|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
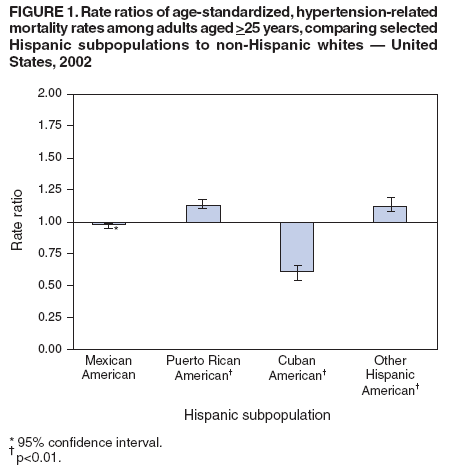
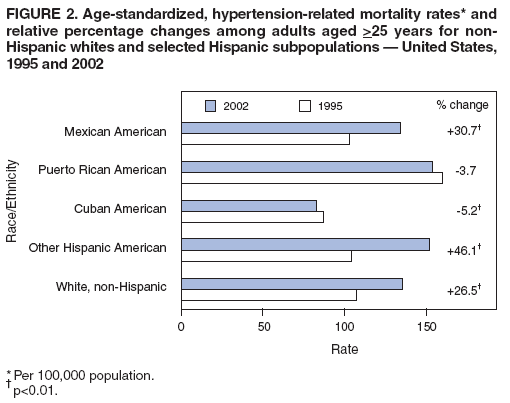
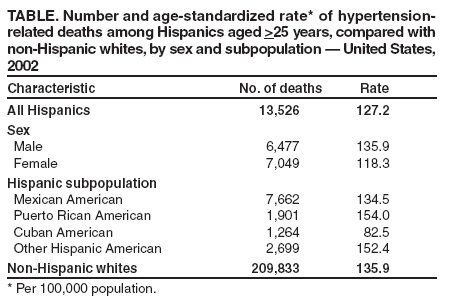
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Hypertension-Related Mortality Among Hispanic Subpopulations --- United States, 1995--2002Hypertension remains a major public health problem in the United States even though effective therapy has been available for more than 50 years (1). Hypertension is a strong independent risk factor for heart disease and stroke and a predictor of premature death and disability from cardiovascular complications (2). Although age-adjusted prevalence of hypertension is lower among Hispanics than among blacks or non-Hispanic whites (3--5), recent data indicate that certain Hispanic subpopulations (Mexican Americans, Puerto Rican Americans, Cuban Americans, and other Hispanic Americans) are characterized by low levels of hypertension awareness, treatment, and control. Because Hispanics are the fastest growing and youngest racial/ethnic population in the United States (6), targeted strategies to reduce morbidity and mortality rates among this population are essential. Since 1995, information on Hispanic ethnicity has been provided on nearly all death certificates issued in the United States.* Although data on Hispanic subpopulations are also available on death certificates, no national mortality statistics on hypertension-related deaths among specific Hispanic subpopulations have been published. To compare age-standardized, hypertension-related death rates among Hispanic subpopulations, CDC analyzed death certificate data from 1995 and 2002. This report describes the results of that analysis, which indicated that Puerto Rican Americans had consistently higher hypertension-related mortality (HRM) rates than all other Hispanic subpopulations and non-Hispanic whites. Comprehensive hypertension prevention and control programs are needed to target these Hispanic subpopulations. National death certificate data were obtained from the multiple cause-of-death files compiled by CDC. Most analyses of mortality data are based on the underlying cause of death (i.e., the disease or injury that initiated the sequence of events leading directly to death). However, hypertension is not only an important underlying cause of death but also is a common complicating factor for other disease. Therefore, in this report, hypertension-related mortality (HRM) includes those deaths for which hypertension (International Classification of Diseases, Ninth Revision (ICD-9) codes 401-404 for 1995 and ICD-10 codes I10-I13 for 2002) was reported either as the underlying cause or as a contributory cause of death (i.e., a condition reported on the death certificate other than the underlying cause). Included are deaths attributed to essential hypertension (i.e., high blood pressure with no identifiable cause), hypertensive heart disease, hypertensive renal disease, hypertensive heart and renal disease, and secondary hypertension. This report was limited to deaths occurring in the 50 states and the District of Columbia among U.S. residents aged >25 years. Age-standardized death rates based on the 2000 U.S. standard population were estimated for non-Hispanic whites, Hispanics, and four Hispanic subpopulations (Mexican Americans, Puerto Rican Americans, Cuban Americans, and other Hispanic Americans). Population denominators from the U.S. Census Bureau used to calculate death rates included postcensal estimates of the U.S. resident population for 2002 and intercensal population estimates for 1995. The change in HRM from 1995 to 2002 among Hispanic subpopulations was defined as the percentage change in age-standardized death rates. Non-Hispanic whites were the referent group for all estimates of HRM disparity. In 2002, a total of 13,526 hypertension-related deaths were reported among all Hispanics, compared with 209,833 among all non-Hispanic whites. The age-standardized HRM rate was 127.2 per 100,000 population for all Hispanics, similar to that of non-Hispanic whites (135.9). The age-standardized HRM rate for Hispanic women (118.3) was substantially lower than that observed for Hispanic men (135.9) (Table). Male HRM rates were higher than female rates for all Hispanic subpopulations. Puerto Rican Americans had the highest death rate among all Hispanic subpopulations (154.0), and Cuban Americans had the lowest (82.5). Compared with non-Hispanic whites, Puerto Rican Americans had 13% (p<0.01) higher age-standardized HRM rates; other Hispanic Americans were 12% (p<0.01) higher. Age-standardized HRM rates for Cuban Americans were 39% lower (p<0.01) than those for non-Hispanic whites. Rates for Mexican Americans did not differ significantly from non-Hispanic whites (95% CI = 0.97--1.01) (Figure 1). In 1995, age-standardized HRM rates (per 100,000 population) were highest among Puerto Rican Americans (159.9), followed by non-Hispanic whites (107.4), other Hispanic Americans (104.3), Mexican Americans (102.9), and Cuban Americans (87.0) (Figure 2). HRM rates increased for Mexican and other Hispanic Americans but decreased for Puerto Rican and Cuban Americans. The greatest percentage increase from 1995 to 2002 was 46.1% (p<0.01) for other Hispanic Americans, followed by increases of 30.7% (p<0.01) for Mexican Americans and 26.5% (p<0.01) for non-Hispanic whites. A 5.2% (p<0.01) decrease occurred from 1995 to 2002 among Cuban Americans, and a 3.7% decrease was observed among Puerto Rican Americans. Reported by: C Ayala, PhD, MR Moreno, MPH, JA Minaya, MPH, JB Croft, PhD, GA Mensah, MD, Div of Adult and Community Health, National Center for Chronic Disease Prevention and Health Promotion; RN Anderson, PhD, National Center for Health Statistics, CDC. Editorial Note:HRM rates increased substantially in the United States during 1995--2002, especially among the Hispanic population. This trend is most evident among Mexican Americans and other Hispanic Americans, who experienced the greatest percentage increases in HRM from 1995 to 2002. Although their HRM rate decreased slightly from 1995 to 2002, Puerto Rican Americans had the highest death rates during all years surveyed, compared with other Hispanic subpopulations and non-Hispanic whites. The higher HRM rates among Puerto Ricans might be the result of greater prevalence of the classic risk factors for hypertensive conditions, including diabetes mellitus, obesity, and physical inactivity in this population. Compared with non-Hispanic whites, Mexican Americans have a three- to five-fold higher incidence of diabetes mellitus and a three-fold higher prevalence of obesity (4); however, their HRM rates are only 4% higher than that of whites. In addition, Mexican American (39%) and Cuban American (34%) women are nearly as likely to be overweight as Puerto Rican American women (37%); however, they have lower HRM rates (7). Because diabetes and overweight are risk factors for hypertension, these higher prevalences could place these populations at higher risk for HRM in the future. The Hispanic population is estimated to account for approximately 13% (35.3 million) of the total 2000 U.S. population. On the basis of current trends, the Hispanic population is projected to increase 2% per year until 2030 and will account for 25% (81 million) of the total U.S. population by 2050. Similar demographic trends have also been projected for Hispanic subpopulations (3). A recent study revealed that, among hypertensive persons, Mexican Americans were less likely than non-Hispanic whites to be treated for hypertension (35% versus 49%, respectively) (5). Hispanics, although generally thought to have lower blood pressure as a population, received therapy for their hypertension in clinics only 50% of the time, and thus were at increased risk for HRM (8). Moreover, untreated hypertension elevates risk for mortality and morbidity from diseases of the heart and stroke, the first and third leading causes of death in the United States, respectively (9). The findings of this study are subject to at least two limitations. First, the multiple-cause mortality data are subject to errors in the certification of cause of death and in the reporting of Hispanic origin and Hispanic subpopulations. Problems associated with the underreporting of Hispanic origin on death certificates and undercoverage in population estimates are well documented (10). Second, misreporting and undercoverage might also vary by Hispanic subpopulation. However, the overall quality and completeness of the mortality data from the vital statistics system are a strength of this study. Two major Hispanic subpopulations (Mexican Americans and other Hispanic Americans) have HRM rates that have substantially increased from 1995 to 2002. Although HRM rates have also increased 26% in the general non-Hispanic population, the rate of increase for these subpopulations has been higher. Three factors might contribute to this growing burden: the increasing Hispanic population (3), the increased risk for HRM among Hispanics, and the low percentage of hypertensive Hispanics receiving therapy for hypertension (5). Only 45% of U.S. persons with hypertension receive therapy for their condition; this figure is considerably lower (34%) among Mexican Americans (5). Even fewer Mexican Americans have their hypertension under control (17%), compared with non-Hispanic whites (30%) (5). Awareness, treatment, and control of hypertension among members of these subpopulations is critical if the burden of hypertension and its serious heart disease and stroke sequelae are to be reduced. References
* Oklahoma did not provide this information until 1997.
Figure 1
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Date last reviewed: 2/23/2006 |
|||||||||
|