Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail.
Quadrivalent Human Papillomavirus Vaccine
Recommendations of the Advisory Committee on Immunization
Practices (ACIP)
Prepared by
Lauri E. Markowitz,1 MD, Eileen F. Dunne,
MD,1 Mona Saraiya, MD,2 Herschel W. Lawson,
MD,2 Harrell Chesson, PhD,1 Elizabeth R. Unger,
MD3
1Division of STD Prevention, National Center for HIV/AIDS, Viral Hepatitis, STD and TB Prevention (proposed)
2Division of Cancer Prevention and Control, National Center for Chronic Disease Prevention and Health Promotion
3Division of Viral and Rickettsial Diseases, National Center for Zoonotic, Vector-Borne and Enteric Diseases (proposed)
The material in this report originated in the National Center for HIV/AIDS, Viral Hepatitis, STD and TB Prevention (proposed), Kevin Fenton,
MD, Director, and the Division of STD Prevention, John Douglas, MD, Director.
Corresponding preparer: Lauri Markowitz, MD, National Center for HIV/AIDS, Viral Hepatitis, STD and TB Prevention (proposed), 1600 Clifton
Road, N.E., MS E02, Atlanta, GA 30333. Telephone: 404-639-8359; Fax: 404-639-8610; E-mail:
lem2@cdc.gov.
Summary
These recommendations represent the first statement by the Advisory Committee on Immunization Practices (ACIP) on
the use of a quadrivalent human papillomavirus (HPV) vaccine licensed by the U.S. Food and Drug Administration on June
8, 2006. This report summarizes the epidemiology of HPV and associated diseases, describes the licensed HPV vaccine,
and provides recommendations for its use for vaccination among females aged 9--26 years in the United States.
Genital HPV is the most common sexually transmitted infection in the United States; an estimated 6.2 million persons
are newly infected every year. Although the majority of infections cause no clinical symptoms and are self-limited,
persistent infection with oncogenic types can cause cervical cancer in women. HPV infection also is the cause of genital warts and
is associated with other anogenital cancers. Cervical cancer rates have decreased in the United States because of widespread
use of Papanicolaou testing, which can detect precancerous lesions of the cervix before they develop into cancer;
nevertheless, during 2007, an estimated 11,100 new cases will be diagnosed and approximately 3,700 women will die from
cervical cancer. In certain countries where cervical cancer screening is not routine, cervical cancer is a common cancer in women.
The licensed HPV vaccine is composed of the HPV L1 protein, the major capsid protein of HPV. Expression of the
L1 protein in yeast using recombinant DNA technology produces noninfectious virus-like particles (VLP) that resemble
HPV virions. The quadrivalent HPV vaccine is a mixture of four HPV type-specific VLPs prepared from the L1 proteins of HPV
6, 11, 16, and 18 combined with an aluminum adjuvant. Clinical trials indicate that the vaccine has high efficacy
in preventing persistent HPV infection, cervical cancer precursor lesions, vaginal and vulvar cancer precursor lesions, and
genital warts caused by HPV types 6, 11, 16, or 18 among females who have not already been infected with the respective HPV
type. No evidence exists of protection against disease caused by HPV types with which females are infected at the time
of vaccination. However, females infected with one or more vaccine HPV types before vaccination would be protected
against disease caused by the other vaccine HPV types.
The vaccine is administered by intramuscular injection, and the recommended schedule is a 3-dose series with the
second and third doses administered 2 and 6 months after the first dose. The recommended age for vaccination of females is
11--12 years. Vaccine can be administered as young as age 9 years. Catch-up vaccination is recommended for females aged
13--26 years who have not been previously vaccinated. Vaccination is not a substitute for routine cervical cancer screening,
and vaccinated females should have cervical cancer screening as recommended.
Introduction
Genital human papillomavirus (HPV) is the most common sexually transmitted infection in the United States;
an estimated 6.2 million persons are newly infected every year
(1). Although the majority of infections cause no symptoms
and are self-limited, persistent genital HPV infection can cause cervical cancer in women and other types of anogenital
cancers and genital warts in both men and women.
Approximately 100 HPV types have been identified, over 40 of which infect the genital area
(2). Genital HPV types are categorized according to their epidemiologic association with cervical cancer. Infections with low-risk types (e.g., types 6
and
11) can cause benign or low-grade cervical cell changes, genital warts, and recurrent respiratory papillomatosis.
High-risk HPV types act as carcinogens in the development of cervical cancer and other anogenital cancers
(3,4). High-risk types, including types 16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 68, 69, 73, and 82, can cause low-grade cervical
cell abnormalities, high-grade cervical cell abnormalities that are precursors to cancer, and anogenital cancers
(5). High-risk HPV types are detected in 99% of cervical cancers
(6); approximately 70% of cervical cancers worldwide are caused by types
16 and 18 (7). Although infection with high-risk types is considered necessary for the development of cervical cancer, it is
not sufficient because the majority of women with high-risk HPV infection do not develop cancer
(3,4).
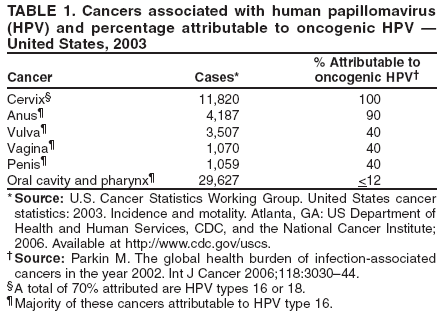
In addition to cervical cancer, HPV infection also is associated with anogenital cancers such as cancer of the vulva,
vagina, penis, and anus (Table 1)
(8,9).Each of these is less common than cervical cancer
(10--14). The association of genital types
of HPV with nongenital cancer is less well established, but studies support a role in a subset of oral cavity and
pharyngeal cancers (15).
In June 2006, the quadrivalent HPV vaccine types 6,11,16,18
(GARDASILTM,manufactured by Merck and Co.,
Inc., Whitehouse Station, New Jersey) was licensed for use among females aged 9--26 years* for prevention of vaccine
HPV-type--related cervical cancer, cervical cancer precursors, vaginal and vulvar cancer precursors, and anogenital warts.
Efficacy studies are ongoing in men.
In the United States, cervical cancer prevention and control programs have reduced the number of cervical cancer cases
and deaths through cervical cytology screening, which can detect precancerous lesions. The quadrivalent HPV vaccine will
not eliminate the need for cervical cancer screening in the United States because not all HPV types that cause cervical cancer
are included in the vaccine.
Methods
The Advisory Committee on Immunization Practices (ACIP) HPV vaccine workgroup first met in February 2004 to
begin reviewing data related to the quadrivalent HPV vaccine. The workgroup held monthly teleconferences and meetings
three times a year to review published and unpublished data from the HPV vaccine clinical trials, including data on
safety, immunogenicity, and efficacy. Data on epidemiology and natural history of HPV, vaccine acceptability, and sexual
behavior in the United States also were reviewed. Several economic and cost effectiveness analyses were considered. Presentations
on these topics were made to ACIP during meetings in June 2005, October 2005, and February 2006. Recommendation
options were developed and discussed by the ACIP HPV vaccine workgroup. When evidence was lacking, the
recommendations incorporated expert opinion of the workgroup members. Options being considered by the workgroup were presented
to ACIP in February 2006. The final recommendations were presented to ACIP at the June 2006 ACIP meeting.
After discussions, minor modifications were made and the recommendations were approved at the June 2006
meeting. Modifications were made to the ACIP statement during the subsequent review process at CDC to update and clarify
wording in the document.
The quadrivalent HPV vaccine is a new vaccine; additional data will be available in the near future from clinical
trials. These data and any new information on epidemiology of HPV will be reviewed by ACIP as they become available,
and recommendations will be updated as needed.
Background
Biology of HPV
HPVs are nonenveloped, double-stranded DNA viruses in the family
Papillomaviridae. Isolates of HPV are classified
as "types," and numbers are assigned in order of their discovery
(16).Types are designated on the basis of the
nucleotide sequence of specific regions of the
genome. All HPVs have an 8 kb circular genome enclosed in a capsid shell composed
of the major and minor capsid proteins L1 and L2, respectively. Purified L1 protein will self-assemble to form empty shells
that resemble a virus, called virus-like particles (VLPs). In addition to the structural genes (L1 and L2), the genome
encodes several early genes (E1, E2, E4, E5, E6, and E7) that enable viral transcription and replication and interact with the
host
genome. Immortalization and transformation functions are associated with the E6 and E7 genes of high-risk HPV. E6 and
E7 proteins from high-risk types are the primary oncoproteins; they manipulate cell cycle regulators, induce
chromosomal abnormalities, and block apoptosis
(17).
Papillomaviruses initiate infection in the basal layer of the epithelium, and viral genome amplification occurs
in differentiating cells using the cellular replication machinery. After infection, differentiating epithelial cells that are
normally nondividing remain in an active cell cycle. This can result in a thickened, sometimes exophytic, epithelial lesion. The virus
is released as cells exfoliate from the epithelium. With neoplastic progression, the virus might integrate into the
host chromosomes, and little virion production will occur.
Immunology of HPV
HPV infections are largely shielded from the host immune response because they are restricted to the epithelium
(18). Humoral and cellular immune responses have been documented, but correlates of immunity have not been established.
Serum antibodies against many different viral products have been demonstrated. The best characterized and most
type-specific antibodies are those directed against conformational epitopes of the L1 capsid protein assembled as VLPs. Not all
infected persons have antibodies; in one study, 54%--69% of women with incident HPV 16, 6, or 18 infections had antibodies
(19). Among newly infected women, the median time to seroconversion is approximately 8 months
(20,21).
Laboratory Testing for HPV
HPV cannot be cultured. Detecting HPV requires identification of HPV genetic information (DNA in the majority
of assay formats). Assays differ considerably in their sensitivity and type specificity. The anatomic region sampled and
the method of specimen collection will impact detection.
Only the Digene Hybrid Capture® 2 (HC2) High-Risk HPV DNA Test is approved by the U.S. Food and
Drug Administration (FDA) for clinical use. The HC2 High Risk test uses liquid nucleic acid hybridization and detects 13
high-risk types (HPV 16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, and 68). Results are reported as positive or negative and
are not type-specific. The HC2 High Risk test is approved for triage of women with equivocal Papanicolaou (Pap) test
results (atypical squamous cells of undetermined significance [ASC-US]) and in combination with the Pap test for cervical
cancer screening in women aged >30 years. The test is not clinically indicated nor
approved for use in men.
Epidemiology and basic research studies of HPV typically use nucleic acid amplification methods that generate
type-specific and, in certain formats, quantitative results. Polymerase chain reaction (PCR) assays used most commonly in
epidemiologic studies target genetically conserved regions of the L1 gene. These consensus assays are designed to amplify HPV, and types
are then determined by type specific hybridization, restriction enzyme digestion, or sequencing. In the trials of quadrivalent
HPV vaccine, multiplex assays were used that specifically detect the L1, E6, and E7 gene for each HPV type.
The most frequently used HPV serologic assays are VLP-based enzyme immunoassays, designed to detect antibodies to
the L1 viral protein. The type-specificity of the assay depends on preparation of conformationally intact VLPs in
recombinant baculovirus or other eukaryotic expression systems
(22). Serologic assays are available only in research settings. Key
laboratory reagents are not standardized, and no gold standards exist for setting a threshold for a positive result
(23). In trials of the quadrivalent HPV vaccine, a competitive radioimmunoassay or a quadriplex competitive immunoassay was used, both
of which measure neutralizing antibodies in serum
(24,25).
Epidemiology of HPV Infection
Transmission and Risk Factors
Genital HPV infection is primarily transmitted by genital contact, usually through sexual intercourse
(2,26). In virtually all studies of HPV prevalence and incidence, the most consistent predictors of infection have been measures of sexual
activity, most importantly the number of sex partners (lifetime and recent)
(27--34). For example, one study indicated that 14.3%
of women aged 18--25 years with one lifetime sex partner, 22.3% with two lifetime sex partners, and 31.5% with more
than three lifetime partners (33) had HPV infection. Transmission of HPV through other types of genital contact in the absence
of penetrative intercourse (i.e., oral-genital, manual-genital, and genital-genital contact) has been described, but is less
common
than through sexual intercourse (26,35,36). Additional risk factors primarily identified for females include partner
sexual behavior (26) and immune status
(37,38). Genital HPV infection also can be transmitted by nonsexual routes, but this
is uncommon. Nonsexual routes of genital HPV transmission include transmission from a mother to a newborn baby
(39,40).
Because HPV is transmitted by sexual activity, understanding the epidemiology of HPV requires data on sexual
behavior. The 2002 National Survey of Family Growth (http://www.cdc.gov/nchs/nsfg) indicated that 24% of females in the
United States were sexually active by age 15 years
(41). This percentage increased to 40% by age 16 years and to 70% by age 18
years. Among sexually active females aged 15--19 years and 20--24 years, the median number of lifetime male sex partners was
1.4 and 2.8, respectively (42). The 2005 Youth Behavioral Risk Survey
(http://www.cdc.gov/mmwr/preview/mmwrhtml/SS5505a1.htm) indicated that that 3.7% of female students had been sexually active before age 13 years
(43). Of those sexually active, 5.7% of 9th-grade females and 20.2% of 12th-grade females had had four or more sex
partners.
Natural History of HPV Infection
The majority of HPV infections are transient and asymptomatic and cause no clinical problems; 70% of new
HPV infections clear within 1 year, and approximately 90% clear within 2 years
(27,44--46). The median duration of new infections is 8 months
(27,45). Persistent infection with high-risk types of HPV is the most important risk factor for
cervical cancer precursors and invasive cervical
cancer(45,47--50). The risk for persistence and progression to precancerous
lesions varies by HPV type, with HPV 16 being more oncogenic than other high-risk HPV types
(51,52). Factors associated with cervical cancer in epidemiologic studies include cigarette smoking, increased parity, increased age, other sexually
transmitted infections, immune suppression, long-term oral contraceptive use, and other host factors
(53--55). The time between initial HPV infection and development of cervical cancer is usually decades. Many aspects of the natural history of HPV are
poorly understood, including the role and duration of naturally acquired immunity after HPV infection.
HPV Prevalence and Incidence in the United States
Overall in the United States, an estimated 6.2 million new HPV infections
occur every year among persons aged 14--44 years
(1). Of these, 74% occur among those aged 15--24 years. Modeling estimates suggest that >80% of sexually active women
will have acquired genital HPV by age 50 years
(56).
Routine reporting of HPV does not exist in the United States. Information on prevalence and incidence has been
obtained primarily from clinic-based populations, such as family planning and sexually transmitted disease or university health
clinic patients. These evaluations have documented prevalence of HPV DNA ranging from 14% to 90%
(57). Prevalence was highest among sexually active females aged <25 years and decreased with increasing age
(31,32,58,59). Data from a multisite, clinic-based study of sexually active women in the United States indicated that prevalence was highest among those aged
14--19 years (60).
Two studies have reported prevalence in representative, population-based samples. In a study of sexually active women
aged 18--25 years, prevalence of any HPV was 26.9%
(33).Prevalence of types 6 or 11 was 2.2%, and prevalence of types 16 or
18 was 7.8%. In a study of females aged 14--59 years during 2003--2004, the prevalence of any HPV was 26.8%
(61). Prevalence was highest among women aged 20--24 years (44.8%). Overall, prevalence of types 6, 11, 16, and 18 was
1.3%, 0.1%, 1.5%, and 0.8%, respectively.
Few data exist on cumulative risk for HPV infection. Detection of HPV DNA indicates infection and does not
provide information on women who were infected but cleared the HPV. Seroprevalence data can provide a better estimate
of cumulative risk but will also be an underestimate, because not all persons with natural HPV infection have
detectable antibodies. In a representative sample of women aged 20--29 years in the United States, HPV 16 seroprevalence was
25% (62). Because as few as 60% of those infected with HPV have detectable antibodies, the seroprevalence is an
underestimate, and true exposure to HPV 16 could be as high as 41% among women in that age group. Data also are available from
the quadrivalent HPV vaccine phase III trials, in which both HPV PCR assays on cervical specimens and serologic tests
were performed at enrollment. Participation was restricted to sexually active women who had no more than four lifetime
partners or were planning sexual debut. Among 5,996 North American females aged 16--24 years, 92% were sexually active, and
the median number of lifetime sex partners was two; 24% had evidence of previous or current infection with HPV
6,11,16, or 18 on the basis of serology and/or PCR at the time of enrollment; four (0.1%) had evidence of infection with all four vaccine
types (Merck and Co., unpublished data, 2006).
Studies of incident HPV infection that have evaluated HPV DNA detection over time demonstrate that acquisition
occurs soon after sexual debut. In a prospective study of college women in the United States, the cumulative probability of
incident infection was 38.9% by 24 months after first sexual intercourse. Of all HPV types, HPV 16 acquisition was highest
(10.4%); 5.6% had acquired HPV 18 (26).
HPV infection also is common among men
(63--67).Among heterosexual men in clinic-based studies, prevalence of
genital HPV infection often is >20% and is highly dependent on the anatomic sites sampled and method of
specimen collection (64,66,67).
Clinical Sequelae of HPV Infection
Clinical sequelae of HPV infection include cervical cancer and cervical cancer precursors, other anogenital cancers and
their precursor lesions, anogenital warts, and recurrent respiratory papillomatosis.
Cervical Cancer and Precursor Lesions
HPV is a necessary but not sufficient cause of all cervical cancers. Approximately three fourths of all cervical cancers in
the United States are squamous cell; the remaining are
adenocarcinomas. HPV 16 and 18 account for approximately 68%
of squamous cell cancers and 83% of adenocarcinomas
(7).
Although HPV infection usually is asymptomatic, cervical infection can result in histologic changes that are classified
as cervical intraepithelial neoplasias (CIN) grades 1, 2, or 3 on the basis of increasing degree of abnormality in the
cervical epithelium or adenocarcinoma in situ (AIS). Spontaneous clearance or progression to cancer in the absence of
treatment varies for CIN 1 and CIN 2, and CIN 3. CIN 1 usually clears spontaneously (60% of cases) and rarely progresses to
cancer (1%); a lower percentage of CIN 2 and 3 spontaneously clears (30%--40%), and a higher percentage progresses to cancer
if not treated (>12%) (68). Cervical cancer screening with the Pap test can detect cytologic changes that reflect the
underlying tissue changes. However, cytologic abnormalities detected by the Pap test can be ambiguous or equivocal.
Abnormalities include ASC-US, atypical glandular cells, low- and high-grade squamous intraepithelial lesions (LSIL and HSIL), and
AIS. HPV types 16 and 18 are more commonly found in association with higher-grade lesions. In one study, the prevalence
of HPV 16 was 13.3% among ASC-US, 23.6% among LSIL, and 60.7% among HSIL Pap tests
(69).
No routine reporting or registry exists for abnormal Pap tests or cervical cancer precursor lesions in the United
States; however, data are available from managed-care organizations and administrative data sets
(70,71).Each year,
approximately 50 million women undergo Pap testing; approximately 3.5--5.0 million of these Pap tests will require some
follow-up, including 2--3 million ASC-US, 1.25 million LSIL, and 300,000 HSIL Pap tests
(72--74).
In the United States, cases of cervical cancer are routinely reported to cancer registries such as the National Cancer
Institute Surveillance, Epidemiology, and End Results program, and CDC-administered National Program of Cancer Registries
that cover approximately 96% of the U.S. population in 2003. Cervical cancer incidence rates have decreased approximately
75% and death rates approximately 70% since the 1950s, largely because of the introduction of Pap testing
(74,75). However, the decrease in incidence is observed primarily in squamous cell carcinomas; the incidence of adenocarcinomas has not
changed appreciably (76). Adenocarcinomas are more difficult to detect because they are found in the endocervix; they account
for approximately 20% of cervical cancer cases in the United States
(77,78). In 2003, cervical cancer incidence in the
United States was 8.1 per 100,000 women, with approximately 11,820 new cases reported
(79). The median age of diagnosis for cervical cancer was 47 years.
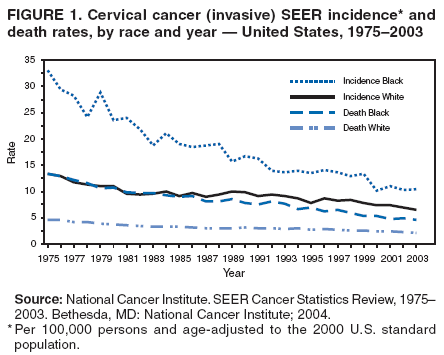
Substantial differences exist in the cervical cancer incidence and mortality by racial/ethnic group in the United States
(78). The incidence for black women was approximately 1.5 times higher than that for white women
(Figure 1). Incidence for Hispanic women also was higher than that for white women
(78). Death rates for black women were twice that for
white women. Although incidence for Asian women overall is similar to that for white women
(78), certain Asian subgroups, especially Vietnamese and Korean women, have higher rates of cervical cancer
(80).
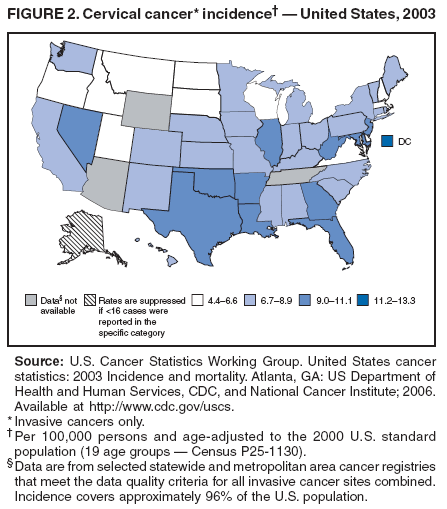
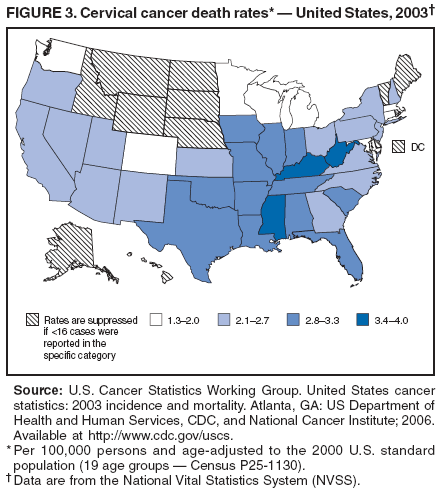
Geographic differences exist in incidence and mortality, with notably higher incidence and mortality in Southern
states (Figures 2 and 3) and Appalachia
(78,81). Mortality rates are higher among specific groups, including Hispanic women
living on the Texas-Mexico border; white women in Appalachia, rural New York State, and the northern part of the
northeast United States; and among American Indians in the Northern Plains and Alaska Native women
(82).
Vaginal and Vulvar Cancer and Precursor Lesions
HPV is associated with vaginal and vulvar cancer and vaginal and vulvar intraepithelial neoplasias; however, unlike
cervical cancer, not all vaginal and vulvar cancers are associated with HPV. The natural history of vaginal and vulvar neoplasia
is incompletely understood (83,84). No routine screening exists for vaginal or vulvar cancer in the United States.
The majority of vaginal cancers and vaginal intraepithelial neoplasias III (VaIN III) are positive for HPV
(85); HPV 16 is the most common type
(86,87). Approximately one third of women with
VaIN or vaginal cancer had been treated previously for an anogenital cancer, usually cervical cancer
(86). Vaginal cancer is rare, and incidence has decreased by 20% during
the preceding two decades. In the United States in 2003, a total of 1,070 cases of invasive vaginal cancer (age-adjusted
incidence rate: 0.7 per 100,000 females) and 391 deaths (death rate: 0.2 per 100,000 females) occurred
(79). The median age for diagnosis of vaginal cancer was 69 years.
HPV is associated with approximately half of vulvar squamous cell cancers, the most common type of vulvar cancer.
HPV-associated vulvar cancer tends to occur in younger women and might be preceded by vulvar intraepithelial neoplasia
(VIN). In a recent study, HPV types 16 or 18 were detected in 76% of the VIN 2/3 and 42% of vulvar carcinoma samples
(87). In 2003, a total of 3,507 cases of vulvar cancer (age-adjusted incidence rate: 2.2 per 100,000) and 775 deaths (death rate: 0.4
per 100,000 females) occurred in the United States
(79). During 1973--2000, the incidence of in situ vulvar cancer increased
by 400%, and the rate of invasive vulvar cancer increased by 20%. Changes in detection or reporting of in situ cancers might
be responsible for the increased rate of in situ cancers
(88).
Anal Cancer
HPV is associated with approximately 90% of anal squamous cell cancers. Anal intraepithelial neoplasia (AIN)
is recognized as a precursor of anal cancer, although the natural history of these lesions (i.e., rate of progression and
regression) is less clear than for CIN (50). Anal cancer is more common in women (2,516 new cases in 2003 [rate: 1.6 per
100,000 women]) than in men (1,671 new cases [rate: 1.3 per 100,000 men])
(79). During the preceding three decades, the
incidence of anal cancer in the United States has increased, especially among men
(89). Women at high risk for anal cancer
include those with high-grade cervical lesions and cervical and vulvar cancers. Men who have sex with men and
persons who have human immunodeficiency virus (HIV) infection also are at high risk for anal cancer
(90). No national recommendations exist for cytologic screening to prevent anal
cancers.
Genital Warts
All anogenital warts (condyloma) are caused by HPV, and approximately 90% are associated with HPV types 6 and
11 (91). The average time to development of new anogenital warts after infection with HPV types 6 or 11 is approximately
2--3 months (92). However, not all persons infected with HPV types 6 or 11 acquire genital warts. Anogenital warts can
be treated, although many warts (20%--30%) regress spontaneously. Recurrence of anogenital warts is common
(approximately 30%), whether clearance occurs spontaneously or following treatment
(93). Anogenital warts are not routinely reported in
the United States. The prevalence of genital warts has been examined using health-care claims data
(94). An estimated 1% of sexually active adolescents and adults in the United States have clinically apparent genital warts
(29).
Recurrent Respiratory Papillomatosis
Infection with low-risk HPV types, primarily types 6 or 11, rarely results in recurrent respiratory papillomatosis (RRP),
a disease that is characterized by recurrent warts or papillomas in the upper respiratory tract, particularly the larynx. On
the basis of age of onset, RRP is divided into juvenile onset (JORRP) and adult onset forms. JORRP, generally defined as
onset before age 18 years, is better characterized than the adult form. JORRP is believed to result from vertical transmission
of HPV from mother to baby during delivery, although the median age of diagnosis is 4 years. A multicenter registry of
JORRP in the United States that collected data during 1999--2003
(95) demonstrated that although the clinical course of JORRP
was variable, it is associated with extensive morbidity, requiring a median of 13 lifetime surgeries to remove warts and maintain
an open airway. Estimates of the incidence of JORRP are relatively imprecise but range from 0.12 to 2.1 cases per
100,000 children aged <18 years in two cities in the United States
(96). The prevalence, incidence, and disease course of the
adult form of RRP are less clear.
Treatment of HPV Infection
HPV infections are not treated; treatment is directed at the HPV-associated lesions. Treatment options for genital warts
and cervical, vaginal, and vulvar cancer precursors include various local approaches that remove the lesion (e.g.,
cryotherapy, electrocautery, laser therapy, and surgical excision). Genital warts also are treated with topical pharmacologic agents
(97). On the basis of limited existing data, available therapies for HPV-related lesions might reduce but probably do not
eliminate infectiousness.
Prevention
HPV Infection
Condom use might reduce the risk for HPV and HPV-associated diseases (e.g., genital warts and cervical cancer). A
limited number of prospective studies have demonstrated a protective effect of condoms on acquisition of genital HPV. A
study among newly sexually active college women demonstrated a 70% reduction in HPV infection when their partners
used condoms consistently and correctly (98). Abstaining from sexual activity (i.e., refraining from any genital contact
with another persons) is the surest way to prevent genital HPV infection. For those who choose to be sexually active,
a monogamous relationship with an uninfected partner is the strategy most likely to prevent future genital HPV infections.
Neither routine surveillance for HPV infection nor partner notification is useful for HPV prevention
(97). Genital HPV infection is so prevalent that the majority of partners of persons found to have HPV infection are infected already;
no prevention or treatment strategies have been recommended for partners.
Cervical Cancer Screening
The majority of cervical cancer cases and deaths can be prevented through detection of pre-cancerous changes in the cervix
by cytology using the Pap test. Pap test screening includes a conventional Pap or a liquid-based cytology
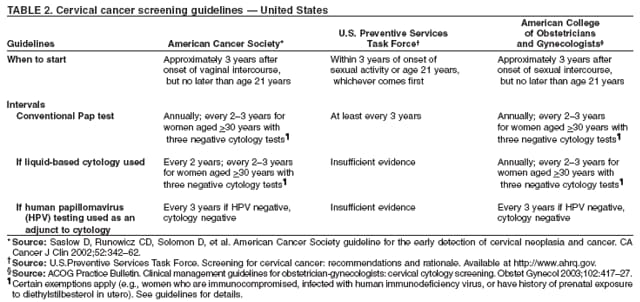
(99). CDC does not issue recommendations for cervical cancer screening, but certain professional groups have published recommendations
(Table 2). The American College of Obstetricians and Gynecologists (ACOG), the American Cancer Society (ACS), and the U.S.
Preventive Services Task Force (USPSTF) guidelines state that all women should have a Pap test for cervical cancer screening within
3 years of beginning sexual activity or by age 21 years, whichever occurs first (Table 2)
(74,100,101). USPSTF recommends a conventional Pap test at least every 3 years, regardless of age. ACOG recommends annual screening of women aged <30
years; ACS recommends annual or biennial screening in this age group, depending on use of conventional or liquid-based
cytology. According to these national organizations, women aged
>30 years with three normal consecutive Pap tests should be
screened every 2--3 years.
ACS and ACOG also recommend use of the HC2 High
Risk test as an adjunct to regular Pap screening of women
aged >30 years. If both tests are negative, women should be rescreened no more frequently than every 3 years. In
addition, ACOG and the American Society of Colposcopy and Cervical Pathology (ASCCP) recommend that HPV DNA testing
be used to triage women with equivocal, ASC-US Pap test results
(102).USPSTF concluded that evidence is insufficient
to recommend for or against routine use of HPV tests
(100).
An estimated 82% of women in the United States have had a Pap test during the preceding 3 years
(103). Pap test rates for all age and ethnic populations have increased during the preceding two decades. However, certain groups continue to
have lower screening rates. These include women with less than a high school education (77%); foreign-born women,
especially women who have been in the United States for <10 years (61%); women without health insurance (62%); and certain
racial/ethnic populations such as Hispanics (77%) and Asians (71%). Approximately half of women who had cervical
cancer diagnosed in the United States had not had a Pap test in the 3 years before diagnosis
(104).
Quadrivalent Human Papillomavirus Vaccine
Composition
The licensed vaccine is a quadrivalent HPV vaccine
(GARDASILTM,produced by Merck and Co, Inc.). The L1
major capsid protein of HPV is the antigen used for HPV vaccination
(105). Using recombinant DNA technology, the L1 protein
is
expressed in Saccharomyces cerevisiae (yeast), and the proteins self-assemble into conformationally intact, noninfectious
VLPs. Each 0.5-mL dose contains 20 µg HPV 6 L1 protein, 40
µg HPV 11 L1 protein, 40 µg HPV 16 L1 protein, and 20
µg HPV 18 L1 protein. VLPs are adsorbed on an aluminum-containing adjuvant. Each 0.5-mL dose contains 225
µg amorphous aluminum hydroxyphosphate sulfate. The formulation also includes sodium chloride, L-histidine, polysorbate 80,
sodium borate, and water for injection. The quadrivalent HPV vaccine contains no thimerosal or antibiotics.
The vaccine should be stored at 2°C--8°C (36°F--46°F) and not frozen.
Dose and Administration
Quadrivalent HPV vaccine is administered intramuscularly as three separate 0.5-mL doses. The second dose should
be administered 2 months after the first dose and the third dose 6 months after the first dose. The vaccine is available as a
sterile suspension for injection in a single-dose vial or a prefilled syringe.
Efficacy
One clinical study evaluated efficacy of monovalent HPV 16 vaccine, and three studies evaluated efficacy of
quadrivalent HPV vaccine: a phase II study of a monovalent HPV 16 vaccine (protocol 005)
(106,107), a phase II study of quadrivalent HPV vaccine (protocol 007)
(108--110), both among females aged 16--23 years, and two phase III studies of
quadrivalent HPV vaccine (protocols 013 and 015) among females aged 16--23 and 16--26 years, respectively. All were
randomized, double-blind, placebo-controlled studies.
The studies used prespecified endpoints to evaluate the impact of the quadrivalent vaccine in preventing
HPV-related infection and disease. Phase II studies were primarily proof-of-concept studies that evaluated the efficacy of vaccine using
a persistent infection endpoint. Phase III studies evaluated the efficacy of vaccine on clinical lesions. Predefined
combinations of phase II and III studies were used to improve the precision of the efficacy findings. Various endpoints were assessed in
the different studies, including vaccine type-related persistent HPV infection, CIN, VIN and VaIN, and genital warts.
The primary endpoint and the basis for licensure was the combined incidence of HPV 16- and 18-related CIN 2/3 or AIS.
These endpoints served as surrogate markers for cervical cancer. Studies using an invasive cervical cancer endpoint were not
feasible because the standard of care is to screen for and treat CIN 2/3 and AIS lesions to prevent invasive cervical
cancer. Furthermore, the time from acquisition of infection to the development of cancer can exceed 20 years. The two phase
III efficacy studies of quadrivalent HPV vaccine (protocols 013 and 015) were international studies, which included
persons from North America, South America, Europe, Australia, and Asia. Data on efficacy against CIN endpoints also are
available from the phase II study (protocol 007)
(108,110) and of monovalent HPV-16 vaccine (protocol 005)
(107).
The quadrivalent HPV vaccine has a high efficacy for prevention of vaccine HPV type HPV 6-, 11-, 16-, and
18-related persistent infection, vaccine type-related CIN, CIN 2/3, and external genital lesions (genital warts, VIN and
VaIN) when analyses were restricted to participants who received all 3 doses of vaccine, had no protocol violations, and no
evidence of infection with the relevant vaccine HPV type (seronegative and HPV PCR-negative through 1 month after dose
3) (Tables 3 and 4) (111). No evidence exists of protection against disease caused by vaccine types for which participants
were PCR positive at baseline. Participants infected with one or more vaccine HPV types before vaccination were protected
against disease caused by the other vaccine HPV types. No evidence exists that the vaccine protects against disease caused
by nonvaccine HPV types.
Persistent HPV Infection
Two phase II studies evaluated persistent infection, defined as a vaccine HPV type detected by PCR at two or
more consecutive visits 4 months apart or at a single visit if it was the last visit of record. In the phase II quadrivalent vaccine
study (protocol 007), 276 women received the 20/40/40/20
µg dose formulation of vaccine, and 275 received a placebo. The
efficacy for prevention of persistent HPV 6, 11, 16, or 18 infection or disease at the end of study (approximately 2.5 years after dose
3) was 89.5% (95% confidence interval [CI] = 70.7%--97.3%). Of the vaccinated persons with persistent infection
endpoints, three had HPV 16 detected at the last visit (without observed persistence), and one had persistent infection with HPV
18 (detected at both 12 and 18 months) but not at months 24, 30, or 36
(108).In the phase II study of a monovalent HPV
16 vaccine (protocol 005), the efficacy against persistent HPV 16 infection was 100% at a midpoint analysis
(106) and 94.3% (CI =
87.8%--97.7%) at the end of the study (107). All seven cases in the vaccine group had HPV 16 DNA detected on the
person's last study visit (without observed persistence).
Cervical Disease
Two phase III trials evaluated efficacy against cervical disease. Protocol 015 included 12,157 women aged 16--26
years. Participants had a Pap test, cervicovaginal sampling for HPV DNA testing, and detailed genital inspection at day 1 and months
7, 12, 24, 36, and 48, and were referred to colposcopy using a protocol specified algorithm based on Pap test results. The
primary study endpoint was incidence of HPV 16- or
18-related CIN 2, CIN 3, AIS, or cervical cancer. In a per protocol analysis,
the vaccine efficacy was 100% (CI = 80.9%--100%) for prevention of HPV 16 or 18 related
CIN 2/3 or AIS (Table 3).
Protocol 013 included 5,442 females aged 16--23 years. Participants had a Pap test at day 1 and at months 7, 12, 18,
24, 30, 36, and 48 and were referred to colposcopy according to protocol. In addition, participants had detailed
genital inspection, with biopsy of abnormalities and cervicovaginal sampling for HPV DNA sampling. The study had two
primary efficacy endpoints: 1) external genital lesions related to HPV 6, 11, 16, or 18, including genital warts, VIN, VaIN,
vulvar cancer, or vaginal cancer; and 2) cervical endpoints related to HPV 6, 11, 16, or 18, including CIN, AIS, or cervical
cancer. In a per protocol analysis, the vaccine efficacy was 100% (CI = 89.5%--100%) for prevention of any grade CIN related
to vaccine types (Table 3).
In a planned combined efficacy analysis, including data from four clinical studies (protocol 005, 007, 013, and
015), protection against HPV 16- or 18-related CIN 2/3 or AIS was
100% (CI = 92.9%--100%) (111). In a planned
combined analysis, including data from three studies (protocol 007, 013, and 015), protection against any CIN attributed to HPV 6, 11,
16, or 18, the efficacy was 95.2% (CI = 87.2%--98.7%). Four cases of CIN occurred in the vaccine group; all were CIN 1.
External Genital Lesions
Data from three studies (protocol 007, 013, and 015) provide data on efficacy against external genital lesions. In
a combined analysis, the efficacy of quadrivalent HPV vaccine against HPV 6-, 11-, 16-, or 18-related external genital
warts was 98.9% (CI = 93.7%--100%) in a per protocol analysis
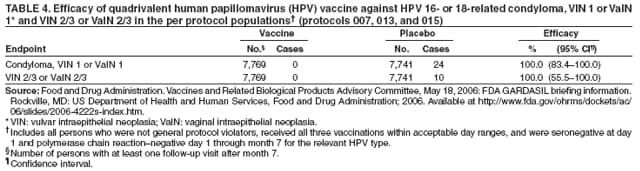
(Table 3). Efficacy against HPV 16- or 18-related VIN 2/3
or VaIN 2/3 was 100% (CI = 55.5--100.0) (Table 4).
Efficacy in Females with Current or Previous Vaccine HPV-Type Infection
Because participants were enrolled into the clinical trials even if they were HPV DNA or antibody positive,
evaluating efficacy in females infected with a vaccine HPV type at the time of vaccination was possible. Overall, 27% of the
study population had evidence of previous exposure to or infection with a vaccine HPV type. Among these participants, 74%
were positive to only one vaccine HPV type and did not have evidence of infection with the other three types. Among
participants positive to one or more vaccine HPV types, the vaccine had high efficacy for prevention of disease caused by the
remaining vaccine HPV types (112).
The vaccine's impact on the course of infection present at the time of infection was evaluated using data from four
clinical studies (protocols 005, 007, 013, and 015). Three different groups were analyzed on the basis of antibody and HPV
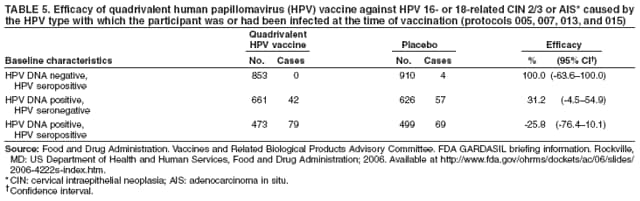
DNA detection at the time of vaccination (Table 5). Among persons seropositive to the relevant HPV type but HPV DNA
negative, efficacy against CIN 2/3 or AIS caused by that type was 100% (CI = -63.6%--100%). Among women who were HPV
DNA positive but seronegative, efficacy was 31.2%
(CI = -4.5--54.9). Among women who were both seropostive
and HPV DNA positive, efficacy against CIN 2/3 caused by that type was -25.8% (CI = -76.4%--10.1%). Because of the small numbers and
wide confidence intervals around efficacy estimates, limited conclusions can be drawn from these
estimates.
Efficacy in the Intent-to-Treat Population
Analyses among all women who received at least 1 dose of vaccine and had any follow-up 1 month after the first
dose, regardless of initial PCR or serology, provide information on efficacy that would be seen in the total study population.
At baseline, 27% of clinical trial participants had evidence of previous or current infection with a vaccine type HPV. In
a combined analysis of protocols 005, 007, 013, and 015, the efficacy for prevention of HPV 16- or 18-related CIN 2/3 or
AIS was 39.0% (CI = 23.3%--51.7%). In a combined analysis of protocols 007, 013 and 015, efficacy for prevention of
any vaccine-type--related CIN was 46.4% (CI = 35.2%--55.7%), for prevention of
vaccine-type--related VIN 2/3 and VaIN 2/3 was 69.1% (CI = 29.8%--87.9%), and for prevention of
vaccine- type--related genital warts was 68.5% (CI =
57.5%--
77.0%). The lower efficacy in these analyses compared with the per protocol population indicates that certain women
were infected with vaccine types before vaccination. A 12.2% (CI = -3.2%--25.3%) reduction occurred in any CIN 2/3 in
the vaccinated group compared with the placebo group at a median follow-up time of 1.9 years
(111).
Duration of Protection
A subset of participants (n = 241) in the phase II quadrivalent HPV vaccine study
(protocol 007) is being followed for 60 months after dose one. In a combined analysis of all participants through year 3 and a subset through 60 months, the
efficacy against vaccine HPV type persistent infection or disease was
95.8% (CI = 83.8%--99.5%) and efficacy against
vaccine-type--related CIN or external genital lesions was 100% (CI =
12.4%--100%) (110).
Follow-up studies are planned by Merck and Co., Inc. to determine duration of protection among women enrolled in
the phase III studies through 3 years after dose 3. Additional data on duration of protection will be available from follow-up
of approximately 5,500 women enrolled in one of the phase III quadrivalent HPV vaccine studies in the Nordic
countries. These women will be followed for at least 14 years; serologic testing will be conducted 5 and 10 years after vaccination;
and Pap testing results will be linked to data from vaccine registries to monitor outcomes.
Immunogenicity
Immunogenicity in Persons Aged 9--26 Years
The immunogenicity of the quadrivalent HPV vaccine has been measured by detection of IgG antibody to the HPV L1
by a type-specific competitive Luminex-based immunoassay (cLIA) in the majority of the studies
(24,25). This assay measures antibodies against neutralizing epitopes for each HPV type. The units (milliMerck units) are internally consistent but
cannot be directly compared across HPV types or with results from other HPV antibody assays. The height of the antibody
titers (geometric mean titers [GMTs]) for the different types cannot be directly compared.
Data on immunogenicity are available from Phase II
(109) and Phase III double-blind, randomized,
placebo-controlled trials conducted among females aged 16--26 years and immunogenicity studies conducted among males and females aged
9--15 years (113). In all studies conducted to date,
>99% of study participants had an antibody response to all four HPV
types in the vaccine 1 month after completing the 3-dose series
(109,113). High seropositivity rates were observed after
vaccination regardless of sex, ethnicity, country of origin, smoking status, or body mass index.
Vaccination produced antibody titers higher than those after natural infection. Among females aged 16--23 years,
anti-HPV 6, 11, 16, and 18 GMTs 1 month after the third dose of vaccine were higher than those observed in participants
who were HPV seropositive and PCR negative at enrollment in the
placebo group (109).
Vaccination of females who were seropositive to a specific vaccine HPV type at enrollment resulted in higher antibody
titers to that type, particularly after the first dose, compared with those seronegative at enrollment
(109), suggesting a boosting of naturally acquired antibody by vaccination. In studies among females aged 16--26 years, the interval between the first
and second dose of vaccine ranged from 6 to 12 weeks.
Variation in the interval did not diminish the GMTs
post-vaccination. Likewise, little impact of intervals was observed between the second and third dose ranging from 12 to 23 weeks.
A serologic correlative of immunity has not been identified and no known minimal titer determined to be protective.
The high efficacy found in the clinical trials to date has precluded identification of a minimum protective antibody titer.
Further follow-up of vaccinated cohorts might allow determination of serologic correlates of immunity.
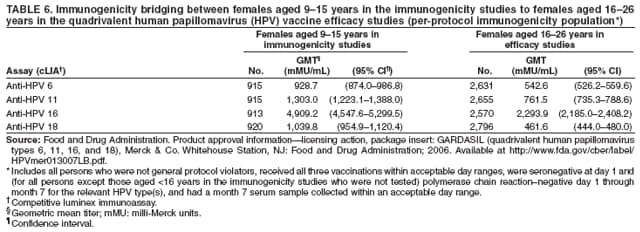
Immunogenicity Bridge to Efficacy Among Females
Immunogenicity studies provide data, allowing comparison of seropositivity and GMTs among females aged 9--15
years with those among females aged 16--26 years who were in the efficacy studies (Table 6)
(111). Seropositivity rates in all age groups were approximately 99% for HPV 6, 11, 16, and 18. Anti-HPV responses 1 month post dose 3 among females
aged 9--15 years were noninferior to those aged 16--26 years. At month 18, anti-HPV GMTs in females aged 9--15 years
remained two to three fold higher than those observed at the same time point in females aged 16--26 years in the vaccine efficacy trials.
Duration of Antibody
The longest follow-up to date is 60 months in the phase II trial of quadrivalent HPV vaccine
(110). Antibody titers decline over time after the third dose but plateau by 24 months. At 36 months, anti-HPV 16 GMT among vaccinees
remained higher than those in participants in the placebo group who were seropositive at baseline, and anti-HPV 6, 11, and 18
titers were similar to those seropositive in the placebo group
(109). At 36 months, seropositivity rates were 94%, 96%, 100%,
and 76% to HPV 6, 11, 16, and 18, respectively. No evidence exists of waning efficacy among participants who
become seronegative during follow-up (110). Data from a revaccination study in which vaccinated women were given a challenge
dose 5 years after enrollment into the study demonstrated an augmented rise in antibody titer consistent with immune
memory (114).
Concomitant Administration of HPV Vaccine with Other Vaccines
GMTs after concomitant administration of quadrivalent HPV vaccine and hepatitis B vaccine at all 3 doses
were noninferior to GMTs after administration at separate visits. Studies are planned to evaluate concomitant administration
with meningococcal conjugate vaccine and with the
adolescent/adult formulation of tetanus, diphtheria and
acellular pertussis (Tdap) vaccine.
Safety and Adverse Events
The quadrivalent HPV vaccine was evaluated for injection-site and systemic adverse events, new medical
conditions reported during the follow-up period, and safety during pregnancy and lactation. Safety data on quadrivalent HPV
vaccine are available from seven clinical trials and include 11,778 persons aged 9--26 years who received quadrivalent vaccine
and 9,686 who received placebo. Detailed data were collected using vaccination report cards for 14 days following each
injection of study vaccine on a subset of participants aged 9--23 years. The population with detailed safety data included 5,088
females who received quadrivalent HPV vaccine and 3,790 who received placebo (Tables 7--9)
(111).
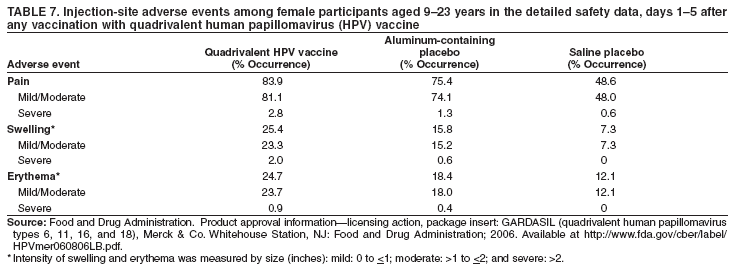
Local Adverse Events
In the study population with detailed safety data, a larger proportion of persons reported injection-site adverse events in
the group that received quadrivalent HPV vaccine compared with aluminum-containing or saline placebo groups
(Table 7). Pain was the most common injection site adverse event, reported by 83.9% of vaccinees, 75.4% of those who received
aluminum-containing placebo, and 48.6% of those who received saline placebo. Swelling and erythema were the next most
common reactions in the vaccine and placebo groups. The majority of injection-site adverse experiences reported among recipients
of quadrivalent HPV vaccine were mild to moderate in intensity; only 2.8%, 2.0%, and 0.9% of vaccinees reported severe
pain, swelling, or erythema, respectively.
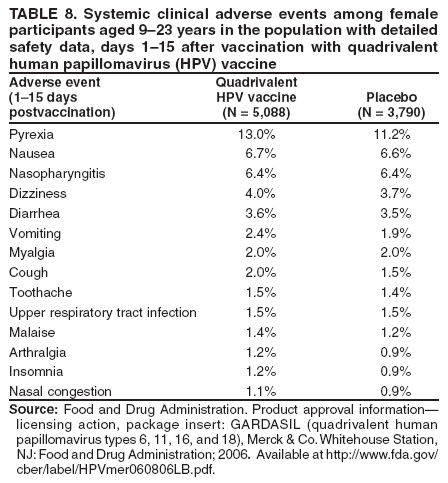
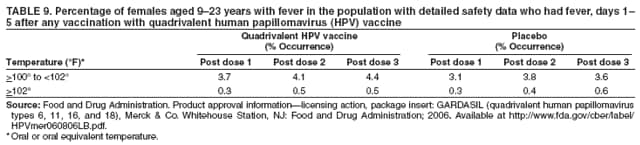
Systemic Adverse Events
Systemic clinical adverse events were reported by a similar proportion of vaccine and placebo recipients in the
population with detailed safety data (Table 8). In both quadrivalent HPV vaccine and placebo groups, more persons reported a
systemic clinical adverse experience in the 15 days after dose 1 compared with after dose 2 and after dose 3. For the majority
of persons, the maximum intensity rating of systemic clinical adverse events was mild or moderate. Overall, 4.0%--4.9%
of females who received quadrivalent HPV vaccine reported a temperature of
>100°F (>38°C) after dose one, two, or
three (Table 9).
Serious Adverse Events in All Safety Studies
Vaccine-related serious adverse events occurred in <0.1% of persons. The proportions of persons reporting a serious
adverse event were similar in the vaccine and placebo groups, as were the types of serious adverse events reported. Seven persons
had events that were determined to be possibly, probably, or definitely related to the vaccine or placebo. Five events
occurred among quadrivalent HPV vaccine recipients and two among placebo recipients. The five in the quadrivalent HPV
vaccine group included bronchospasm, gastroenteritis, headache/hypertension, vaginal hemorrhage, and injection site
pain/movement impairment.
In the overall safety evaluation, 10 persons in the group that received quadrivalent HPV vaccine and seven persons in
the placebo group died during the course of the trials. None of the deaths was considered to be vaccine related. Two deaths in
the vaccine group and one death in the placebo group occurred within 15 days following vaccination. Seven deaths
were attributed to motor-vehicle accidents (four in vaccine group and three in placebo group), three were caused by
intentional overdose (nonstudy medications) or suicide (one in vaccine group and two in placebo group), two were attributed
to pulmonary embolus or deep venous thrombosis (one each in vaccine and placebo group), two were attributed to sepsis,
one case each attributed to cancer and arrhythmia (in vaccine group), and one case caused by asphyxia (placebo group).
New Medical History
Information was collected on new medical conditions that occurred in up to 4 years of follow-up. Overall, nine
(0.08%) participants in the vaccine group and three (0.03%) participants in the placebo group had conditions potentially indicative
of autoimmune disorders, including various arthritis diagnoses (nine in vaccine group and two in placebo group) and
systemic lupus erythematosis (none in vaccine group and one in placebo group)
(111). No statistically significant differences
exist between vaccine and placebo recipients for the incidence of these conditions.
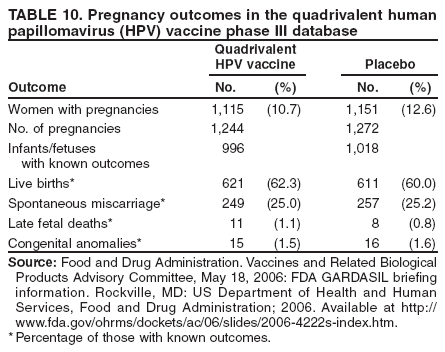
Vaccination During Pregnancy
The quadrivalent clinical trial protocols excluded women who were pregnant. Human beta gonadotropin testing
was conducted before administration of each vaccine dose, and if women were found to be pregnant, vaccination was
delayed until completion of pregnancy. Nevertheless, among clinical trial participants, 1,244 pregnancies occurred in the
vaccine group and 1,272 occurred in the placebo group (Table 10)
(111). Among those with known outcomes (996 and 1,018),
the percentage with spontaneous loss was similar in both groups (25%). A total of 15 and 16 congenital abnormalities
occurred in the vaccine and placebo groups, respectively, including five in the vaccine group and none in the placebo group
among infants born to women who received vaccine or placebo within 30 days of estimated onset of pregnancy. The five
congenital abnormalities were determined by an expert panel to be unrelated (one pyloric stenosis with ankyloglossia, one
congenital hydronephrosis, one congenital megacolon, one club foot, and one hip dysplasia). Rates of congenital abnormalities in
the study were consistent with those in surveillance registries. Quadrivalent HPV vaccine has been classified as Category B on
the basis of animal studies in rats showing no evidence of impaired fertility or harm to the
fetus.
Vaccination During Lactation
In the clinical trials, 995 women in the evaluated population (500 and 495 persons in the group that received
quadrivalent HPV vaccine or placebo, respectively) were breast feeding during the vaccination period. A total of 17 (3.4%) and
nine (1.8%) infants of women who breastfed who received quadrivalent HPV vaccine or placebo, respectively, experienced
a serious adverse event. Of the 23 experiences among the 17 infants of women who received vaccine, 12 were
respiratory infections, five were gastroenteritis or diarrhea, and the remaining included various other single events. None was
considered vaccine related.
Impact of Vaccination and Cost Effectiveness
Economic Burden of HPV
The prevention and treatment of anogenital warts and cervical HPV-related disease imposes an estimated burden of
$4 billion or more (2004 dollars) in direct costs in the United States each year
(70,71,115). Of this, approximately $200
million is attributable to the management of genital warts; approximately $300--$400 million to invasive cervical cancer; and
the remainder to routine cervical cancer screening, the follow-up of abnormal Pap tests, and pre-invasive cervical cancer
(71,115).The estimated economic burden associated with HPV would be more substantial if the cost of other HPV-related
diseases (e.g., vaginal and anal cancer and RRP) were included.
Expected Impact of Vaccination
Various different models have been developed to evaluate the impact of HPV vaccine
(116). Markov models have suggested that vaccination of an entire cohort of females aged 12 years could reduce the lifetime risk for cervical cancer by
20%--66% (117,118) in that cohort, depending on the efficacy of the vaccine and the duration of vaccine protection. Models also
project
decreases in Pap test abnormalities and cervical cancer precursor lesions as a result of vaccination. For example, incidence
of low-grade Pap test abnormalities would decrease by 21% over the life of a vaccinated cohort of females aged 12 years
(117). Models that incorporate HPV transmission dynamics suggest an even greater potential impact of HPV vaccination
on cervical cancer and cervical cancer precursors
(119--121). Decreases in cervical cancer incidence and precursor lesions
would occur more quickly with catch-up vaccination according to models that evaluated catch-up for females aged 12--24
years (121,122).
Cost Effectiveness of HPV Vaccine
Since 2003, four studies have estimated the potential cost effectiveness of HPV vaccination in the context of cervical
cancer screening practices in the United States
(117--119,121). Two of these studies applied Markov models to estimate the cost
per quality-adjusted life year (QALY), focusing on the costs and impact of HPV vaccination for a given cohort,
without considering the effect of vaccination on HPV transmission in the population (herd immunity). The other studies
applied dynamic transmission models to incorporate the benefits of herd immunity in estimating the cost effectiveness of
HPV vaccination.
The two studies based on Markov models of the natural history of HPV infection examined the cost effectiveness
of vaccinating females aged 12 years. One study assumed 100% vaccine coverage, 90% vaccine efficacy against HPV
16/18, lifetime duration of protection, and a cost of $377 per vaccine series
(118). Under these assumptions, an estimated
58% reduction was achieved in the lifetime risk for cervical cancer for the vaccinated cohort at a cost of $24,300 (2002 dollars)
per QALY compared with no vaccination. A second study assumed 70% vaccine coverage, 75% efficacy against all
high-risk HPV types, 10 years duration of protection plus 10 additional years of protection with a booster, and a cost of $300 per vaccine
series plus $100 per booster (117). Under these assumptions, an estimated 20% reduction in cervical cancer incidence was achieved
in the vaccinated cohort at a cost of $22,800 per QALY (2001 dollars) compared with no
vaccination.
The two cost effectiveness analyses based on dynamic transmission models examined the cost effectiveness of
vaccinating females. One study assumed vaccination at age 12 years with 70% vaccine coverage. The vaccine cost $300 per series
plus $100 per booster and targeted HPV 16/18 with 90% efficacy and 10-year duration of protection plus 10 additional
years with a booster (119). Under these assumptions, the lifetime risk for cervical cancer among vaccinated females would
be reduced by 62% at a cost per QALY of $14,600 (2001 dollars) compared with no vaccination. A second study
assumed vaccination at or before age 12 years with 70% vaccine coverage
(121). The vaccine cost $360 per series and targeted
HPV types 6, 11, 16, and 18, with 90% efficacy against infection and 100% efficacy against HPV-related diseases attributable
to these HPV types, with lifelong duration of protection. Under these assumptions, over the long term, a reduction
of approximately 75% was achieved in the cervical cancer incidence rate attributable to HPV 16 and 18 at a cost of $3,000
per QALY in 2005 dollars compared with no vaccination. This model also suggested that a catch-up program for females
aged 12--24 years would cost $4,700 per QALY compared with vaccination of females aged 12 years only.
The cost per QALY gained by routine vaccination of females at age 12 years in the published studies ranged from $3,000
to $24,300. The results summarized are calculated using base-case scenarios, which vary across studies. In the
sensitivity analyses, when base-case assumptions were modified, the estimated cost effectiveness ratios changed substantially.
For example, factors such as duration of vaccine-induced protection, duration of natural immunity, frequency of cervical
cancer screening, vaccine coverage, and vaccine cost impacted the estimated cost effectiveness of HPV vaccination
(116--119,121,123).
Summary of Rationale for Quadrivalent HPV Vaccine Recommendations
The availability of a quadrivalent HPV vaccine offers an opportunity to decrease the burden of HPV infection and
its sequelae, including cervical cancer precursors, cervical cancer, other anogenital cancers, and genital warts in the United
States. Quadrivalent HPV vaccine is licensed for use among females aged 9--26 years. In this age group, clinical trials indicate
that the vaccine is safe and immunogenic. Trials among females aged 16--26 years indicated the vaccine to be effective
against HPV types 6-, 11-, 16-, and 18-related cervical,
vaginal and vulvar cancer precursor and dysplastic lesions, and genital
warts. HPV 16 and 18 are the cause of approximately 70% of cervical cancers; HPV 6 and 11 are the cause of approximately
90% of genital warts. Because HPV is sexually transmitted and often acquired soon after onset of sexual activity,
vaccination
should ideally occur before sexual debut. The recommended age for vaccination is 11--12 years; vaccine can be administered
to females as young as age 9 years. At the beginning of a vaccination program, females aged >12 years will exist who did not
have the opportunity to receive vaccine at age 11--12 years. Catch-up vaccination is recommended for females aged 13--26 years
who have not yet been vaccinated.
The recommendation for routine vaccination of females aged 11--12 years is based on several considerations,
including studies suggesting that quadrivalent HPV vaccine among adolescents will be safe and effective; high antibody titers
achieved after vaccination at age 11--12 years; data on HPV epidemiology and age of sexual debut in the United States; and the
high probability of HPV acquisition within several years of sexual debut. Ideally, HPV vaccine should be administered
before sexual debut, and duration of protection should extend for many years, providing protection when exposure through
sexual activity might occur. The vaccine has been demonstrated to provide protection for at least 5 years without evidence of
waning protection. Long-term follow-up studies are underway to determine duration of protection. The recommendation
also considered cost effectiveness evaluations and the established young adolescent health-care visit at age 11--12
years recommended by several professional organizations, when other vaccines are also recommended.
Although routine vaccination is recommended at age 11--12 years, the majority of females aged 13--26 years also
can benefit from vaccination. Females not yet sexually active can be expected to receive the full benefit of vaccination.
Although sexually active females in this age group might have been infected with one or more vaccine HPV types,
type-specific prevalence studies in the United States suggest that a small percentage of sexually active females have been infected with
all four of the HPV vaccine types. These data, available from North American females aged 16--24 years who participated in
the quadrivalent vaccine trials, are from women who were more likely to have ever had sex than similar aged females in
the general U.S. population. Among those sexually active females, the median number of lifetime sex partners (two) was
similar in trial participants and females in the general
U.S. population. The vaccine does not appear to protect against
persistent infection, cervical cancer precursor lesions, or genital warts caused by an HPV type that females are infected with at the
time of vaccination. However, females already infected with one or more vaccine HPV types before vaccination would be
protected against disease caused by the other vaccine HPV types. Therefore, although overall vaccine effectiveness would be lower
when administered to a population of females who are sexually active, and would decrease with older age and likelihood of
HPV exposure with increasing number of sex partners, the majority of females in this age group will derive at least partial
benefit from vaccination.
Recommendations for Use of HPV Vaccine
Recommendations for Routine Use and Catch-Up
Routine Vaccination of Females Aged 11--12 Years
ACIP recommends routine vaccination of females aged 11--12 years with 3 doses of quadrivalent HPV vaccine.
The vaccination series can be started as young as age 9 years.
Catch-Up Vaccination of Females Aged 13--26 Years
Vaccination also is recommended for females aged 13--26 years who have not been previously vaccinated or who have
not completed the full series. Ideally, vaccine should be administered before potential exposure to HPV through sexual
contact; however, females who might have already been exposed to HPV should be vaccinated. Sexually active females who have
not been infected with any of the HPV vaccine types would receive full benefit from vaccination. Vaccination would provide
less benefit to females if they have already been infected with one or more of the four vaccine HPV types. However, it is
not possible for a clinician to assess the extent to which sexually active persons would benefit from vaccination, and the risk
for HPV infection might continue as long as persons are sexually active. Pap testing and screening for HPV DNA or
HPV antibody are not needed before vaccination at any age.
Dosage and Administration
The vaccine should be shaken well before administration. The dose of quadrivalent HPV vaccine is 0.5 mL,
administered intramuscularly (IM), preferably in the deltoid muscle.
Recommended Schedule
Quadrivalent HPV vaccine is administered in a 3-dose schedule. The second and third doses should be administered 2
and 6 months after the first dose.
Minimum Dosing Intervalsand Management of Persons Who Were Incorrectly Vaccinated
The minimum interval between the first and second doses of vaccine is 4 weeks. The minimum recommended
interval between the second and third doses of vaccine is 12 weeks. Inadequate doses of quadrivalent HPV vaccine or vaccine
doses received after a shorter-than-recommended dosing interval should be readministered.
Interrupted Vaccine Schedules
If the quadrivalent HPV vaccine schedule is interrupted, the vaccine series does not need to be restarted. If the series
is interrupted after the first dose, the second dose should be administered as soon as possible, and the second and third
doses should be separated by an interval of at least 12 weeks. If only the third dose is delayed, it should be administered as soon
as possible.
Simultaneous Administration with Other Vaccines
Although no data exist on administration of quadrivalent HPV vaccine with vaccines other than hepatitis B
vaccine, quadrivalent HPV vaccine is not a live vaccine and has no components that adversely impact safety or efficacy of
other vaccinations. Quadrivalent HPV vaccine can be administered at the same visit as other age appropriate vaccines, such as
the Tdap and quadrivalent meningococcal conjugate (MCV4) vaccines. Administering all indicated vaccines together at a
single visit increases the likelihood that adolescents and young adults will receive each of the vaccines on schedule. Each
vaccine should be administered using a separate syringe at a different anatomic site.
Cervical Cancer Screening Among Vaccinated Females
Cervical cancer screening recommendations have not changed for females who receive HPV vaccine (Table 2). HPV
types in the vaccine are responsible for approximately 70% of cervical cancers; females who are vaccinated could subsequently
be infected with a carcinogenic HPV type for which the quadrivalent vaccine does not provide protection. Furthermore,
those who were sexually active before vaccination could have been infected with a vaccine type HPV before vaccination.
Health-care providers administering quadrivalent HPV vaccine should educate women about the importance of cervical
cancer screening.
Groups for Which Vaccine is Not Licensed
Vaccination of Females Aged <9 Years and >26 Years
Quadrivalent HPV vaccine is not licensed for use among females aged <9 years or those aged >26 years. Studies are
ongoing among females aged >26 years. No studies are under way among children aged <9 years.
Vaccination of Males
Quadrivalent HPV vaccine is not licensed for use among males. Although data on immunogenicity and safety are
available for males aged 9--15 years, no data exist on efficacy in males at any age. Efficacy studies in males are under way.
Special Situations Among Females Aged 9--26 Years
Equivocal or Abnormal Pap Test or Known HPV Infection
Females who have an equivocal or abnormal Pap test could be infected with any of approximately 40 high-risk or
low-risk genital HPV types. Such females are unlikely to be infected with all four HPV vaccine types, and they might not be
infected with any HPV vaccine type. Vaccination would provide protection against infection with HPV vaccine types not
already acquired. With increasing severity of Pap test findings, the likelihood of infection with HPV 16 or 18 increases and
the benefit of vaccination would decrease. Women should be advised that results from clinical trials do not indicate the
vaccine will have any therapeutic effect on existing HPV infection or cervical lesions.
Females who have a positive HC2 High-Risk test conducted in conjunction with a Pap test could have infection with
any of 13 high-risk types. This assay does not identify specific HPV types, and testing for specific HPV types is not
conducted routinely in clinical practice. Women with a positive HC2 High-Risk test might not have been infected with any of the
four HPV vaccine types. Vaccination would provide protection against infection with HPV vaccine types not already
acquired. However, women should be advised that results from clinical trials do not indicate the vaccine will have any therapeutic
effect on existing HPV infection or cervical lesions.
Genital Warts
A history of genital warts or clinically evident genital warts indicates infection with HPV, most often type 6 or
11. However, these females might not have infection with both HPV 6 and 11 or infection with HPV 16 or 18.
Vaccination would provide protection against infection with HPV vaccine types not already acquired. However, females should be
advised that results from clinical trials do not indicate the vaccine will have any therapeutic effect on existing HPV infection
or genital warts.
Lactating Women
Lactating women can receive HPV vaccine.
Immunocompromised Persons
Because quadrivalent HPV vaccine is a noninfectious vaccine, it can be administered to females who are
immunosuppressed as a result of disease or medications. However, the immune response and vaccine efficacy might be less than that in
persons who are immunocompetent.
Vaccination During Pregnancy
Quadrivalent HPV vaccine is not recommended for use in pregnancy. The vaccine has not been causally associated
with adverse outcomes of pregnancy or adverse events in the developing fetus. However, data on vaccination during pregnancy
are limited. Until additional information is available, initiation of the vaccine series should be delayed until after completion
of the pregnancy. If a woman is found to be pregnant after initiating the vaccination series, the remainder of the 3-dose
regimen should be delayed until after completion of the pregnancy. If a vaccine dose has been administered during pregnancy,
no intervention is needed. A vaccine in pregnancy registry has been established; patients and health-care providers should
report any exposure to quadrivalent HPV vaccine during pregnancy (telephone: 800-986-8999).
Precautions and Contraindications
Acute Illnesses
Quadrivalent HPV vaccine can be administered to persons with minor acute illnesses (e.g., diarrhea or mild
upper respiratory tract infections with or without fever). Vaccination of persons with moderate or severe acute illnesses should
be deferred until after the patient improves
(124).
Hypersensitivity or Allergy to Vaccine Components
Quadrivalent HPV vaccine is contraindicated for persons with a history of immediate hypersensitivity to yeast or to
any vaccine component. Data from passive surveillance in Vaccine Adverse Event Reporting System (VAERS) indicates
that recombinent yeast derived vaccines pose a minimal risk for anaphylaxic reactions in persons with a history of allergic
reactions to Saccharomyces cerevisiae (baker's yeast)
(125).
Preventing Syncope After Vaccination
Syncope (i.e., vasovagal or vasodepressor reaction) can occur after vaccination, most commonly among adolescents
and young adults (124). Among reports to VAERS for any vaccine that were coded as syncope during 1990--2004, a total of
35% of these episodes were reported among persons aged 10--18 years. Through January 2007, the second most common report
to VAERS following receipt of HPV vaccine was syncope (CDC, unpublished data, 2007). Vaccine providers should
consider observing patients for 15 minutes after they receive HPV vaccine.
Reporting of Adverse Events After Vaccination
As with any newly licensed vaccine, surveillance for rare adverse events associated with administration of quadrivalent
HPV vaccine is important for assessing its safety in widespread use. All clinically significant adverse events should be reported
to VAERS at http://vaers.hhs.gov, even if causal relation to vaccination is not certain. VAERS reporting forms and
information are available electronically at http://www.vaers.hhs.gov or by telephone (800-822-7967). Web-based reporting is available
and providers are encouraged to report electronically at
https://secure.vaers.org/VaersDataEntryintro.htm to promote
better timeliness and quality of safety data.
Safety surveillance for adolescent quadrivalent HPV vaccine, Tdap, MCV4, and other vaccines is being conducted on
an ongoing basis in cooperation with FDA. A vaccine in pregnancy registry has been established by Merck and Co., Inc.;
patients and health-care providers should report any exposure to quadrivalent HPV vaccine during pregnancy (telephone:
800-986-8999).
Areas for Research and Program Activity Related to HPV Vaccine
With licensure and introduction of quadrivalent HPV vaccine for females, monitoring impact of vaccination and
vaccine safety will be needed. Research in several areas is ongoing, and research in other areas is needed.
Duration of Protection from the Quadrivalent Vaccine:
Long-term data on duration of antibody response and
clinical protection will be obtained through studies conducted in the Nordic countries through the Nordic cancer registries
and through other studies in the United States
(111). Follow up of vaccine trial participants aged 9--15 years will continue for
up to 10 years after dose 3. This will include evaluation of antibody titers and, in participants who reach their 16th
birthday, evaluation of vaccine effectiveness.
Surveillance for HPV-Related Outcomes: Although it will take years to realize the impact of vaccination on
cervical cancer, decreases in cervical cancer precursors and genital warts should be realized sooner. Studies are planned to
monitor these lesions and other HPV-related outcomes in the United States.
Virologic Surveillance: Prevalence and incidence of HPV types in the vaccine are expected to decrease as a result
of vaccination. Studies are planned to monitor HPV types in various populations and specimens.
Safety of Vaccination: Postlicensure studies to evaluate general safety and pregnancy outcomes will be conducted by
the manufacturer and independently by CDC. Monitoring will be accomplished through VAERS and CDC's Vaccine
Safety Datalink, which will include surveillance of cohorts of recently vaccinated females and evaluation of outcomes of
pregnancy among those pregnant at the time of vaccination. The manufacturer will be monitoring long-term safety as part of the
Nordic Cancer Registry Program (111).
Simultaneous Vaccination: Safety and immunogenicity studies of simultaneous administration of quadrivalent
HPV vaccine with Tdap and MCV4 are ongoing.
Efficacy of HPV Vaccine in Men: Studies are needed to define the efficacy of HPV vaccination in preventing genital
warts and anogenital intraepithelial neoplasia in men. Studies of the effectiveness of HPV vaccination of men in
preventing transmission to both female and male sex partners are also needed.
Cervical Cancer Screening: Recommendations for cervical cancer screening guidelines have not changed. Evaluation
of the impact of HPV vaccination on cervical cancer screening provider practices and women's screening behavior is needed
as well as further economic analyses.
Vaccine Delivery and Implementation: Administration of 3 doses of vaccine in adolescents will be
challenging. Programmatic research is needed to determine optimal strategies to reach this age group.
Vaccines for Children Program
The Vaccines for Children (VFC) program supplies vaccines to all states, territories, and the District of Columbia for
use by participating providers. These vaccines are to be administered to eligible children without cost to the patients or
the provider. All routine childhood vaccines recommended by ACIP are available through this program. The program
saves patients and providers out-of-pocket expenses for vaccine purchases and provides cost savings to states through CDC
vaccine contracts. The program results in lower vaccine prices and ensures that all states pay the same contract prices.
Detailed information about the VFC program is available at
http://www.cdc.gov/nip/vfc/default.htm.
The following persons provided technical expertise: William L. Atkinson, MD, Melinda Wharton, MD, John Iskander, MD, CDC,
and Nancy Miller, MD, FDA. Natalya Revzina, MD, also assisted in the production of this report.
References
Weinstock H, Berman S, Cates W Jr. Sexually transmitted diseases among American youth: incidence and prevalence estimates, 2000. Perspect
Sex Reprod Health 2004;36:6--10.
Koutsky LA, Kiviat NB. Genital human papillomavirus. In: Holmes KK, Sparling PF, Mardh PA, et al, eds. Sexually transmitted diseases.
New York, NY: McGraw-Hill; 1999:347--59.
World Health Organization. IARC monograph on the evaluation of carcinogenic risks to humans: human papillomaviruses. 1995. Lyons,
France, IARC; 2000.
Munoz N, Bosch FX, de Sanjose S, et al. Epidemiologic classification of human papillomavirus types associated with cervical cancer. N Engl J
Med 2003;348:518--27.
Walboomers JM, Jacobs MV, Manos MM, et al. Human papillomavirus is a necessary cause of invasive cervical cancer worldwide. J
Pathol 1999;189:12--9.
Bosch FX, de SS. Human papillomavirus and cervical cancer---burden and assessment of causality. J Natl Cancer Inst Monogr 2003;31:3--13.
World Health Organization. HPV IARC monograph summary. Lancet Oncology 2005;6:204.
Parkin DM. The global health burden of infection-associated cancers in the year 2002. Int J Cancer 2006;118:3030--44.
Daling JR, Weiss NS, Klopfenstein LL, Cochran LE, Chow WH, Daifuku R. Correlates of homosexual behavior and the incidence of anal
cancer. JAMA 1982;247:1988--90.
Daling JR, Weiss NS, Hislop TG, et al. Sexual practices, sexually transmitted diseases, and the incidence of anal cancer. N Engl J
Med 1987;317:973--7.
Holly EA, Whittemore AS, Aston DA, Ahn DK, Nickoloff BJ, Kristiansen JJ. Anal cancer incidence: genital warts, anal fissure or fistula,
hemorrhoids, and smoking. J Natl Cancer Inst 1989;81:1726--31.
Koblin BA, Hessol NA, Zauber AG, et al. Increased incidence of cancer among homosexual men, New York City and San Francisco,
1978--1990. Am J Epidemiol 1996;144:916--23.
Ries L, Kosery C, Hankey B, MillerB, Clegg L, Edwards B. SEER Cancer Statistics Review 1973--1996. Bethesda, MD: National Cancer
Institute; 1999.
Kreimer AR, Clifford GM, Boyle P, Franceschi S. Human papillomavirus types in head and neck squamous cell carcinomas worldwide:
a systematic review. Cancer Epidemiol Biomarkers Prev 2005;14:467--75.
de Villiers EM, Fauquet C, Broker TR, Bernard HU, zur HH. Classification of papillomaviruses. Virology 2004;324:17--27.
Duensing S, Munger K. Mechanisms of genomic instability in human cancer: insights from studies with human papillomavirus oncoproteins. Int
J Cancer 2004;109:157--62.
Stanley M. Immune responses to human papillomavirus. Vaccine 2006;24:S16--S22.
Carter JJ, Koutsky LA, Hughes JP, et al. Comparison of human papillomavirus types 16, 18, and 6 capsid antibody responses following
incident infection. J Infect Dis 2000;181:1911--9.
Ho GY, Studentsov YY, Bierman R, Burk RD. Natural history of human papillomavirus type 16 virus-like particle antibodies in young
women. Cancer Epidemiol Biomarkers Prev 2004;13:110--6.
Carter JJ, Koutsky LA, Wipf GC, et al. The natural history of human papillomavirus type 16 capsid antibodies among a cohort of
university women. J Infect Dis 1996;174:927--36.
Kirnbauer R, Booy F, Cheng N, Lowy DR, Schiller JT. Papillomavirus L1 major capsid protein self-assembles into virus-like particles that are
highly immunogenic. Proc Natl Acad Sci U S A 1992;89:12180--4.
Pagliusi SR, Dillner J, Pawlita M, Quint WG, Wheeler CM, Ferguson M. International standard reagents for harmonization of HPV serology
and DNA assays-an update. Vaccine 2006;24:S193--S200.
Opalka D, Lachman CE, MacMullen SA, et al. Simultaneous quantitation of antibodies to neutralizing epitopes on virus-like particles for
human papillomavirus types 6, 11, 16, and 18 by a multiplexed luminex assay. Clin Diagn Lab Immunol 2003;10:108--15.
Dias D, Van Doren J, Schlottmann S, et al. Optimization and validation of a multiplexed luminex assay to quantify antibodies to
neutralizing epitopes on human papillomaviruses 6, 11, 16, and 18. Clin Diagn Lab Immunol 2005;12:959--69.
Winer RL, Lee SK, Hughes JP, Adam DE, Kiviat NB, Koutsky LA. Genital human papillomavirus infection: incidence and risk factors in a
cohort of female university students. Am J Epidemiol 2003;157:218--26.
Ho GY, Bierman R, Beardsley L, Chang CJ, Burk RD. Natural history of cervicovaginal papillomavirus infection in young women. N Engl J
Med 1998;338:423--8.
Moscicki AB, Hills N, Shiboski S, et al. Risks for incident human papillomavirus infection and low-grade squamous intraepithelial
lesion development in young females. JAMA 2001;285:2995--3002.
Koutsky L. Epidemiology of genital human papillomavirus infection. Am J Med 1997;102:3--8.
Karlsson R, Jonsson M, Edlund K, et al. Lifetime number of partners as the only independent risk factor for human papillomavirus infection:
a population-based study. Sex Transm Dis 1995;22:119--27.
Ley C, Bauer HM, Reingold A, et al. Determinants of genital human papillomavirus infection in young women. J Natl Cancer Inst
1991;83:997--1003.
Peyton CL, Gravitt PE, Hunt WC, et al. Determinants of genital human papillomavirus detection in a US population. J Infect
Dis 2001;183:1554--64.
Manhart LE, Holmes KK, Koutsky LA, et al. Human papillomavirus infection among sexually active young women in the United
States: implications for developing a vaccination strategy. Sex Transm Dis 2006;33:502--8.
Trottier H, Franco EL. The epidemiology of genital human papillomavirus infection. Vaccine 2006;24:1--15.
Fairley CK, Gay NJ, Forbes A, Abramson M, Garland SM. Hand-genital transmission of genital warts? An analysis of prevalence data.
Epidemiol Infect 1995;115:169--76.
Marrazzo JM, Stine K, Koutsky LA. Genital human papillomavirus infection in women who have sex with women: a review. Am J Obstet
Gynecol 2000;183:770--4.
Sun XW, Kuhn L, Ellerbrock TV, Chiasson MA, Bush TJ, Wright TC. Human papillomavirus infection in women infected with the
human immunodeficiency virus. N Engl J Med 1997;337:1343--9.
Fairley CK. Prevalence of HPV DNA in cervical specimens in women with renal transplants: a comparison with dialysis-dependent patients
and patients with renal impairment. Nephrology, Dialysis, Transplantation 1994;9:416--20.
Watts DH, Koutsky LA, Holmes KK, et al. Low risk of perinatal transmission of human papillomavirus: results from a prospective cohort
study. Am J Obstet Gynecol 1998;178:365--73.
af Geijersstam V, Eklund C, Wang Z, et al. A survey of seroprevalence of human papillomavirus types 16, 18 and 33 among children. Int J
Cancer 1999;80:489--93.
Abma JC, Martinez GM, Mosher WD, Dawson BS. Teenagers in the United States: sexual activity, contraceptive use, and childbearing,
2002. Vital Health Stat 2004;24:1--48.
Mosher WD, Chandra A, Jones J. Sexual behavior and selected health measures: men and women 15--44 years of age, United States, 2002.
Adv Data 2006;362:1--55.
Franco EL, Villa LL, Sobrinho JP, et al. Epidemiology of acquisition and clearance of cervical human papillomavirus infection in women from a
high-risk area for cervical cancer. J Infect Dis 1999;180:1415--23.
Molano M, Van den BA, Plummer M, et al. Determinants of clearance of human papillomavirus infections in Colombian women with
normal cytology: a population-based, 5-year follow-up study. Am J Epidemiol 2003;158:486--94.
Moscicki AB, Shiboski S, Broering J, et al. The natural history of human papillomavirus infection as measured by repeated DNA testing
in adolescent and young women. J Pediatr 1998;132:277--84.
Ho GY, Burk RD, Klein S, et al. Persistent genital human papillomavirus infection as a risk factor for persistent cervical dysplasia. J Natl
Cancer Inst 1995;87:1365--71.
Hildesheim A, Schiffman MH, Gravitt PE, et al. Persistence of type-specific human papillomavirus infection among cytologically normal
women. J Infect Dis 1994;169:235--40.
Schlecht NF, Platt RW, Duarte-Franco E, et al. Human papillomavirus infection and time to progression and regression of cervical
intraepithelial neoplasia. J Natl Cancer Inst 2003;95:1336--43.
Schiffman M, Kjaer SK. Natural history of anogenital human papillomavirus infection and neoplasia. J Natl Cancer Inst Monogr 2003;31:14--9.
Moscicki AB, Schiffman M, Kjaer S, Villa LL. Updating the natural history of HPV and anogenital cancer. Vaccine 2006;24:S42--S51.
Wheeler CM, Hunt WC, Schiffman M, Castle PE. Human papillomavirus genotypes and the cumulative 2-year risk of cervical precancer. J
Infect Dis 2006;194:1291--9.
Castellsague X, Munoz N. Cofactors in human papillomavirus carcinogenesis---role of parity, oral contraceptives, and tobacco smoking. J
Natl Cancer Inst Monogr 2003;31:20--8.
Zelmanowicz AM, Schiffman M, Herrero R, et al. Family history as a co-factor for adenocarcinoma and squamous cell carcinoma of the
uterine cervix: results from two studies conducted in Costa Rica and the United States. Int J Cancer 2005;116:599--605.
Munoz N, Castellsague X, de Gonzalez AB, Gissmann L. HPV in the etiology of human cancer. Vaccine 2006;24:S1--S10.
Myers ER, McCrory DC, Nanda K, Bastian L, Matchar DB. Mathematical model for the natural history of human papillomavirus infection
and cervical carcinogenesis. Am J Epidemiol 2000;151:1158--71.
Revzina NV, Diclemente RJ. Prevalence and incidence of human papillomavirus infection in women in the USA: a systematic review. Int J
STD AIDS 2005;16:528--37.
Burk RD, Kelly P, Feldman J, et al. Declining prevalence of cervicovaginal human papillomavirus infection with age is independent of other
risk factors. Sex Transm Dis 1996;23:333--41.
Wheeler CM, Parmenter CA, Hunt WC, et al. Determinants of genital human papillomavirus infection among cytologically normal
women attending the University of New Mexico student health center. Sex Transm Dis 1993;20:286--9.
Datta DS, Koutsky L, Douglas JM, et al. Sentinel surveillance for human papillomavirus among women in the United States,
2003--2004 [Abstract MO-306 ISSTDR]. Amsterdam; 2005--2006.
Dunne EF, Unger ER, Sternberg M, et al. Prevalence of HPV infection among females in the US; National health and nutrition
examination survey (NHANES), 2003--2004. JAMA 2007;297:813--9.
Stone KM, Karem KL, Sternberg MR, et al. Seroprevalence of human papillomavirus type 16 infection in the United States. J Infect
Dis 2002;186:1396--402.
Baldwin SB, Wallace DR, Papenfuss MR, et al. Human papillomavirus infection in men attending a sexually transmitted disease clinic. J Infect
Dis 2003;187:1064--70.
Hernandez BY, McDuffie K, Goodman MT, et al. Comparison of physician- and self-collected genital specimens for detection of
human papillomavirus in men. J Clin Microbiol 2006;44:513--7.
Weaver BA, Feng Q, Holmes KK, et al. Evaluation of genital sites and sampling techniques for detection of human papillomavirus DNA in men.
J Infect Dis 2004;189:677--85.
Partridge JM, Koutsky LA. Genital human papillomavirus infection in men. Lancet Infect Dis 2006;6:21--31.
Dunne EF, Nielson CM, Stone KM, Markowitz LE, Giuliano AR. Prevalence of HPV infection among men: a systematic review of the literature.
J Infect Dis 2006;194:1044--57.
Ostor AG. Natural history of cervical intraepithelial neoplasia: a critical review. Int J Gynecol Pathol 1993;12:186--92.
Datta DS, Koutsky L, Ratelle S, et al. Type-specific high-risk human papillomavirus prevalence in the US: HPV Sentinel Surveillance
Project, 2003--2005 [Abstract 1084]. Infectious Disease Society of America, Toronto 2006.
Insinga RP, Glass AG, Rush BB. The health care costs of cervical human papillomavirus--related disease. Am J Obstet Gynecol 2004;191:114--20.
Chesson HW, Blandford JM, Gift TL, Tao G, Irwin KL. The estimated direct medical cost of sexually transmitted diseases among American
youth, 2000. Perspect Sex Reprod Health 2004;36:11--9.
Cox JT. Management of women with cervical cytology interpreted as ASC-US or as ASC-H. Clin Obstet Gynecol 2005;48:160--77.
Wright TC Jr., Cox JT, Massad LS, Twiggs LB, Wilkinson EJ. 2001 consensus guidelines for the management of women with cervical
cytological abnormalities. JAMA 2002;287:2120--9.
Saslow D, Runowicz CD, Solomon D, et al. American Cancer Society guideline for the early detection of cervical neoplasia and cancer. CA
Cancer J Clin 2002;52:342--62.
Schiffman M, Brinton L, Devesa S, Fraumeni J. Cervical cancer. In: Schottenfeld D, Fraumeni J, eds. Cancer epidemiology and prevention.
New York, NY: Oxford University Press; 1996:1090--128.
Smith HO, Tiffany MF, Qualls CR, Key CR. The rising incidence of adenocarcinoma relative to squamous cell carcinoma of the uterine cervix
in the United States---a 24-year population-based study. Gynecol Oncol 2000;78:97--105.
Hildesheim A, Berrington de GA. Etiology and prevention of cervical adenocarcinomas. J Natl Cancer Inst 2006;98:292--3.
Saraiya M, Ahmed F, Krishnan S, Richards T, Unger E, Lawson HW. Cervical cancer incidence in a prevaccine era in the United States,
1998--2002. Obstet Gynecol 2007;109:360--70.
US Cancer Statistics Working Group. United States cancer statistics: 2003. Incidence and mortality. Atlanta, GA: US Department of Health
and Human Services, CDC and the National Cancer Institute. 2005. Available at
http://www.cdc.gov/uscs.
Miller B, Kolonel L, Bernstein L, et al. Racial/ethnic patterns of cancer in the United States, 1996. Bethesda, MD: National Cancer
Institute (NIH Pub No. 96-4104).
Lengerich EJ, Tucker TC, Powell RK, et al. Cancer incidence in Kentucky, Pennsylvania, and West Virginia: disparities in Appalachia. J
Rural Health 2005;21:39--47.
Freeman H, Wingrove B. Excess cervical cancer mortality: a marker for low access to health care in poor communities. Rockville, MD:
National Cancer Institue, Center to Reduce Cancer Health Disparities 2005 (NIH Pub. No. 05-5282).
van Seters M, van Beurden M, de Craen AJ. Is the assumed natural history of vulvar intraepithelial neoplasia III based on enough evidence?
A systematic review of 3322 published patients. Gynecol Oncol 2005;97:645--51.
Jones RW, Rowan DM, Stewart AW. Vulvar intraepithelial neoplasia: aspects of the natural history and outcome in 405 women. Obstet
Gynecol 2005;106:1319--26.
Daling JR, Sherman KJ. Cancers of vulva and vagina. In: Schottenfeld D, Fraumeni J, eds. Cancer epidemiology and prevention. New York,
NY: Oxford University Press; 1996:1117--29.
Daling JR, Madeleine MM, Schwartz SM, et al. A population-based study of squamous cell vaginal cancer: HPV and cofactors. Gynecol
Oncol 2002;84:263--70.
Hampl M, Sarajuuri H, Wentzensen N, Bender HG, Kueppers V. Effect of human papillomavirus vaccines on vulvar, vaginal, and
anal intraepithelial lesions and vulvar cancer. Obstet Gynecol 2006;108:1361--8.
Judson PL, Habermann EB, Baxter NN, Durham SB, Virnig BA. Trends in the Incidence of Invasive and In Situ Vulvar Carcinoma.
Obstet Gynecol 2006;107:1018--22.
Johnson LG, Madeleine MM, Newcomer LM, Schwartz SM, Daling JR. Anal cancer incidence and survival: the surveillance, epidemiology, and
end results experience, 1973--2000. Cancer 2004;101:281--8.
Schottenfeld D, Winawer S. Cancers of the large intestine. In: Schottenfeld D, Fraumeni J, eds. Cancer epidemiology and prevention. New
York, NY: Oxford University Press; 1996:813--40.
Greer CE, Wheeler CM, Ladner MB, et al. Human papillomavirus (HPV) type distribution and serological response to HPV type 6
virus-like particles in patients with genital warts. J Clin Microbiol 1995;33:2058--63.
Winer RL, Kiviat NB, Hughes JP, et al. Development and duration of human papillomavirus lesions, after initial infection. J Infect
Dis 2005;191:731--8.
Chuang TY, Perry HO, Kurland LT, Ilstrup DM.
Condyloma acuminatum in Rochester, Minn., 1950--1978. I. Epidemiology and clinical
features. Arch Dermatol 1984;120:469--75.
Insinga RP, Dasbach EJ, Myers ER. The health and economic burden of genital warts in a set of private health plans in the United States.
Clin Infect Dis 2003;36:1397--403.
Reeves WC, Ruparelia SS, Swanson KI, Derkay CS, Marcus A, Unger ER. National registry for juvenile-onset recurrent respiratory
papillomatosis. Arch Otolaryngol Head Neck Surg 2003;129:976--82.
Armstrong LR, Preston EJ, Reichert M, et al. Incidence and prevalence of recurrent respiratory papillomatosis among children in Atlanta
and Seattle. Clin Infect Dis 2000;31:107--9.
Winer RL, Hughes JP, Feng Q, et al. Condom use and the risk of genital human papillomavirus infection in young women. N Engl J
Med 2006;354:2645--54.
Ferenczy A, Franco E. Cervical-cancer screening beyond the year 2000. Lancet Oncol 2001;2:27--32.
US Preventive Services Task Force. Screening for cervical cancer: recommendations and rationale. Available at
http://www.ahrq.gov.
ACOG Practice Bulletin. Clinical management guidelines for obstetrician-gynecologists: cervical cytology screening. Obstet
Gynecol 2003;102:417--27.
ACOG Practice Bulletin. Clinical management guidelines for obstetrician-gynecologists: human papillomavirus. Obstet Gynecol
2005;105:905--18.
Swan J, Breen N, Coates RJ, Rimer BK, Lee NC. Progress in cancer screening practices in the United States: results from the 2000
National Health Interview Survey. Cancer 2003;97:1528--40.
Leyden WA, Manos MM, Geiger AM, et al. Cervical cancer in women with comprehensive health care access: attributable factors in the
screening process. J Natl Cancer Inst 2005;97:675--83.
Stanley M, Lowy DR, Frazer I. Prophylactic vaccines: underlying mechanisms. Vaccine 2006;24:S106--S113.
Koutsky LA, Ault KA, Wheeler CM, et al. A controlled trial of a human papillomavirus type 16 vaccine. N Engl J Med 2002;347:1645--51.
Mao C, Koutsky LA, Ault KA, et al. Efficacy of human papillomavirus-16 vaccine to prevent cervical intraepithelial neoplasia: a
randomized controlled trial. Obstet Gynecol 2006;107:18--27.
Villa LL, Costa RL, Petta CA, et al. Prophylactic quadrivalent human papillomavirus (types 6, 11, 16, and 18) L1 virus-like particle vaccine in
young women: a randomised double-blind placebo-controlled multicentre phase II efficacy trial. Lancet Oncol 2005;6:271--8.
Villa LL, Ault KA, Giuliano AR, et al. Immunologic responses following administration of a vaccine targeting human papillomavirus Types 6,
11, 16, and 18. Vaccine 2006;24:5571--83.
Villa LL, Costa RL, Petta CA, et al. High sustained efficacy of a prophylactic quadrivalent human papillomavirus types 6/11/16/18 L1
virus-like particle vaccine through 5 years of follow-up. Br J Cancer 2006;95:1459--66.
Food and Drug Administration. Product approval information---licensing action [package insert]. Gardasil (quadrivalent human papillomavirus
types 6,11,16,18). Merck & Co., Whitehouse Station, NJ. Available at http://www.fda.gov/cber/label/HPVmer060806LB.pdf.
Ferris D. Efficacy of a quadrivalent HPV (types 6/11/16/18) L1 virus-like particle (VLP) vaccine in women with virologic evidence of
HPV infection: a combined analysis [Abstract S11-2.]. European Research Organization on Genital Infection and Neoplasia, Paris, France.April
23--26, 2006.
Block SL, Nolan T, Sattler C, et al. Comparison of the immunogenicity and reactogenicity of a prophylactic quadrivalent human
papillomavirus (types 6, 11, 16, and 18) L1 virus-like particle vaccine in male and female adolescents and young adult women. Pediatrics 2006;118:2135--45.
Villa LL, Costa RLR, Petta CA, et al. Induction of immune memory following administration of a prophylactic quadrivalent
human papillomavirus (HPV) types 6/11/16/18 L1 virus-like particle vaccine. Int J Infec Dis 2006;10(Suppl 1).
Insinga RP, Dasbach EJ, Elbasha EH. Assessing the annual economic burden of preventing and treating anogenital human
papillomavirus-related disease in the US: analytic framework and review of the literature. Pharmacoeconomics 2005;23:1107--22.
Garnett GP, Kim JJ, French K, Goldie SJ. Modelling the impact of HPV vaccines on cervical cancer and screening programmes.
Vaccine 2006;24:S178--S186.
Sanders GD, Taira AV. Cost-effectiveness of a potential vaccine for human papillomavirus. Emerg Infect Dis 2003;9:37--48.
Goldie SJ, Kohli M, Grima D, et al. Projected clinical benefits and cost-effectiveness of a human papillomavirus 16/18 vaccine. J Natl Cancer
Inst 2004;96:604--15.
Barnabas RV, Laukkanen P, Koskela P, Kontula O, Lehtinen M, Garnett GP. Epidemiology of HPV 16 and cervical cancer in Finland and
the potential impact of vaccination: mathematical modelling analyses. PLoS Med 2006;3:e138.
Elbasha E, Dasbach EJ, Insinga RP. Model for assessing human papillomavirus vaccination. Emerg Infect Dis 2007;13:29--41.
French K, Barnabas RV, Matti L, Kontula O, Killner J, Garnett G. Comparing strategies for introducing HPV vaccination in the United States
and Europe; Finland: modeling the optimal age and sex pattern of vaccination [Abstract PS 10-7]. Presented at the 23rd International
Papillomavirus Conference and Workshop; September 1--7, 2006; Prague, Czech Republic.
Kulasingam SL, Myers ER. Potential health and economic impact of adding a human papillomavirus vaccine to screening programs.
JAMA 2003;290:781--9.
DiMiceli L, Pool V, Kelso JM, Shadomy SV, Iskender J. Vaccination of yeast sensitive individuals: review of safety data in the U.S. vaccine
adverse event reporting system (VAERS). Vaccine 2006;24:703--7.
* The en dash in numeric ranges is used to represent inclusive years, hours, days, ages, dosages, or a sequence of numbered items.
Advisory Committee on Immunization Practices
Membership List, June 24, 2006
Chairman: Jon Abramson, MD, Wake Forest University School of Medicine, Winston-Salem, North Carolina.
Executive Secretary: Larry Pickering, MD, CDC, Atlanta, Georgia.
Members: Ban Mishu Allos, MD, Vanderbilt University School of Medicine, Nashville, Tennessee; Judith Campbell, MD, Baylor College of
Medicine, Houston, Texas; Robert Beck, JD, Consumer Representative, Palmyra, Virginia; Reginald Finger, MD, Focus on the Family, Colorado
Springs, Colorado; Janet Gilsdorf, MD, University of Michigan, Ann Arbor, Michigan; Harry Hull, MD, Minnesota Department of Health, St.
Paul, Minnesota; Tracy Lieu, MD, Harvard Pilgrim Health Care and Harvard Medical School, Boston, Massachusetts; Edgar Marcuse, MD,
Children's Hospital and Regional Medical Center, Seattle, Washington; Dale Morse, MD, New York State Department of Health, Albany, New York; Julia
Morita, MD, Chicago Department of Public Health, Chicago, Illinois; Gregory Poland, MD, Mayo Medical School, Rochester, Minnesota; Patricia
Stinchfield, MSN, Children's Hospitals and Clinics of Minnesota, St. Paul, Minnesota; John J. Treanor, MD, University of Rochester, Rochester, New York;
Robin Womeodu, MD, University Hospital, Memphis, Tennessee.
Ex-Officio Members: James E. Cheek, MD, Indian Health Services, Albuquerque, New Mexico; Wayne Hachey, DO, Department of Defense,
Falls Church, Virginia; Geoffrey S. Evans, MD, Health Resources and Services Administration, Rockville, Maryland; Bruce Gellin, MD, National
Vaccine Program Office, Washington, DC; Linda Murphy, Centers for Medicare and Medicaid Services, Baltimore, Maryland; George T. Curlin, MD,
National Institutes of Health, Bethesda, Maryland; Kristin Lee Nichol, MD, Department of Veterans Affairs, Minneapolis, Minnesota.
Liaison Representatives: American Academy of Family Physicians, Jonathan Temte, MD, Madison, Wisconsin, and Doug Campos-Outcalt,
MD, Phoenix, Arizona; American Academy of Pediatrics, Keith Powell, MD, Akron, Ohio, and Carol Baker, MD, Houston, Texas; America's
Health Insurance Plans, Andrea Gelzer, MD, Hartford, Connecticut; American College Health Association, James C. Turner, MD, Charlottesville,
Virginia; American College of Obstetricians and Gynecologists, Stanley Gall, MD, Louisville, Kentucky; American College of Physicians, Kathleen M.
Neuzil, MD, Seattle, Washington; American Medical Association, Litjen Tan, PhD, Chicago, Illinois; American Pharmacists Association, Stephan L.
Foster, PharmD, Memphis, Tennessee; Association of Teachers of Preventive Medicine, W. Paul McKinney, MD, Louisville, Kentucky; Biotechnology
Industry Organization, Clement Lewin, PhD, Cambridge, Massachusetts; Canadian National Advisory Committee on Immunization, Monica Naus,
MD, Vancouver, British Columbia; Healthcare Infection Control Practices Advisory Committee, Steve Gordon, MD, Cleveland, Ohio; Infectious
Diseases Society of America, Samuel L. Katz, MD, Durham, North Carolina; London Department of Health, David Salisbury, MD, London, United
Kingdom;
National Association of County and City Health Officials, Nancy Bennett, MD, Rochester, New York, and Jeffrey S. Duchin, MD,
Seattle, Washington; National Coalition for Adult Immunization, David A. Neumann, PhD, Alexandria, Virginia; National Foundation for Infectious
Diseases, William Schaffner, MD, Nashville, Tennessee; National Immunization Council and Child Health Program, Romeo S. Rodriquez, Mexico City,
Mexico; National Medical Association, Patricia Whitley-Williams, MD, New Brunswick, New Jersey; National Vaccine Advisory Committee, Gary Freed,
MD, Swiftwater, Pennsylvania, and Peter Paradiso, PhD, Collegeville, Pennsylvinia; Society for Adolescent Medicine, Amy B. Middleman, MD,
Houston, Texas; Pharmaceutical Research and Manufacturers of America, Damian A. Araga, Swiftwater, Pennsylvania.
Human Papillomavirus Vaccine Working Group
Chair: Janet Gilsdorf, MD, Ann Arbor, Michigan.
Members: Robert L. Beck, JD, Palmyra, Virginia; Stuart Berman, MD, Atlanta, Georgia; Joseph Bocchini, MD, Shreveport, Louisiana;
Harrell Chesson, PhD, Atlanta, Georgia; Carolyn Deal, PhD, Bethesda, Maryland; Shelley Deeks, MD, Toronto, Canada; John Douglas, MD,
Atlanta, Georgia; Eileen F. Dunne, MD, Atlanta, Georgia; Dan Fishbein, MD, Atlanta, Georgia; Stanley Gall, MD, Louisville, Kentucky; Bruce Gellin,
MD, Washington, DC; Karen Goldenthal, MD, Rockville, Maryland; Harry Hull, MD, St. Paul, Minnesota; Samuel Katz, MD, Durham, North
Carolina; Katrin Kohn, MD; Herschel W. Lawson, MD, Atlanta, Georgia; Nicole Liddon, PhD, Atlanta, Georgia; Lauri E. Markowitz, MD, Atlanta,
Georgia; Eric Mast, MD, Atlanta, Georgia; Alison Mawle, PhD, Atlanta, Georgia; Amy Middleman, MD, Houston, Texas; Siobhan O'Connor, MD,
Atlanta, Georgia; Mona Saraiya, MD, Atlanta, Georgia; Debbie Saslow, PhD, Atlanta, Georgia; Jane Seward, MBBS, Atlanta, Georgia; Jonathan L. Temte,
MD, Madison, Wisconsin; James Turner, MD, Charlottesville, Virginia; Elizabeth R. Unger, MD, Atlanta, Georgia; Gregory S. Wallace, MD,
Atlanta, Georgia; Robin Womeodu, MD, Memphis, Tennessee; Richard Zimmerman, MD, Pittsburgh, Pennsylvania; and Jane Zucker, MD, New York,
New York.
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services.References to non-CDC sites on the Internet are
provided as a service to MMWR readers and do not constitute or imply
endorsement of these organizations or their programs by CDC or the U.S.
Department of Health and Human Services. CDC is not responsible for the content
of pages found at these sites. URL addresses listed in MMWR were current as of
the date of publication.
All MMWR HTML versions of articles are electronic conversions from ASCII text
into HTML. This conversion may have resulted in character translation or format errors in the HTML version.
Users should not rely on this HTML document, but are referred to the electronic PDF version and/or
the original MMWR paper copy for the official text, figures, and tables.
An original paper copy of this issue can be obtained from the Superintendent of Documents,
U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800.
Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to
mmwrq@cdc.gov.