|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
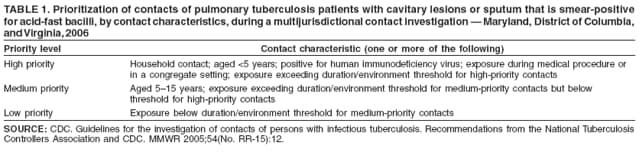
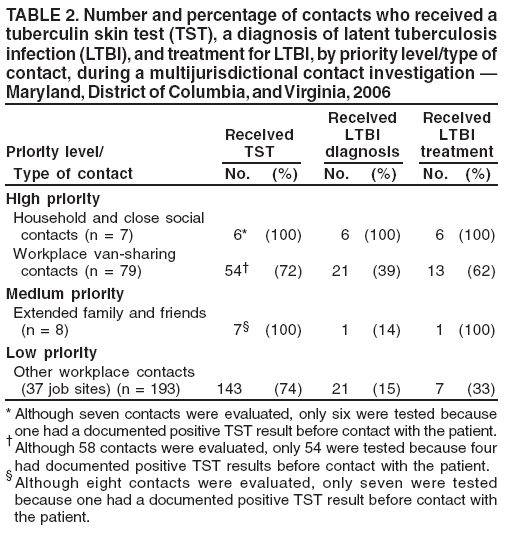
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Workplace-Based Investigation of Contacts of a Patient with Highly Infectious Tuberculosis --- Maryland, District of Columbia, and Virginia, 2006In late April 2006, the Maryland Department of Health and Mental Hygiene (DHMH) was notified by a local health department of a case of pulmonary tuberculosis (TB) in a patient with cavitary lung lesions and numerous acid-fast bacilli (AFB) observed on a sputum smear.* The patient worked for an office furniture installation company at multiple sites in Maryland, the District of Columbia (DC), and Virginia. An investigation was conducted to 1) determine the extent of TB transmission, including identifying and screening the exposed cohort of contacts, and 2) provide treatment, if indicated, to contacts with latent TB infection (LTBI) or TB disease. This report describes the multijurisdictional contact investigation and summarizes its results. The findings underscore the importance of prompt diagnosis of TB, the value of interjurisdictional cooperation during large contact investigations, and the effectiveness of workplace-based methods for rapidly identifying and screening contacts. The patient, a U.S.-born man aged 46 years, visited the emergency department of a local hospital (hospital A) in late April 2006, with longstanding cough, shortness of breath, and weight loss. Because TB was suspected, he was admitted to an airborne-infection isolation room and administered anti-TB therapy. Chest radiography and computed tomography revealed extensive bilateral upper and lower lobe infiltrates with cavitation. A sputum smear was positive for AFB. Hospital A reported the TB case to the local health department. After a 3-day hospital stay, the patient was discharged to home isolation. Follow-up care, including directly observed therapy, was coordinated by the local health department. The DHMH public health laboratory identified the AFB as Mycobacterium tuberculosis using the Amplified MTD® (M. tuberculosis Direct) test (Gen-Probe, San Diego, California). The AFB were confirmed by culture to be M. tuberculosis that were sensitive to all first-line anti-TB drugs. Investigators determined that approximately 1 year before admission to hospital A, in late May 2005, the patient had visited the emergency department of another local hospital (hospital B), complaining of abdominal pain. Chest radiography performed at that time revealed upper lobe infiltrates, and the patient was prescribed a 5-day course of Zithromax® (azithromycin) for community-acquired pneumonia. The patient did not visit a health-care provider subsequently for any symptoms until visiting hospital A in April 2006. For investigation of cases of TB in patients with TB symptoms and sputum that is smear-positive for AFB, the National TB Controllers Association (NTCA) and CDC recommend setting the beginning of the infectious period at 3 months before symptom onset, or at the first positive finding consistent with TB disease, whichever is earlier (1). The patient was a smoker with a chronic cough, which made distinguishing the onset of a TB-associated cough difficult. Because the patient potentially had undocumented TB-associated cough at the time he visited hospital B in May 2005, the start of the infectious period was considered to be 3 months before potential symptom onset (i.e., February 2005). Thus, the infectious period for this investigation was defined as the approximately 15 months from February 1, 2005, through late April 2006. Contacts of the patient were identified and assigned to priority groups based on NTCA/CDC recommendations (1). According to these recommendations, household contacts, contacts with exposure in congregate settings, and contacts whose exposure exceeds duration/environment limits set by state or local health departments should be categorized as high priority† (Table 1). Accordingly, for this patient, household contacts, close social contacts, and close workplace contacts, including coworkers who traveled to job sites in vans with him, were categorized as high priority, whereas other family and social contacts with less duration of exposure and in more open environments were categorized as medium priority.§ Persons whose only contact with the patient was at job sites where the patient worked installing furniture were classified as low priority¶ because they likely had limited or no exposure. High-priority household, social, and workplace contacts of the patient were identified and evaluated within 7 business days of identification of the patient, as recommended by NTCA/CDC (1). Evaluation of contacts for TB includes ascertainment of prior positive tuberculin skin test (TST) status and skin testing of those with no prior positive TST result. Contacts with positive TST results were evaluated further for TB disease with chest radiography. Sputum was collected for AFB smear if any TB symptoms (e.g., cough, fever, weight loss, night sweats, bloody sputum, or malaise) were present. According to NTCA/CDC, sputum also should be collected from contacts whose chest radiographs are suggestive of TB disease (1); however, in this investigation, no contacts had abnormal chest radiographs. All contacts with positive TST results who did not have TB disease, including contacts with prior positive TST results who had no history of treatment for LTBI, were offered treatment for LTBI. Seven high-priority household and social contacts were identified and evaluated for TB in accordance with NTCA/CDC recommendations. Six of the seven contacts were screened with a TST; one was excluded because he was known to have had a positive TST result before contact with the patient. All six contacts had a positive TST (defined as induration >5 mm) (Table 2). Three of these contacts were male. None of the six contacts were foreign born. To locate workplace contacts, the patient's employer was contacted. The employer provided a list of approximately 500 employees who worked at the company, including their hire and termination dates. From this list, 79 employees were identified as high priority because they potentially traveled in vans with the patient to job sites during the 15-month period during which the patient was potentially infectious. Cooperation of the employer and coordination between the health department for the jurisdiction in which the patient resided and the health department for the jurisdiction in which the employer was based allowed for on-site evaluation and skin testing of workplace contacts within a few days. Because the NCTA/CDC guidelines emphasize that TST results might not be positive until at least 8--10 weeks after infection occurs (1), a second round of testing was conducted at the same location 10 weeks after the initial screening for contacts with negative TST results who had had exposure to the patient within the preceding 10 weeks. Of the 79 high-priority contacts identified at the workplace, 58 (73%) were contacted and evaluated within 1 week after being identified as contacts (Table 2). Four had prior positive TST results and had received treatment for LTBI before contact with the patient. Oral reports were verified with medical record documentation. The remaining 54 workplace contacts had either unknown or negative past TST status and were administered TSTs at the workplace. Twenty-one (39%) had positive TST results. Three (14%) of the 21 TST-positive workplace contacts were foreign born, compared with one (3%) of the 33 TST-negative workplace contacts. Six (29%) contacts, one of whom was foreign born, were identified as "converters" (i.e., persons who had a negative TST result during first-round testing and a positive TST result during second-round testing), suggesting recent transmission. According to the NCTA/CDC guidelines, the decision to expand a contact investigation should be based on 1) the extent to which high- and medium-priority contacts have been identified and tested and 2) the extent of recent transmission. In response to the unexpectedly high rate of infection in high-priority contacts (39%, which was more than twice the 8%--10% estimated background rate in this urban Maryland population) and the high proportion of high-priority contacts who were converters, the investigation was expanded to include potential low-priority contacts who had exposure at one or more of the 37 job sites where the patient installed furniture in Maryland, DC, and Virginia during the 15-month infectious period (1). One job included several overnight stays at a hotel; therefore, contacts at the hotel and a nearby bar also were included. To manage the multijurisdictional contact investigation, TB-control staff from all affected jurisdictions participated in a series of weekly conference calls. A total of 193 low-priority contacts associated with the 37 job sites in Maryland, DC, and Virginia were identified. Of these 193 contacts, 143 were located and administered a TST (Table 2). Twenty-one (15%) of 143 contacts had a positive TST result, a rate above the estimated background rate of infection of 8%--10% for Maryland, DC, and Virginia. Overall, contacts related to the patient's workplace and job sites constituted the majority of all identified contacts (95% [272 of 287 contacts]). No cases of TB disease were identified. Twenty (71%) of 28 medium- and high-priority contacts with LTBI agreed to begin treatment for LTBI, including all seven household, close social, and extended family TST-positive contacts and 13 (62%) of 21 TST-positive close workplace contacts. Although follow-up data were not complete, approximately 33% of low-priority contacts with LTBI agreed to begin treatment. Reported by: E Munk, G Maltas, S Dorman, MD, Johns Hopkins Medical Institutions; B Johnson, S Johnson, K Taylor, MD, Baltimore City Health Dept; J Thomas, C Campbell, Baltimore County Health Dept; L Gossett, MA, M Mentzer, Anne Arundel County Health Dept; Y Richards, T Walsh, MD, Montgomery County Health Dept; S Massey, L Federline, K Trimeloni, MSN, Prince George's County Health Dept; E Balm, J Dougé, MD, Frederick County Health Dept; M Miner, C Goldsborough, M Donovan, MA, W Cronin, PhD, D Blythe, MD, V Randle, MPH, N Baruch, MBA, Maryland Dept of Health and Mental Hygiene. R Jackson, Charlottesville/Albemarle Health Dept; J Moore, MHSA, W Heirendt, S Keller, MA, W White, M Tipple, MD, Virginia Dept of Health. D Hardge, J Hinnant, District of Columbia Dept of Health. G Mirchandani, PhD, EIS Officer, CDC. Editorial Note:When a patient with TB disease is identified, contact investigations are conducted to interrupt further transmission of TB by actively finding and treating additional persons with infectious TB disease. Contact investigations also help prevent future cases of TB disease by identifying and treating persons infected by the patient. In the United States, an average of 10--20 contacts are identified for each person with TB disease (2--4). Approximately 20%--30% of contacts have LTBI, and 1% have TB disease (2). Of the contacts with LTBI who progress to TB disease, approximately one half will have onset of TB disease within the first year after exposure (5,6). The NTCA/CDC guidelines suggest prioritization of contacts based on three main criteria: degree of infectiousness of the patient, age and immune status of contacts, and intensity and duration of exposure (1). Infectiousness is highest in patients with sputum that is smear-positive for AFB or those with cavitary lesions on a chest radiograph. Thus, contacts of pulmonary TB patients with positive sputum smears and cavitary lesions, such as the patient described in this report, are assigned the highest priority. Contacts aged <5 years and those with weakened immune systems because of human immunodeficiency virus infection or immunosuppressive drugs also are assigned the highest priority. None of the contacts of the patient described in this report were young children, and none were known to have compromised immune systems. Contacts with exposure in congregate settings or with exposure duration greater than the limits established by state or local health departments for high-priority contacts (e.g., the household, close social, and workplace contacts in this investigation) also are assigned the highest priority (1). A 2003 meta-analysis indicated that the mean prevalence of LTBI among workplace contacts of patients with TB disease was approximately 29% (range: 16%--51%) (7). The 39% rate of infection observed among close workplace contacts in this investigation is consistent with these prevalences. Exposure in small, enclosed spaces with poor ventilation, such as the vans in which the patient and his coworkers rode, are associated with greater transmission. Previous studies have demonstrated that workplace risk factors include carpooling with a person with TB disease and working on the same or subsequent shift as such a person (8). The high proportion (29%) of converters among TST-positive workplace contacts in this investigation suggests recent transmission. This finding is consistent with the patient becoming more infectious as his TB disease progressed over time, evidenced by the high AFB load detected in his sputum at the time of diagnosis. The findings in this report illustrate the usefulness of contact prioritization in TB investigations. A TB-infection rate of 42% (28 of 67 contacts) among high- and medium-priority contacts, compared with 15% (21 of 143 contacts) among low-priority contacts, demonstrates that the strategy used to identify and prioritize contacts effectively targeted those with the highest risk for infection. The findings in this report are subject to at least three limitations. First, accurately quantifying varying levels of exposure, especially among workplace contacts, was not possible. Beyond identifying persons who worked in contact with the patient and rode together in vans with him, calculating the total hours of exposure was not possible. Second, baseline TST information for most contacts identified in this investigation was lacking, thus limiting the ability to definitively attribute a high proportion of LTBI to the patient. However, a high percentage of U.S.-born TST-positive patients suggests recent transmission was likely. Finally, obtaining exact information on contacts from the patient was challenging because of recall bias resulting from the substantial length of time that the patient worked while potentially infectious. This investigation demonstrated that the workplace, which served as the main source of information about the majority of contacts, can be an effective starting place for obtaining a history of patient contacts. In this investigation, a substantial proportion of contacts was identified and screened through the patient's workplace. The investigation also made effective use of interjurisdictional relationships among state and local health departments in the national capital region. Contact investigations are one of the mainstays of TB-prevention measures because they enable identification and treatment of persons with TB. In an era of limited public health resources, prioritization of contacts for testing can be essential. Acknowledgments The findings in this report are based, in part, on contributions by M Davenport, Maryland Dept of Health and Mental Hygiene; and J Blair, PhD, and K Ijaz, MD, National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention. References
* The patient's sputum-smear grade was 4+. † Per DHMH guidelines, contacts meeting the following duration/environment limits should be categorized as high priority: >8 hours in a small, poorly ventilated space; >16 hours in a small, well-ventilated space; >24 hours in a classroom-sized space; or >100 hours in a large, open space. § Per DHMH guidelines, contacts not meeting the requirements for the high-priority category and meeting the following exposure duration/environment limits should be categorized as medium priority: >4 hours in a small space; >8 hours in a classroom-sized space; or >50 hours in a large, open space. ¶ Per DHMH guidelines, contacts with exposure below the duration/environment threshold for medium priority should be categorized as low priority. Table 1
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Date last reviewed: 1/30/2008 |
|||||||||
|