|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
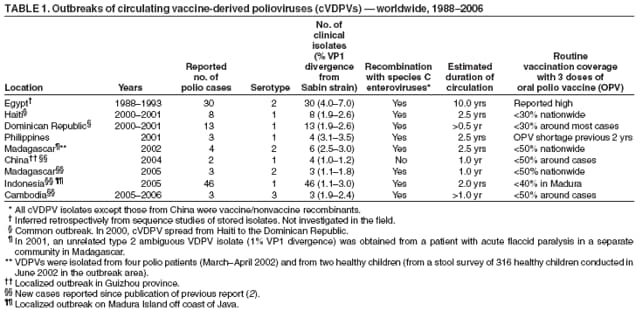
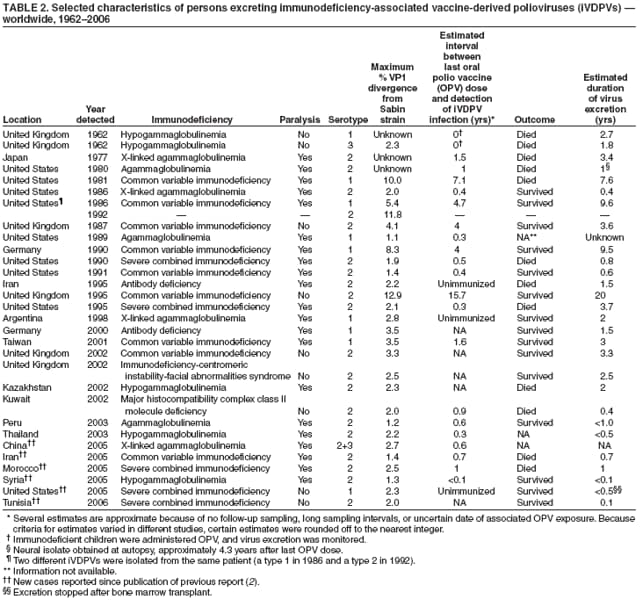
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Update on Vaccine-Derived PoliovirusesIn 1988, the World Health Assembly resolved to eradicate polio worldwide. The Global Polio Eradication Initiative (PEI) of the World Health Organization (WHO) has led to a decline in global polio incidence, from an estimated 350,000 cases in 1988 to fewer than 2,000 reported cases in 2005, and polio remains endemic to only four countries (Afghanistan, India, Nigeria, and Pakistan) (1). However, two additional obstacles to global eradication involve vaccine-derived polioviruses (VDPVs). Polio outbreaks continue to be associated with circulating vaccine-derived polioviruses (cVDPVs) in areas with low oral poliovirus vaccine (OPV) coverage. In addition, long-term excretion of neurovirulent immunodeficiency-associated vaccine-derived polioviruses (iVDPVs) can lead to poliovirus spread to contacts. Overcoming these obstacles is challenging. High rates of OPV coverage will prevent all poliovirus spread, including spread of VDPVs, but will not prevent establishment of prolonged VDPV infections in certain persons with B-cell immunodeficiencies (i.e., having defects in antibody production). Inevitable gaps in vaccination coverage will give rise to cVDPVs as long as OPV use continues. This report updates a previous report on VDPVs and describes the potential implications of VDPVs in the final stages of global polio eradication (2). The findings underscore the critical need to strengthen strategies to prevent emergence of VDPVs and to stop all OPV use once wild polioviruses (WPVs) are eradicated (2--5). Biologic Properties of VDPVsThe critical biologic properties of VDPVs are their capacity to cause paralytic polio in humans and their potential or demonstrated capacity for sustained circulation. VDPVs have lost key attenuating mutations and resemble WPVs biologically (2). All known cVDPVs (except those from China) (Table 1), but no iVDPVs, are recombinants with nonstructural protein sequences derived from species C enteroviruses, a property associated with poliovirus circulation (2). Most VDPVs are antigenic variants of the Sabin strains, but antigenic evolution appears to be faster in iVDPVs than in cVDPVs. Unlike cVDPV isolates, iVDPV isolates commonly contain mixed VDPV populations. These biologic distinctions (and the differing conditions favoring iVDPV and cVDPV emergence) have helped in recognition of the likely origins of many ambiguous VDPVs (aVDPVs) (2). Categories of VDPVsVDPVs differ from the majority of vaccine-related isolates by having genetic properties consistent with prolonged replication or transmission. Because poliovirus genomes evolve at a rate of approximately 1% per year, vaccine-related isolates that differ from the corresponding OPV strain by more than 1% of nucleotide positions (usually determined by sequencing the genomic region encoding the major viral surface protein, VP1) are estimated to have replicated for at least 1 year after administration of an OPV dose, substantially longer than the normal period of vaccine virus replication of 4--6 weeks. Poliovirus isolates are divided into three categories, identified by the extent of VP1 nucleotide sequence divergence from the corresponding Sabin OPV strain: 1) OPV-like viruses (<1% divergent), 2) VDPVs (1%--15% divergent), and 3) WPVs (>15% divergent) (2). VDPVs are further divided into 1) iVDPVs isolated from persons with primary immunodeficiencies who have prolonged VDPV infections after exposure to OPV, 2) cVDPVs that emerge in communities with inadequate OPV coverage, and 3) aVDPVs, which are clinical isolates from persons with no known immunodeficiency and environmental isolates whose ultimate source has not been identified (2). iVDPVsA small proportion of immunodeficient persons exposed to OPV have excreted iVDPV over prolonged periods (>6 months). WHO maintains an iVDPV registry; since the introduction of OPV in 1961--1962, only 30 persons excreting iVDPVs have been identified. Persons with primary B-cell immunodeficiencies, but not persons with T-cell immunodeficiencies (e.g., from human immunodeficiency virus infection), are at risk for iVDPV infections (6). Approximately 70% of iVDPV infections have spontaneously ceased within 3 years of exposure to OPV, or the patients have died from complications of their immunodeficiency. Five persons excreted virus for 3--8 years, and in three persons, the duration of excretion exceeded 9 years (Table 2). Eighteen (60%) documented iVDPV infections were associated with type 2 poliovirus infection, eight (27%) with type 1, one (3%) with type 3, and three (9%) with mixed infections (Table 2, Figure). The first reports of iVDPVs came from high-income countries (e.g., the United States, countries of Western Europe, and Japan) but recent reports of iVDPVs include middle-income countries (Table 2). No iVDPVs have been reported from low-income countries, where survival rates for persons with B-cell immunodeficiencies are low (7). Exposure usually is from receipt of OPV, but three of the known iVDPV infections occurred in unimmunized persons (Table 2). Strategies for resolving iVDPV infections are needed, both because of the risk for paralytic disease to infected persons and the risk for transmission to the wider community. No antiviral drug that has been shown to resolve iVDPV infections is currently available. However, new antiviral drugs broadly effective against VDPVs are under development (8). cVDPVsVDPVs do not circulate when high vaccination coverage leads to high population immunity. However, low vaccination coverage increases the proportion of nonimmune persons in a population; this increases the potential for VDPVs to circulate. Under circumstances of low vaccination coverage, cVDPVs have produced several localized polio outbreaks. Eight independent outbreaks (i.e., two or more polio cases) in eight countries have been associated with cVDPVs (Table 1, Figure). The largest documented outbreak (46 polio cases) occurred on the Indonesian island of Madura. Genetic studies on stored isolates suggest that a type 2 cVDPV circulated endemically in Egypt for 10 years (approximately from 1983 to 1993) and probably caused more polio cases than were reported (2). Outbreaks of cVDPVs have been associated with all three poliovirus serotypes. Two independent type 2 cVDPV outbreaks occurred in Madagascar in 2002 and 2005 (2), possibly signaling a higher potential for the emergence of type 2 cVDPVs. aVDPVsaVDPVs are VDPV isolates that cannot be clearly assigned to either of the other two well-defined categories. They have been isolated from paralyzed persons with no evidence of additional paralyzed VDPV-infected persons among household or community contacts. Highly divergent (>12% VP1 nucleotide divergence) aVDPVs also have been isolated from sewage in Estonia, Israel, and Slovakia. The sewage isolates have similar genetic and antigenic properties as iVDPVs, but measures to identify the infected persons have been unsuccessful. In 1966, aVDPVs were found in Belarus after local suspension of OPV use; in 1999, they were found in Russia among children in orphanages (2). A growing number of aVDPVs having VP1 sequence divergence slightly above 1% have been found by the Global Polio Laboratory Network. Limited person-to-person transmission for certain aVDPVs has occurred. In 2005, a type 3 aVDPV was isolated from one polio patient and seven nonparalyzed contacts in Madagascar. Similarly, a type 1 VDPV was isolated from one patient and seven contacts in Romania in 2002, a type 2 VDPV was isolated from one patient and two contacts in Laos in 2004 (2), a type 1 VDPV was isolated from an unimmunized severe combined immunodeficiency (SCID) patient and four community members in rural Minnesota in 2005 (9), and a type 1 VDPV was isolated from one patient and six contacts in Myanmar in 2006. Other aVDPVs with genetic properties resembling those of cVDPVs were found in Peru in 1983, in Pakistan in 2000, and in Nigeria in 2002 and 2006 (2). Risk Factors for VDPV EmergenceThe key factors favoring cVDPV emergence and spread are the same as for WPV circulation: low OPV coverage, poor sanitation, high population densities, and (usually) tropical conditions. In all but the remaining polio-endemic areas, immunity to polio is no longer acquired from natural infection; immunization is the only current means to prevent the spread of emerging VDPVs or imported WPVs (3). Although OPV is not recommended for immunodeficient patients, it is often inadvertently administered because certain primary immunodeficiencies (e.g., common variable immunodeficiency [CVID]) develop later in life. Certain persons with CVID who excrete iVDPVs had onset of polio several years after the implicated OPV dose was administered, and three have demonstrated no signs of paralysis. Survival of patients with primary immunodeficiencies can be extended in upper- and middle-income countries by intravenous immunoglobulin therapy; however, for patients in low-income countries, such therapy often is too expensive and difficult to obtain (7). Global VDPV SurveillanceSince the cVDPV outbreak in Haiti and the Dominican Republic in 2000--2001 (Figure, Table 1), all polioviruses isolated in the WHO Global Poliovirus Laboratory Network from patients with acute flaccid paralysis have been characterized by one molecular method, to identify polioviruses by their genetic properties (usually using the polymerase chain reaction), and one antigenic method, to detect antigenic differences from the OPV strains (using either an enzyme-linked immunosorbent assay [ELISA] or panels of specific neutralizing monoclonal antibodies) (10). Isolates found to be genetically related to an OPV strain but with antigenic differences are possible VDPVs. VP1 sequencing is routinely performed on all possible VDPV and WPV isolates. Approximately 12,000 isolates from all WHO regions have been routinely screened for VDPVs since 2001 (10). Temporal or geographic clustering of vaccine-related isolates of the same serotype has prompted the detection and investigation of cVDPV outbreaks in eight countries (Table 1). Reported by: WHO Global Poliovirus Laboratory Network. Immunization, Vaccines and Biologicals Dept, WHO, Geneva, Switzerland. Div of Viral Diseases and Global Immunization Div, National Center for Immunization and Respiratory Diseases (proposed), CDC. Editorial Note:VDPVs will continue to emerge as long as OPV is used. Intensified surveillance has indicated that cVDPVs can emerge repeatedly under conditions of low OPV coverage (e.g., Madagascar). VDPVs also can be found in developed countries with no paralytic cases (e.g., Estonia, Israel, and Slovakia) and can circulate in isolated pockets of unimmunized persons in countries with overall high rates of vaccination coverage (e.g., China and the United States). Although iVDPVs can emerge in middle-income developing countries, cVDPVs have not been found in some areas of high biologic risk, such as in northern India, presumably because of the current high rates of OPV coverage. Occurrences of VDPVs, including cVDPV-related outbreaks, are rare events, and all recent outbreaks of cVDPVs have been rapidly interrupted using OPV campaigns. The recent increase in the detection of VDPVs is probably primarily attributable to intensified surveillance and improved laboratory methods. Enhanced surveillance for VDPVs has allowed for better understanding of the risks associated with the different types of VDPVs. Areas with continued use of OPV but lacking optimal coverage (e.g., Indonesia in 2005) are at increased risk for cVDPV emergence. The importance of detecting aVDPVs with limited VP1 divergence is not clear; the presence of aVDPVs in certain settings might not have any public health consequences, whereas aVDPVs found elsewhere might signal conditions favoring the emergence of a cVDPV. Under certain circumstances, OPV viruses regain both neurovirulence and the capacity to circulate and cause outbreaks and therefore are of concern to the PEI. After global eradication of WPVs, the continued use of OPV would continually generate cVDPVs and could eventually pose a challenge to the goal of stopping all poliovirus infections in the human population. The increasing risk of cVDPV emergence in countries with widening immunity gaps and the ongoing risks for vaccine-associated paralytic polio and iVDPVs have prompted an evaluation of the feasibility of orderly cessation of OPV use as soon as possible in the posteradication era (4) while population immunity and surveillance sensitivity are still high (6). Continued development and implementation of a comprehensive strategy to minimize the risks for VDPV emergence in the posteradication era presents a challenge to the PEI and to the public health and scientific communities. References
|
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services. |
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Date last reviewed: 10/12/2006
|
|
|||||
|
HOME |
ABOUT MMWR |
MMWR SEARCH |
DOWNLOADS |
RSS
|
CONTACT
|
|||||
|
|
|||||
|