|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
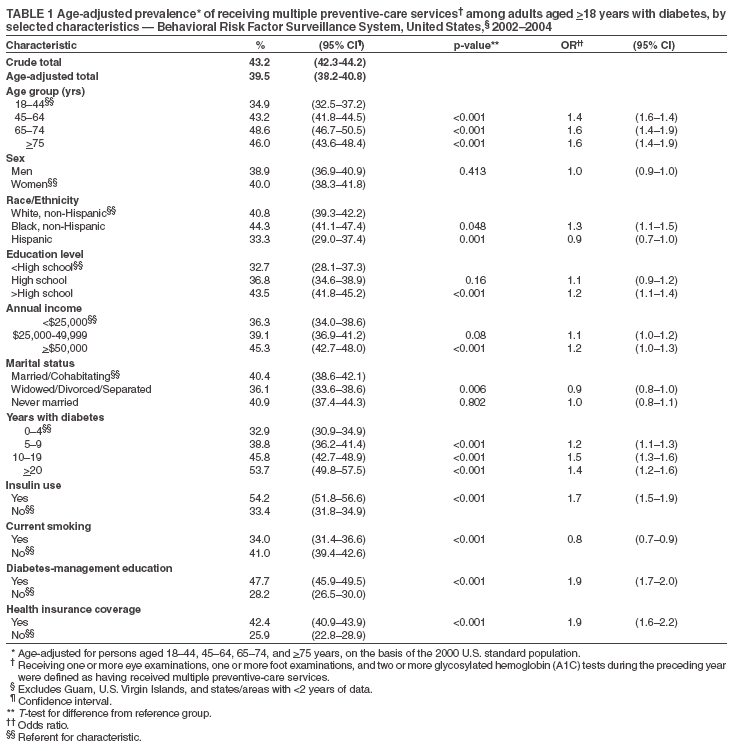
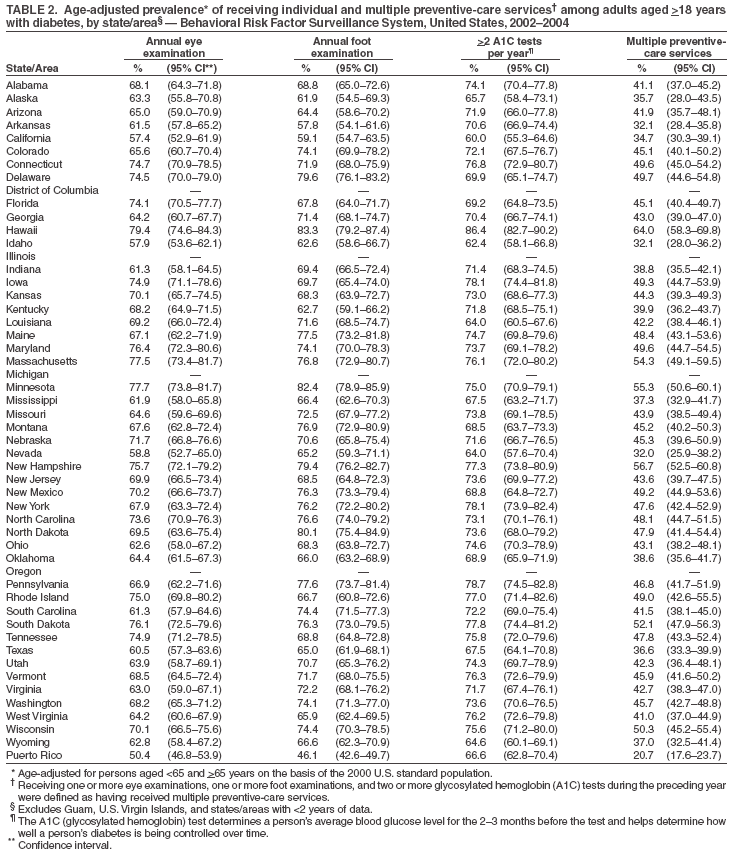
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Prevalence of Receiving Multiple Preventive-Care Services Among Adults with Diabetes --- United States, 2002--2004An estimated 7% of the U.S. population has diabetes; however, only 70% of these persons have had the disease diagnosed (1). Recommended preventive-care services such as annual foot and eye examinations can prevent or delay amputation and blindness (2,4). Measurement of glycosylated hemoglobin (A1C) two or more times per year is important for glycemic control and diabetes management (3,4). Three national health objectives for 2010 are to increase the proportion of adults with diabetes who have an annual dilated eye examination (objective no. 5-13; target: 75%), an annual foot examination (objective no. 5-14; target: 75%), and A1C measurements at least twice each year (objective no. 5-12; target: 50%) (5). To determine the percentage of U.S. adults with diabetes receiving each of these three preventive-care services and the percentage receiving all three services, CDC analyzed data from Behavioral Risk Factor Surveillance System (BRFSS) surveys for 2002--2004. This report summarizes the results of that analysis, which determined that four in 10 U.S. adults with diabetes reported receiving all three preventive-care services; persons with recently diagnosed diabetes and current smokers were least likely to receive all three preventive-care services. Increased understanding of barriers to receiving multiple preventive-care services and continued interventions to ensure their delivery can improve the health status of persons with diabetes. BRFSS is an ongoing, state-based, random-digit--dialed telephone survey of noninstitutionalized civilian adults aged >18 years. Median response rates among the state surveys were 58.3% (range: 42.2%--80.5%) in 2002, 53.2% (range: 34.4%--80.5%) in 2003, and 52.7% (range: 32.2%--66.6%) in 2004. Persons with diabetes were defined as respondents who answered "yes" to the core question, "Has a doctor ever told you that you have diabetes?" Those with prediabetes or borderline diabetes and women who were told they had diabetes but only during pregnancy were classified as not having diabetes. Among persons with diabetes, 70% responded to the following three diabetes module questions and were included in the analyses: "When was the last time you had an eye exam in which the pupils were dilated?" , "About how many times in the last year has a health professional checked your feet for any sores or irritations?" (persons who indicated having bilateral amputations were not asked this question), and "About how many times in the last year has a doctor, nurse, or other health professional checked you for glycated hemoglobin or hemoglobin A1c?" Those who reported one or more eye examinations, one or more foot examinations, and two or more A1C tests during the preceding year were defined as having received multiple preventive-care services. Data were available from 47 states and Puerto Rico for the analysis. Persons with missing data and areas with <2 years of data were excluded from the analysis. Data were weighted to reflect the age, sex, and racial/ethnic distribution of noninstitutionalized U.S. adults, and all estimates were age-adjusted to the 2000 U.S. adult population. T-tests were used to determine statistically significant differences between groups and populations. Multiple logistic regression analysis was used to determine whether selected characteristics (e.g., age, race/ethnicity, income, and health insurance) were associated significantly with receipt of multiple preventive-care services. Of 807,771 survey respondents, 65,441 reported diabetes. Among those responding, the overall age-adjusted weighted prevalence of those receiving multiple preventive-care services was 39.5% (Table 1), ranging from 20.7% in Puerto Rico to 64.0% in Hawaii (median: 44.7%) (Table 2). The following six states/areas reported prevalence of >50% for receipt of multiple preventive-care services: Hawaii (64.0%), New Hampshire (56.7%), Minnesota (55.3%), Massachusetts (54.3%), South Dakota (52.1%), and Wisconsin (50.3%) (Table 2). Prevalence of receiving multiple preventive-care services was significantly lower (p<0.001) among persons aged 18--44 years than among those aged >45 years, lower among Hispanics than non-Hispanic whites, and lower among current smokers than among nonsmokers or former smokers (Table 1). Prevalence was significantly higher (p<0.001) among persons with the following characteristics: having more than a high school education, annual income of >$50,000, duration of diabetes of >4 years, insulin use, receiving diabetes-management education, and having health insurance coverage (Table 1). Multivariate analyses determined that the following characteristics were significantly associated with the likelihood of receiving multiple preventive-care services: aged >75 years (odds ratio [OR] = 1.6), non-Hispanic black (OR = 1.3), more than a high school education (OR = 1.2), duration of diabetes of 10--19 years (OR = 1.5), insulin use (OR = 1.7), receiving diabetes-management education (OR = 1.9), and having health insurance coverage (OR = 1.9) (Table 1). Current smoking (OR = 0.8) was negatively associated with receiving multiple preventive-care services. Reported by: Q Mukhtar, PhD, L Pan, MD, L Jack Jr, PhD, DL Murphy, MPH, Div of Diabetes Translation, National Center for Chronic Disease Prevention and Health Promotion, CDC. Editorial Note:This report is the first population-based assessment of the receipt of multiple preventive-care services among persons with diabetes. Although the percentage of persons with diabetes receiving individual preventive-care services (e.g., foot or eye examinations and A1C tests) in certain states is close to or above the national targets (75% for foot and eye examinations and 50% for A1C tests) (5), more than half of those with diabetes reported they had not received all three preventive-care services. This prevalence is low even among those with favorable characteristics (e.g., having health insurance coverage, receiving diabetes-management education, and being in high education or income groups). Possible barriers to not receiving all three recommended preventive-care services might include lack of awareness, inadequate health insurance coverage, and inability to make co-payments or visit specialists. Effective management of diabetes requires persons with diabetes and health-care providers to be aware of the need for multiple preventive-care services and a multidisciplinary approach to care. Expansion of preventive-care services available through health plans might be needed to improve the affordability and availability of multiple services (6). However, further research is needed to increase understanding of individual, social, and environmental barriers to persons with diabetes receiving multiple preventive-care services. The findings in this report are subject to at least three limitations. First, persons living in long-term--care facilities or in households with no telephone or only a cellular telephone are not included in BRFSS surveys; thus, these results do not reflect the entire U.S. population. Second, BRFSS data are self-reported and subject to recall bias; further investigation is needed particularly to assess the reliability and validity of self-reports for foot examinations and A1C tests. Nonetheless, validation studies have indicated that self-reported diabetes and dilated eye examinations are accurate (7,8). Finally, only three of the preventive-care services recommended to persons with diabetes were evaluated; incorporating additional recommended services (e.g., influenza and pneumococcal vaccination) likely would yield even lower prevalence of multiple preventive-care services. CDC supports 59 diabetes prevention and control programs, one in each state and territory, to 1) increase awareness about diabetes and diabetes management, 2) work with health systems to improve the quality of diabetes care, 3) encourage early detection of diabetes and diabetes-related complications, and 4) monitor trends in the burden of diabetes and quality of care received by persons with diabetes. In addition, CDC partners with the Health Disparities Collaborative,* and CDC and the National Institutes of Health jointly sponsor the National Diabetes Education Program,† which develops educational tools and community-based interventions and establishes public- and private-sector partnerships to improve diabetes prevention, treatment, and outcomes and to promote early detection. References
* Available at http://www.healthdisparities.net/hdc/html/collaboratives.topics.diabetes.aspx. † Available at http://www.ndep.nih.gov. Table 1
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Date last reviewed: 11/9/2005 |
|||||||||
|