|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
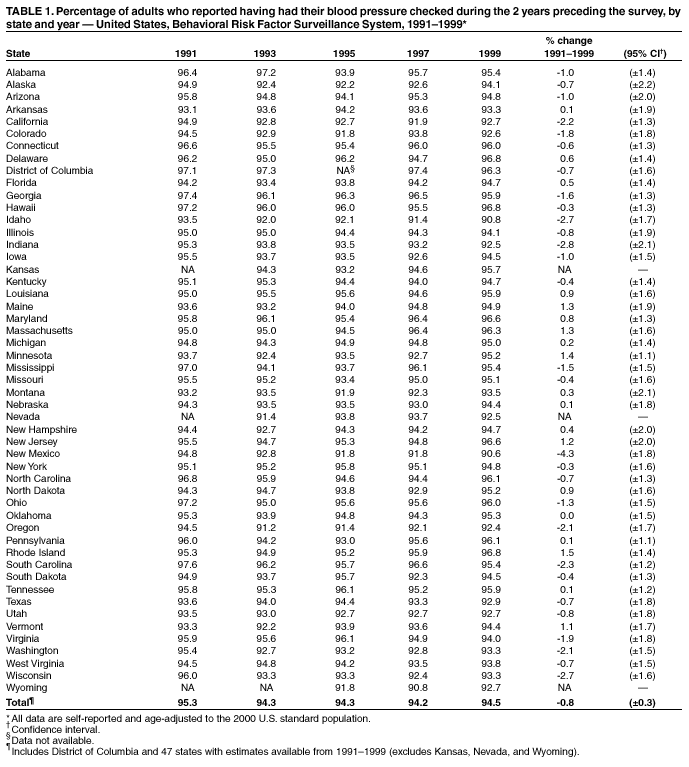
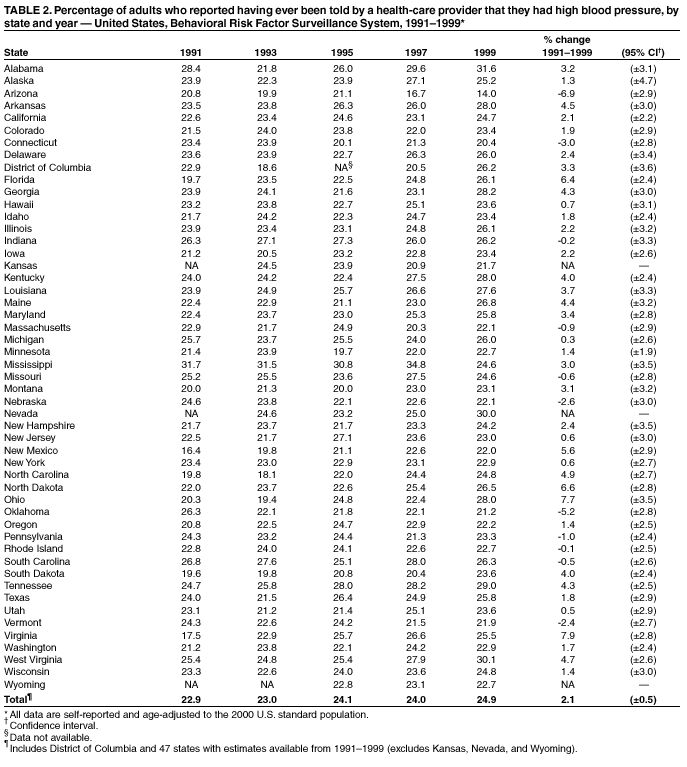
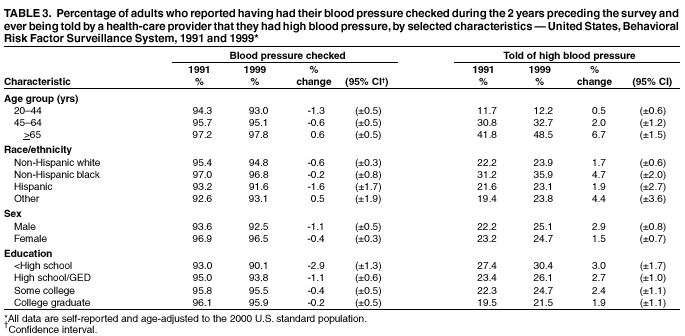
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. State-Specific Trends in Self-Reported Blood Pressure Screening and High Blood Pressure --- United States, 1991--1999High blood pressure (HBP) increases the risk for heart disease and stroke, the first and third leading causes of death in the United States, respectively. An estimated one in four U.S. adults has HBP, which is defined as taking antihypertensive medication or having either a systolic blood pressure (SBP) of >140 mmHg or a diastolic blood pressure (DBP) of >90 mmHg (1). Optimal blood pressure is defined as SBP of <120 mmHg or DBP of <80 mmHg. To reduce the prevalence of HBP in the United States, the National Heart, Lung, and Blood Institute initiated the National High Blood Pressure Education Program (NHBPEP) in 1972, recommending that all adults aged >20 years have their blood pressure (BP) checked at least once every 2 years. Although HBP is easily detectable and can usually be controlled with treatment, greater awareness of BP levels among U.S. adults is needed (2). This report summarizes data from the Behavioral Risk Factor Surveillance System (BRFSS) on state-specific trends in recent BP screening and prevalence of HBP (both by self-report). The findings indicate that during 1991--1999, BP screening levels were very high, and the percent of adults reporting HBP increased among some populations. Innovative education and intervention programs are needed to prevent and treat HBP in five high-risk groups: men, blacks, Hispanics, persons with less education, and older adults. BRFSS is a state-based, random-digit--dialed telephone survey of the civilian, noninstitutionalized U.S. population aged >18 years. CDC analyzed BRFSS data from 1991, 1993, 1995, 1997, and 1999 for persons from the 50 states and the District of Columbia (DC). The range of sample sizes for individual states was 1,163--3,404 in 1991, 1,182--4,294 in 1993, 1,184--5,052 in 1995, 1,437--4,877 in 1997, and 1,225--4,914 in 1999. BRFSS CASRO median response rates ranged from 70.9% in 1991 to 55.2% in 1999. These rates reflect both telephone sampling efficiency and the degree of cooperation among eligible respondents who were contacted. Survey participants were asked 1) about how long it had been since they last had their BP taken by a doctor, nurse, or other health-care professional, and 2) if they had ever been told by a doctor, nurse, or other health-care professional that they had HBP. Recent BP screening was defined if the respondent's blood pressure had been checked during the 2 years preceding the interview. Persons who reported that they were ever told they had HBP were classified as having self-reported HBP. Analyses were restricted to persons aged >20 years. Data were weighted and analyzed using SUDAAN (version 7.0) to account for the complex sampling design in each state and to obtain prevalence and variance estimates. Prevalences were age-adjusted to the 2000 U.S. standard population. The state-specific percentage point differences between 1991 and 1999 for recent BP screening and HBP were limited to DC and the 47 states that participated in BRFSS during 1991--1999. During 1991--1999, approximately 100% of adults reported that they ever had their BP checked. The age-adjusted prevalence of adults reporting that they had recent BP screening remained relatively constant at 95.3% in 1991 and 94.5% in 1999 (Table 1). The prevalence of recent BP screening declined in 30 states; the decline was statistically significant in 11 states (California, Georgia, Idaho, Indiana, Mississippi, New Mexico, Oregon, South Carolina, Virginia, Washington, and Wisconsin). Recent BP screening increased significantly in Minnesota, New Jersey, North Dakota, and Vermont. The age-adjusted prevalence of adults reporting having ever been told that they had HBP increased significantly from 22.9% in 1991 to 24.9% in 1999 (Table 2). In 1999, age-adjusted prevalence of self-reported HBP ranged from 14.0% in Arizona to 31.6% in Alabama. During 1991--1999, statistically significant increases in age-adjusted prevalence of self-reported HBP were observed in 17 states (Alabama, Arkansas, Florida, Georgia, Kentucky, Louisiana, Maine, Maryland, New Mexico, North Carolina, North Dakota, Ohio, South Dakota, Tennessee, Virginia, Washington, and West Virginia). Significant declines were observed in Arizona, Connecticut, and Oklahoma. In 1991 and 1999, age-specific prevalences of recent BP screening and self-reported HBP were higher among adults aged >65 years than among those aged 20--64 years (Table 3). Recent BP screening declined significantly among persons aged 20--44 years and those aged 45--64 years, but increased among those aged >65 years. Prevalences of self-reported HBP increased in all age groups except among persons aged 20--44 years. In 1991 and 1999, age-adjusted prevalences of recent BP screening were higher among non-Hispanic blacks, women, and persons with >12 years of education compared, respectively, with those of other racial/ethnic groups, men, and persons with less education. However, recent BP screening declined significantly among non-Hispanic whites, men, women, and persons with <12 years of education. In 1999, age-adjusted prevalences of self-reported HBP were higher among non-Hispanic blacks than among other racial/ethnic groups, among men than among women, and among persons with less education. Self-reported HBP increased during 1991--1999 among almost all groups, irrespective of race/ethnicity, sex, or education. Reported by: C Ayala, PhD, KJ Greenlund, PhD, JB Croft, PhD, LJ Neff, PhD, S Dai, PhD, ZJ Zheng, MD, ML Casper, PhD, NL Keenan, PhD, GA Mensah, MD, Div of Adult and Community Health, National Center for Chronic Disease Prevention and Health Promotion, CDC. Editorial Note:The findings in this report indicate that although BP screening prevalences were high in all states and demographic groups, the lowest levels were among men, Hispanics, persons with less education, and younger adults, suggesting that ongoing programs should increase efforts to reach these populations. Factors that might be associated with disparities in some groups and in some states include differences in perception of the risk for heart disease and stroke and the benefits of lowering BP, limited access to quality health care, and limited socioeconomic resources (3). Although data on prevalences of treatment and control of HBP were not available in this BRFSS report, the impact of uncontrolled HBP on cardiovascular disease is an important public health issue. The National Health and Nutrition Examination Surveys (NHANES) based on actual blood pressure measurements suggest that the age-adjusted (2000 standard) prevalence of HBP declined from 39.8% during 1971--1974 to 23.9% during 1988--1991 (4). However, BRFSS data suggest increases during 1991--1999 in the percentage of the U.S. population who have ever been told by a health-care provider that they had HBP. Although a real increase in the prevalences of HBP is possible in association with observed increases in the prevalence of obesity and being overweight (5), the increase in reported HBP also might be associated with increased detection and reporting of conditions by health-care providers to their patients. The findings in this report are subject to several limitations. First, estimates of self-reported HBP depend both on screening and awareness of BP measurements and might be overstated if patients reported having HBP but actually had been told that they had high-normal or borderline HBP. Conversely, prevalences might be underestimated if members of a population were not screened and were unaware of their BP status. In a study using similar questions, the sensitivity and specificity of self-reported HBP was high compared with actual HBP or use of BP medications (6). Second, because interstate migration was high during the 1980s and 1990s, current state prevalences cannot be assumed to reflect the prevalences among long-term state residents (7). Third, the declining median response rates in the BRFSS (from 70.9% to 55.2%) could affect measurements over time. Fourth, BRFSS excludes an unknown number of persons in institutions and all persons aged <18 years. Fifth, because BRFSS is a telephone-based survey, persons of low socioeconomic status who are less likely to have a telephone might not have been included in representative numbers. Finally, because time and functional capacity are required for participation in the questionnaire, BRFSS might underrepresent those with a severe impairment. Estimates of self-reported HBP depend on screening, awareness of BP measurements, and the accurate reporting of HBP rather than clinical diagnoses such as high-normal or borderline HBP. HBP is a major modifiable risk factor for cardiovascular diseases, and BP screening is an important first step in identifying and controlling HBP and preventing heart disease and stroke. Clinical guidelines for BP screening and management emphasize prevention of HBP by improving lifestyles, self-measurement of BP, the use of new combination antihypertensive medications, and strategies for improving adherence to treatment (2). Many CDC-sponsored state cardiovascular health programs, the NHBPEP, and the American Heart Association provide programs that raise public awareness and understanding about HBP as a risk factor for heart disease and stroke. Eleven states (Alaska, California, Connecticut, Illinois, Iowa, Massachusetts, Michigan, Nebraska, North Carolina, South Dakota, and Vermont) provide BP screening and other services to participants in the National Breast and Cervical Cancer Early Detection program (8). Some states use prevention block grant funds to conduct BP screening campaigns that target priority populations (e.g., younger members of certain racial/ethnic groups or older adults). In addition to these ongoing public health efforts, prevention programs are encouraged to seek innovative strategies to ensure that high BP screening rates continue among priority populations. Acknowledgments This report is based on data contributed by the following BRFSS coordinators: S Reese, MPH, Alabama; P Owens, Alaska; R Weyant, Arizona; B Woodson, Arkansas; B Davis, PhD, California; B Rosenblatt, Colorado; M Adams, MPH, Connecticut; F Breukelman, Delaware; J Davies-Cole, District of Columbia; S Oba, MSPH, Florida; L Martin, MS, Georgia; F Reyes-Salvail, MS, Hawaii; J Aydelotte, MA, Idaho; B Steiner, MS, Illinois; L Stemnock, Indiana; D Sheperd, PhD, Iowa; M Arnold, Kansas; T Sparks, Kentucky; B Bates, MSPH, Louisiana; J Graber, MS, Maine; H Lopez, Maryland; Z Zhang, MPH, Massachusetts; H McGee, MPH, Michigan; N Salem, PhD, Minnesota; D Johnson, MS, Mississippi; J Jackson-Thompson, PhD, Missouri; P Feigley, PhD, Montana; L Andelt, PhD, Nebraska; E DeJan, MPH, Nevada; J Porter, MPH, New Hampshire; G Boeselager, MS, New Jersey; W Honey, MPH, New Mexico; C Baker, New York; Z Gizlice, PhD, North Carolina; L Shireley, MPH, North Dakota; P (Pullen) Cross, Ohio; K Baker, MPH, Oklahoma; K Pickle, MPH, Oregon; L Mann, Pennsylvania; J Hesser, PhD, Rhode Island; DJ Goodwin, DrPH, South Carolina; M Gildemaster, South Dakota; D Ridings, Tennessee; K Condon, MS, Texas; K Marti, Utah; R McCormick, PhD, Vermont; G Seifen, MS, Virginia; KW Simmons, PhD, Washington; F King, West Virginia; K Pearson, Wisconsin; M Futa, Wyoming. References
|
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services. |
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 5/30/2002
|
|
|||||
|
HOME |
ABOUT MMWR |
MMWR SEARCH |
DOWNLOADS |
RSS
|
CONTACT
|
|||||
|
|
|||||
|
This page last reviewed 5/30/2002