|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
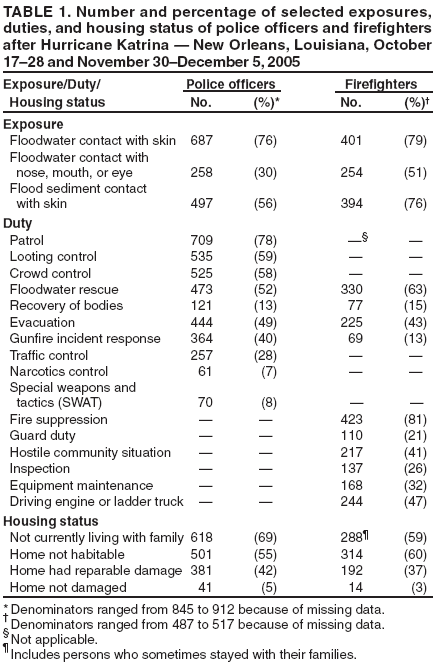
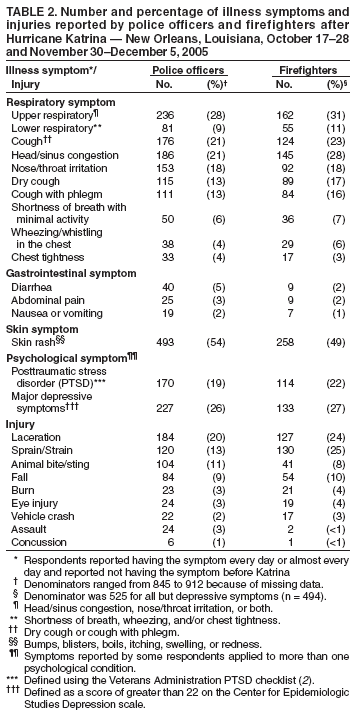
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Health Hazard Evaluation of Police Officers and Firefighters After Hurricane Katrina --- New Orleans, Louisiana, October 17--28 and November 30--December 5, 2005In the weeks after Hurricane Katrina struck the U.S. Gulf Coast on August 29, 2005, reports of increased injuries and symptoms of physical illness and psychological strain among New Orleans police officers and firefighters prompted CDC to conduct a health hazard evaluation of these two groups. Questionnaires were distributed to members of the New Orleans Police Department (NOPD) and New Orleans Fire Department (NOFD) 7--13 weeks after the hurricane. This report summarizes the results of that evaluation, which determined that upper respiratory and skin rash symptoms were the most common physical symptoms reported by police officers and firefighters and lacerations and sprains were the most common injuries. In addition, approximately one third of the respondents reported either depressive symptoms or symptoms of posttraumatic stress disorder (PTSD), or both. These results underscore the need to incorporate the safety and health of emergency responders into existing disaster preparedness plans and to provide periodic responder training and education in tasks unique to disaster situations. Clinical follow-up of the physical and psychological health of emergency responders should be conducted to better understand, monitor, and treat their health conditions. Investigators distributed survey questionnaires to NOPD members during October 17--28 and to NOFD members during November 30--December 5. The survey included questions about exposures to floodwater or floodwater sediment, work duties, housing status, physical and mental health symptoms, injuries, and whether medical care was sought. Respiratory and gastrointestinal symptoms were considered hurricane related if the respondent reported having the symptom every day or almost every day during the preceding 4 weeks and reported not having the symptom before Hurricane Katrina. A score of greater than 22 on the Center for Epidemiologic Studies Depression Scale was used to define major depressive symptoms (1), and the Veterans Administration checklist was used to define symptoms consistent with PTSD (2). NOPD officials estimated that 1,650 police officers were employed by the department before Hurricane Katrina, and 1,200--1,400 police officers were on duty at the time of the interviews; 912 police officers completed the questionnaire, resulting in an estimated overall participation rate of 65%--76%. NOFD officials reported 683 firefighters on its most recent (prehurricane) roster; 525 (77%) completed the questionnaire. Median age of participants was 37 years (range: 19--78 years) for police officers and 42 years (range: 20--64 years) for firefighters. Eighty percent of police officers and 96% of firefighters were male. Police officers had a median job tenure of 8 years (range: <1--41 years); median tenure for firefighters was 13 years (range: <1--40 years). Not all participants responded to all questions; the number of responses per question ranged from 845 to 912 for police officers and from 487 to 525 for firefighters. Floodwater contact with the nose, mouth, or eye was reported by 51% of firefighters (254 of 500) and 30% of police officers (258 of 864); 52% of police officers (473 of 910) and 63% of firefighters (330 of 524) reported rescuing citizens from flooded areas. Sixty-nine percent of police officers (618 of 899) and 59% of firefighters (288 of 490) reported that they were not living with their families at the time of the survey (Table 1). Police officers and firefighters reported similar prevalences of physical health symptoms. Approximately 28% of police officers (236 of 848) and 31% of firefighters (162 of 525) reported upper respiratory symptoms (i.e., head/sinus congestion or nose/throat irritation). Cough was reported by 21% of police officers (176 of 845) and 23% of firefighters (124 of 525). Skin rash was reported by 54% of police officers (493 of 909) and 49% of firefighters (258 of 525) (Table 2). Injuries most commonly reported by police officers and firefighters were lacerations (police officers: 20% [184 of 912] and firefighters: 24% [127 of 525]), sprains/strains (13% [120 of 912] and 25% [130 of 525]), falls (9% [84 of 912] and 10% [54 of 525]) and animal bites/stings (11% [104 of 911] and 8% [41 of 525]) (Table 2). Of 525 firefighters, 114 (22%) reported symptoms consistent with PTSD, and 133 of 494 (27) reported major depressive symptoms. Of 912 police officers, 19% (170) reported PTSD symptoms and 26% (227 of 888) reported major depressive symptoms. Among all police officers, 31% (279) reported seeing a health-care provider for post-hurricane illnesses and injuries; health-care utilization among firefighters was not assessed. Reported by: BP Bernard, MD, RJ Driscoll, PhD, Div of Surveillance, Hazard Evaluations, and Field Studies, M Kitt, MD, Div of Respiratory Disease Studies, National Institute for Occupational Safety and Health; CA West, MSN, MPH, SW Tak, ScD, EIS officers, CDC. Editorial Note:The findings from these surveys indicate that, 7--13 weeks after Hurricane Katrina, a substantial proportion of police officers and firefighters in New Orleans had injuries and symptoms of physical and mental illness. The prevalences of reported respiratory symptoms, skin rashes, and injuries were similar to those reported by Katrina relief workers through active CDC surveillance in the greater New Orleans area (3). The high prevalence of symptoms for PTSD and major depressive symptoms among police and firefighters is consistent with reports of increased risk for PTSD and depression after natural disasters (4,5). Police officers and firefighters also experienced stressors such as extended working hours, sleep deprivation, hostile communities, separation from their families, and destruction of their homes (6). The relation between floodwater exposure and reported symptoms of illness is not clear. Hazards in floodwaters vary but can include varying amounts of sewage, household and industrial chemicals, petroleum products, pesticides, and flammable liquids. Floodwaters also can obscure physical hazards (e.g., storm debris or drainage openings); other threats are posed by displaced domestic animals (7,8). The inherent dangers of the work of police officers and firefighters likely were compounded by the environmental hazards and personal stressors after Hurricane Katrina. In addition, certain police officers and firefighters were assigned to atypical activities (e.g., narcotic control officers who performed search and rescue operations) for which they might not have been adequately prepared. Full clinical diagnostic assessment of physical and psychological health is necessary to determine the breadth and scope of illness in persons with persistent symptoms. The National Institute for Occupational Safety and Health has prepared guidance for medical screening to assess the fitness of persons for deployment as recovery workers after a hurricane (9). These guidelines also can be used as a part of periodic medical evaluations to assess whether emergency responders meet minimal physical requirements to perform work duties. The findings in this report are subject to at least three limitations. First, only police officers and firefighters working at the time of the surveys were included, introducing the possibility of participation bias. Second, responses to traumatic events can provoke a range of reactions, including intensifying preexisting symptoms; therefore, new symptoms alone are not adequate to fully document physical or mental illness. Finally, even psychological symptoms persisting for >1 month might be normal and reversible acute stress and grief reactions; responses to the questionnaire alone are not sufficient to diagnose PTSD or major depression (10). Reducing risks for illness and injury to police officers, firefighters, and other emergency responders requires combining the capabilities of multiple government and private response agencies. Safety and health guidelines for emergency responders should be incorporated into existing disaster preparedness plans. These should include periodic disaster response training and education in tasks unique to disaster situations. Additional information regarding safety management strategies and guidance for emergency workers is available at http://www.cdc.gov/niosh/docs/2004-144, and comprehensive information regarding prevention of worker illness and injury after hurricanes and other natural disasters is available at http://www.cdc.gov/niosh/topics/flood. Acknowledgments This report is based, in part, on data contributed by E Page, MD, AL Tepper, PhD, B King, MPH, A Markey, MS, C Dowell, MS, C Mueller, MS, J Hurrell, PhD, K Mead, MS, A Warren, MPH, L Taylor-McKernan, MPH, T Hales, MD, L Ewers, PhD, Div of Surveillance, Hazard Evaluations, and Field Studies, and S Brown, MPH, National Institute for Occupational Safety and Health, CDC. References
|
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services. |
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Date last reviewed: 4/27/2006
|
|
|||||
|
HOME |
ABOUT MMWR |
MMWR SEARCH |
DOWNLOADS |
RSS
|
CONTACT
|
|||||
|
|
|||||
|