|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
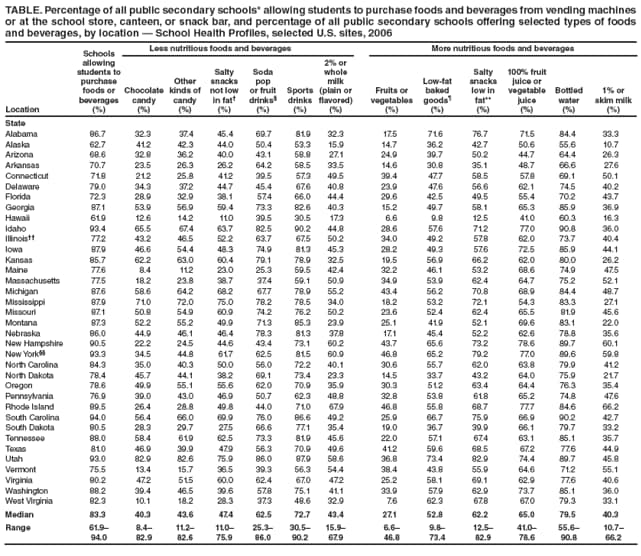
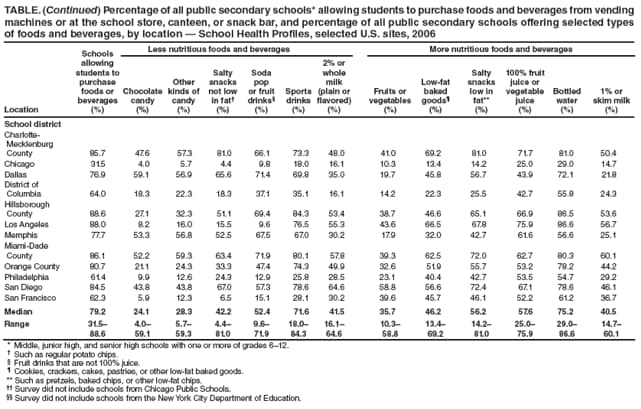
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Competitive Foods and Beverages Available for Purchase in Secondary Schools --- Selected Sites, United States, 2006Schools are in a unique position to help improve youth dietary behaviors and prevent and reduce obesity. In most schools, foods and beverages are made available to students through the U.S. Department of Agriculture (USDA) school meal programs and the sale of competitive foods, which are any foods and beverages sold at a school separately from the USDA school meal programs. Foods and beverages sold through the USDA school meal programs must meet federal nutrition requirements (1). Competitive foods are not subject to any federal nutrition standards unless they are sold inside the food service area during mealtimes (2). A 2007 Institute of Medicine (IOM) report concluded that schools should limit the availability of less nutritious competitive foods or include more nutritious foods and beverages if they make competitive foods available (3). To identify the types of competitive foods and beverages available for purchase from vending machines or at school stores, canteens, or snack bars, CDC analyzed data from the 2006 School Health Profiles for public secondary schools* in 36 states and 12 large urban school districts.† CDC also compared 2004 and 2006 data among 24 states and nine large urban school districts. This report summarizes the results of these analyses, which indicated that, from 2004 to 2006, the median percentage of secondary schools across states allowing students to purchase chocolate candy and salty snacks that are not low in fat decreased; however, in 2006, secondary schools still offered less nutritious foods and beverages that compete with school meals. School and public health officials should work together with families to provide foods and beverages at school that follow the IOM recommendations (3). School Health Profiles surveys have been conducted biennially since 1994 to assess school health programs (4). States and large urban school districts participate in the surveys, selecting either all public secondary schools within their jurisdictions or systematic, equal-probability representative samples of schools.§ At each school, the principal and lead health education teacher are sent questionnaires to be self-administered and returned to the state or local agency conducting the survey. Only principals (or their designees) are asked questions about competitive foods available for purchase by students in their schools.¶ Participation in School Health Profiles is confidential and voluntary. Follow-up telephone calls and written reminders were used to encourage participation. Data from each questionnaire were cleaned and edited by CDC. Those surveys that used a representative sample of schools, had appropriate documentation, and achieved a response rate of 70% or higher were included in the analysis. Data from these surveys were weighted to reflect the likelihood of schools being selected and to adjust for differing patterns of nonresponse. In 2006, 36 states and 13 large urban school districts met the criteria for inclusion in the analysis, and all but one large urban school district granted CDC permission to publish their results. Among states, the number of principals who participated ranged from 68 to 661 (median: 262), and response rates ranged from 70% to 91% (median: 78%); among school districts, the number of principals ranged from 31 to 234 (median: 56), and response rates ranged from 71% to 98% (median: 81%). Comparisons between 2004 and 2006 results include only the 24 states and nine large urban school districts with weighted data available for both years. Data from 2004 were recalculated so that the denominator included all schools in each jurisdiction rather than including only schools allowing students to purchase foods or beverages from vending machines or at the school store, canteen, or snack bar, as was done in a previous report (5). The Wilcoxon rank-sum test was used to test for these differences across states and cities. Differences in distributions were considered statistically significant at p<0.05. The percentage of all secondary schools in which students could purchase snack foods or beverages from vending machines or at the school store, canteen, or snack bar ranged from 61.9% to 94.0% (median: 83.3%) across the 36 states and from 31.5% to 88.6% (median: 79.2%) across the 13 large urban school districts (Table). The types of less nutritious foods available for purchase from vending machines or at the school store, canteen, or snack bar varied. For example, chocolate candy was available for purchase in 8.4% to 82.9% (median: 40.3%) of all secondary schools across states and in 4.0% to 59.1% (median: 24.1%) of all secondary schools across large urban school districts, whereas sports drinks were available in 30.5% to 90.2% (median: 72.7%) of schools across states and in 18.0% to 84.3% (median: 71.6%) of schools across large urban school districts. Students also could purchase more nutritious foods and beverages from vending machines or at the school store, canteen, or snack bar (Table). Fruits or vegetables were available for purchase in 6.6% to 46.8% (median: 27.1%) of all secondary schools across states and in 10.3% to 58.8% (median: 35.7%) of all secondary schools across large urban school districts. Bottled water was available for purchase in 55.6% to 90.8% (median: 79.5%) of schools across states and in 29.0% to 86.6% (median: 75.2%) of schools across large urban school districts. The percentage of all secondary schools that allowed students to purchase candy; snacks not low in fat; soda pop, sports drinks, or fruit drinks that are not 100% juice; or 2% or whole milk during school lunch periods ranged from 3.9% to 81.3% (median: 34.9%) across states and from 15.7% to 72.3% (median: 36.9%) across large urban school districts. From 20.2% to 72.5% (median: 35.0%) of schools across states and from 7.2% to 58.0% (median: 27.6%) of schools across large urban school districts allowed students to purchase these items before classes began in the morning and from 11.9% to 56.6% (median: 29.3%) of schools across states and in 2.9% to 39.1% (median: 12.0%) of schools across large urban school districts allowed students to purchase these items during any school hours when meals were not being served. A comparison of the availability of competitive foods and beverages in schools revealed few changes between 2004 and 2006. Across states, decreases were observed in the median percentage of schools that allowed students to purchase chocolate candy (from 52.3% to 43.1% [p=0.03]) and salty snacks that are not low in fat (from 63.5% to 47.4% [p=0.001]) from vending machines or at the school store, canteen, or snack bar. Across states, no significant changes were detected in the median percentage of schools that allowed students to purchase other kinds of candy, soda pop or fruit drinks that are not 100% juice, sports drinks, fruits or vegetables, low-fat baked goods, low-fat salty snacks, or bottled water from vending machines or at the school store, canteen, or snack bar. Across states, the median percentage of schools that allowed students to purchase candy; snacks that are not low in fat; soda pop, sports drinks, or fruit drinks that are not 100% juice; or 2% or whole milk during school lunch periods decreased from 52.9% to 36.6% (p=0.03). However, no change was observed in the median percentage of schools that allowed students to purchase candy; snacks that are not low in fat; soda pop, sports drinks, or fruit drinks that are not 100% juice; or 2% or whole milk before school or during any school hours when meals are not being served. Across districts, no significant changes were detected in any of the variables tested. Reported by: N Brener, PhD, L Kann, PhD, T O'Toole, PhD, H Wechsler, EdD, Div of Adolescent and School Health; J Kimmons, PhD, Div of Nutrition, Physical Activity, and Obesity, National Center for Chronic Disease Prevention and Health Promotion, CDC. Editorial Note:The findings in this report indicate that, in 2006, in all 36 states and all but one of 12 large urban school districts, 62%--94% of schools allowed students to purchase snack foods or beverages from vending machines at the school or at the school store, canteen, or snack bar. In 28 states and five districts, fruits and vegetables were the least common items available, and in 34 states and 11 districts, bottled water was the most common item available. These results are consistent with previous reports from state and district (5) and national surveys (6). During 2004--2006, the availability during school lunch periods of some less nutritious competitive foods and beverages at schools decreased across states, but availability did not decrease before school or during any school hours when meals are not being served. Competitive food policies are viewed increasingly as an important strategy to address rising rates of childhood obesity. Congress passed legislation in 2004 requiring all school districts to develop a Wellness Policy starting in the 2006--07 school year that includes nutrition guidelines for competitive foods (7). By February 2007, 27 states, 19 of which are included in this report, had adopted competitive food and beverage policies through legislative bills, executive orders, rules, and regulations more restrictive than current USDA federal regulations (3). The findings in this report are subject to at least three limitations. First, these data apply only to public secondary schools and, therefore, do not reflect practices at private schools or elementary schools. Second, these data were self-reported by principals or their designees and were not verified by other sources. Finally, these data were collected during spring and fall 2006 and do not reflect any state, district, or school policies enacted, modified, or discontinued since then. To help improve dietary behavior and reduce obesity among youths, schools should encourage and support greater daily consumption of fruits, vegetables, whole grains, and nonfat or low-fat dairy products by providing better access to these foods and beverages (3). Science-based strategies are available to help states, districts, and schools improve their school nutrition environment. For example, the School Health Index helps schools identify the strengths and weaknesses of their health-promotion policies and programs and develop an action plan to ensure that students have access to appealing and nutritious foods and beverages outside the school meals program (8). In addition, Making It Happen! School Nutrition Success Stories describes the innovative strategies schools and school districts throughout the United States have used to improve the nutritional quality of foods and beverages sold outside of federal meal programs (9). These strategies include establishing nutrition standards for competitive foods, influencing food and beverage contracts, making more healthful foods and beverages available, adopting marketing techniques to promote healthful choices, limiting student access to competitive foods, and using fundraising activities and rewards that support student health. Acknowledgments The findings in this report are based on data collected by state and local School Health Profiles coordinators. References
* Middle, junior high, and senior high schools with one or more of grades 6--12. † States: Alabama, Alaska, Arizona, Arkansas, Connecticut, Delaware, Florida, Georgia, Hawaii, Idaho, Illinois, Iowa, Kansas, Maine, Massachusetts, Michigan, Mississippi, Missouri, Montana, Nebraska, New Hampshire, New York, North Carolina, North Dakota, Oregon, Pennsylvania, Rhode Island, South Carolina, South Dakota, Tennessee, Texas, Utah, Vermont, Virginia, Washington, and West Virginia. School districts: Charlotte-Mecklenburg County, North Carolina; Chicago, Illinois; Dallas, Texas; District of Columbia; Hillsborough County, Florida; Los Angeles, California; Memphis, Tennessee; Miami-Dade County, Florida; Orange County, Florida; Philadelphia, Pennsylvania; San Diego, California; and San Francisco, California. § In the 2006 surveys, statewide samples were representative of all public secondary schools in the state with two exceptions: no schools from the New York City Department of Education were included in the New York state sample, and no schools from the Chicago Public Schools were included in the Illinois sample. ¶ Principals were asked the following questions: 1) "Can students purchase snack foods or beverages from one or more vending machines at the school or at a school store, canteen, or snack bar?" 2) "Can students purchase each snack food or beverage (chocolate candy; other kinds of candy; salty snacks that are not low in fat; soda pop or fruit drinks that are not 100% juice; sports drinks; 2% or whole milk; salty snacks that are low in fat; fruits or vegetables; low-fat cookies, crackers, cakes, pastries, or other low-fat baked goods; 100% fruit juice or vegetable juice; bottled water; or 1% or skim milk) from vending machines or at the school store, canteen, or snack bar?" and 3) "Can students purchase candy; snacks that are not low in fat; soda pop, sports drinks, or fruit drinks that are not 100% juice; or 2% or whole milk during the following times (before classes begin in the morning, during any school hours when meals are not being served, and during school lunch periods)?"
All MMWR HTML versions of articles are electronic conversions from typeset documents. This conversion might result in character translation or format errors in the HTML version. Users are referred to the electronic PDF version (http://www.cdc.gov/mmwr) and/or the original MMWR paper copy for printable versions of official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Date last reviewed: 8/28/2008 |
|||||||||
|