presence in the dust or debris cloud was the strongest factor associated with many outcomes. In many cases, building type, building floor, and time of evacuation also were associated with health effects. To better understand the clinical and public health significance of these findings among building survivors and other subpopulations of interest, researchers will need to couple ongoing surveillance of health status with in-depth studies that include medical examinations and matching of registrants to cancer registries and vital records. For example, preliminary findings about cardiovascular outcomes (e.g., stroke and hypertension) need to be validated in future research. WTCHR provides a platform for future studies among the various affected groups, which will yield a better understanding of the etiology of health problems related to the WTC disaster and a comprehensive picture of the public health impact of the disaster. Planned biennial follow-up surveys of all WTCHR registrants will help determine the long-term persistence of reported health symptoms and conditions. Acknowledgments We acknowledge the professionalism and compassion of WTCHR baseline interviewers employed by RTI International. The success of the WTCHR baseline enrollment also resulted from the concerted efforts of the outreach, communication, and data teams of the New York City DOHMH, RTI, and ATSDR. In addition, we thank Thomas Frieden, MD, Thomas Matte, MD, and Stephen Friedman, MD, for providing invaluable feedback on conceptual aspects of this report. We also thank the Port Authority of New York and New Jersey for giving us access to a database of persons who were issued security badges for the WTC complex. References
* After WTCHR was designed, FEMA identified and classified 55 buildings south of Chambers Street that were destroyed or damaged between the time of the first plane impact and noon on September 11. WTCHR used information from the New York City Department of Buildings to identify 38 buildings or structures (including the north and south pedestrian bridges) that had structural damage. This report is based on enrollees from all 22 buildings and structures that sustained the most severe collateral damage on September 11 (i.e., six fully collapsed, four partially collapsed, and 12 with major damage) and 16 with moderate damage. Differences between the New York City Department of Buildings list and the FEMA Building Performance Study include the distinction between the North Bridge and WTC Concourse from other WTC buildings and FEMA's inclusion of an additional 19 buildings that sustained moderate damage. † Floors were categorized as 1) basement, mezzanine, concourse, and lobby (i.e., persons exited from these levels and, as a result, they were treated in a separate category); 2) floors 2--9 (hook and ladder typically cannot reach beyond the 10th floor of a building); 3) floors 10--42 (using the same stratification as the National Institute of Standards and Technology [9]); 4) floors 43--75; and 5) floors 76 and higher. § The time when a person began evacuating was determined using the events as they occurred to demarcate time on the morning of September 11 (i.e., when the first airplane hit WTC-1, when the second airplane hit WTC-2, when WTC-2 collapsed, and when WTC-1 collapsed). ¶ For each symptom-related question, each respondent was asked the following: 1. Since 9/11, have you had any of the following symptoms?" A respondent also could describe additional symptoms not mentioned in the list. 2. If the respondent said "yes" to any of the symptoms, then he/she was asked, "Before 9/11 did you have (symptom) 3. If the respondent said "yes" to having had the symptom before 9/11, he/she was asked, "Did your (symptom) get worse after 9/11? A new case was defined as an affirmative answer to question 1 and a negative answer to question 2. A symptom that became worse after 9/11 was defined as affirmative to all three questions. ** For each of the self-reported diagnosed conditions, the following questions were asked: 1. "The next questions ask about health conditions diagnosed by a doctor that you ever had, including before 9/11. Have you ever been told by a doctor or other health professional that you had (condition)?" 2. If the respondent said "yes," he/she was then asked, "Did a doctor or other health professional first tell you that you had (condition) before 9/11 or after 9/11?" A new case of a diagnosed condition was defined as "yes" to the first question and "after 9/11" to the second question. †† Items for SPD: [Repeated for each symptom]: During the past 30 days, that is, since (reference date) how often did you feel …
§§The response rate was calculated according to the AAPOR standard. Response rate is equal to completed interviews divided by the number of completed interviews plus the number of noninterviews plus cases of potential but unknown eligibility. The number of cases of potential but unknown eligibility was estimated by using the proportion of known eligibles on the basis of the number of persons screened and applying that proportion to the number of cases for which no contact occurred. Table 1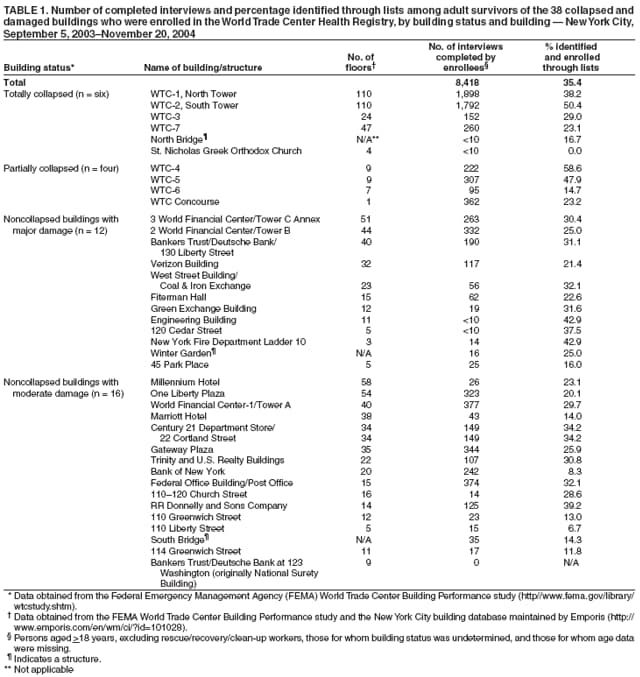 Return to top. Figure 1 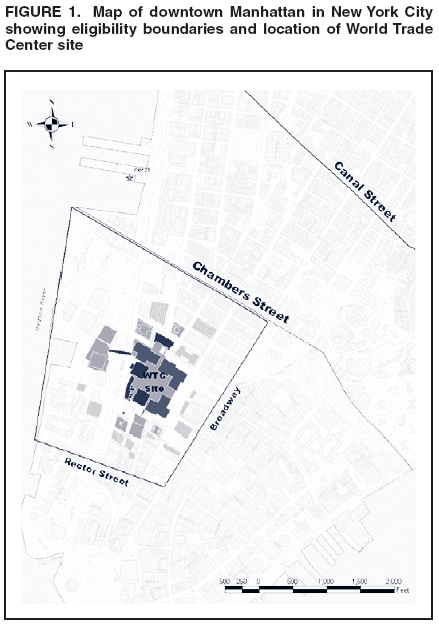 Return to top. Table 2 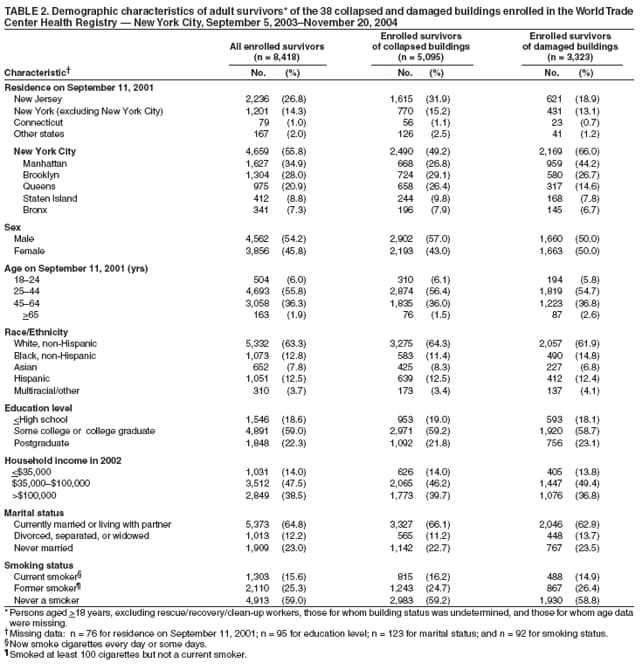 Return to top. Figure 2 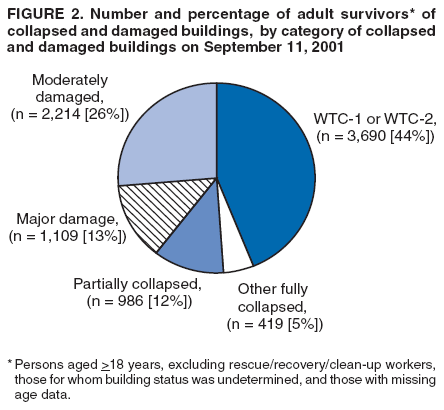 Return to top. Table 3 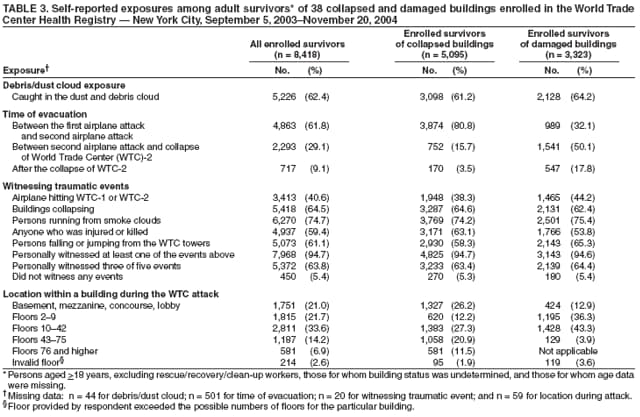 Return to top. Table 4 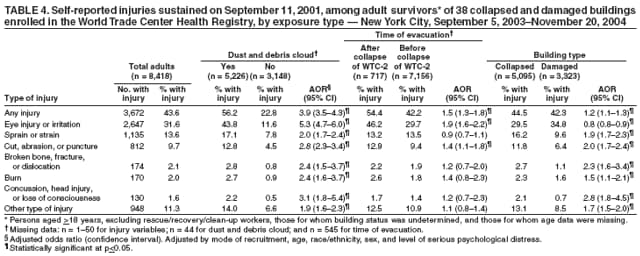 Return to top. Table 5 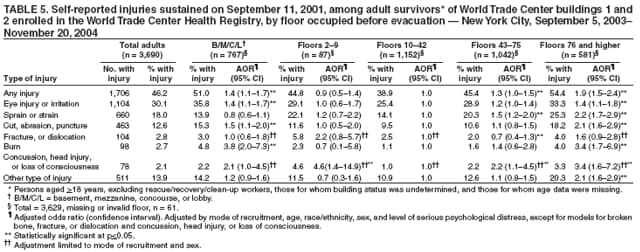 Return to top. Table 6 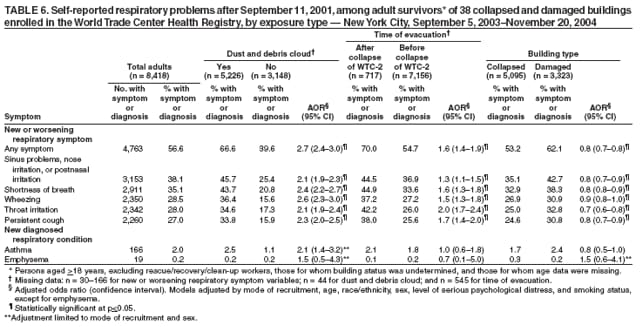 Return to top. Table 7 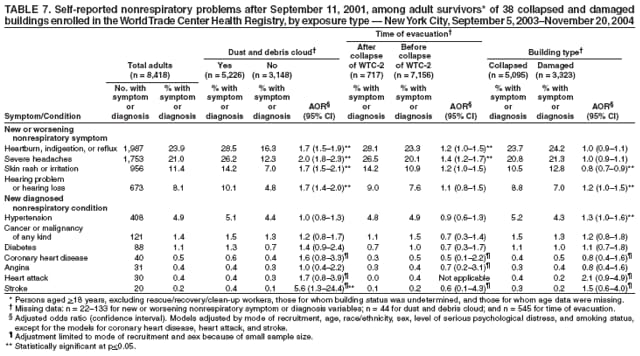 Return to top. Table 8 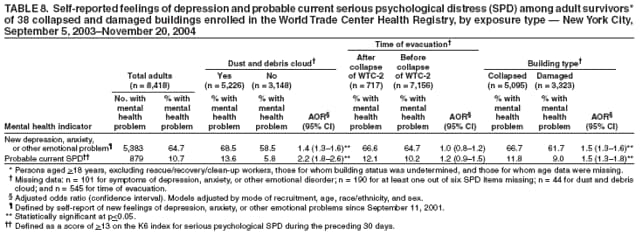 Return to top.
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Date last reviewed: 3/23/2006 |
|||||||||
|