|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
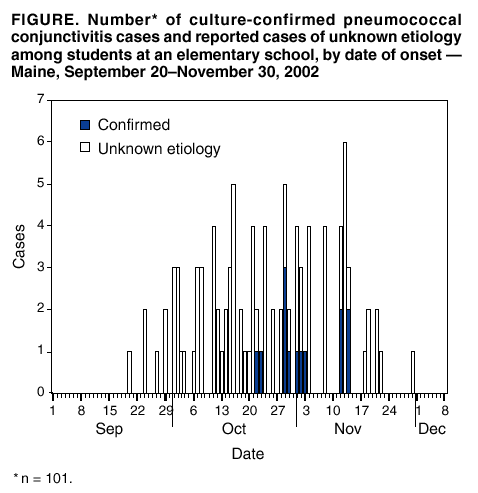
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Pneumococcal Conjunctivitis at an Elementary School --- Maine, September 20--December 6, 2002On October 18, 2002, the nurse at an elementary school in Westbrook, Maine, notified the Maine Bureau of Health (MBOH) of an increase in the number of students with conjunctivitis. During September 23--October 18, a total of 31 students in kindergarten and in first and second grades either were reported by parents to the nurse as having conjunctivitis or had conjunctivitis diagnosed by the nurse at school. Conjunctival swab cultures from five (38%) of the 13 students who were tested initially grew Streptococcus pneumoniae. This report documents additional cases in the community and summarizes preliminary results of the investigation of this outbreak, which indicated that the outbreak was caused by the same nontypeable strain of pneumococcus that caused an outbreak of conjunctivitis among college students in New Hampshire during January--March 2002 (1). This is the first time that this strain has been reported as the cause of a conjunctivitis outbreak among schoolchildren. Health-care providers and public health officials should be aware that nontypeable S. pneumoniae can cause outbreaks of conjunctivitis in school-age children and college students; outbreaks should be reported to state health departments and CDC. School nurses and child care center managers were asked to report to MBOH any children or staff member who had onset of conjunctivitis during September 20--December 6. Reported episodes of conjunctivitis were considered culture-confirmed if S. pneumoniae was isolated from eye secretions. A questionnaire to identify children and family members with conjunctivitis was sent home with all children attending the index elementary school. Among 361 students, 101 (28%) (median age: 6 years; range: 5--8 years) had at least one episode of conjunctivitis, and 11 (55%) of 20 students tested had an episode of culture-confirmed pneumococcal conjunctivitis (Figure). The attack rate was highest among first-grade students (51 [38%] of 136), followed by morning kindergarten (20 [29%] of 70), second-grade (28 [26%] of 108), and afternoon kindergarten students (two [4%] of 47). Among school staff, three (13%) of 23 classroom teachers and three (15%) of 20 other staff members had conjunctivitis during the study period. Of 709 family members who did not attend the school, 37 (5%) (median age: 4 years; range: <1--42 years) reported conjunctivitis; 28 (76%) of the 37 were household contacts of students who were ill previously. Of 221 household contacts of students with conjunctivitis, 28 (13%) reported having conjunctivitis with onset after the student's illness. A second questionnaire was distributed to all students in selected classrooms. Among 65 students with conjunctivitis who responded, the symptoms reported most commonly were red eyes (55 [85%]); itchy, painful, or burning eyes (45 [69%]); crusty eyes in the morning (42 [65%]); grey or yellow discharge from eyes (42 [65%]); and swelling of the eyelids (30 [46%]). Redness in both eyes was reported for 35 (64%) of the 55 students who had red eyes. The median duration of symptoms was 3 days (range: 1--14 days). Of the 65 students, 53 (82%) missed school during their illness, with a median absence from school of 2 days (range: 1--7 days). Symptoms of systemic pneumococcal infections were not identified in any of the students or contacts. School nurses and child care staff in the community reported an additional 77 students who had conjunctivitis with onset during September 20--December 2, including 53 (4%) of 1,313 students, ranging from kindergarten through grade 12 at four schools, and 24 (9%) of 271 children attending three community child care centers. Among the 53 students with conjunctivitis at other schools, 10 (19%) had a family member at the index school, and seven (29%) of 24 ill child care attendees had a sibling at the index school. Of 20 conjunctival specimens collected from students at the index school and 15 collected from students at other schools, 11 (55%) and five (33%), respectively, grew S. pneumoniae. All seven isolates that were tested for antimicrobial susceptibility were resistant to erythromycin but susceptible to penicillin and third-generation cephalosporins. Nine isolates were sent to CDC for serotyping; eight could not be typed by using CDC antisera, and one isolate from a conjunctival swab collected from an index school student was serotype 38. Nontypeable isolates, but not the serotype 38 isolate, produced identical electrophoretic patterns by pulsed field gel electrophoresis to pneumococcal isolates from an outbreak of conjunctivitis on a college campus in New Hampshire during January--March 2002 (1). Viral cell cultures of specimens from 30 students were negative for adenovirus (i.e., no cytopathic effect in cell culture was identified after 10 days' incubation). To prevent transmission at the school, students and teachers were encouraged to wash hands frequently with soap and water and to clean and limit the sharing of objects in the classroom. In addition, symptomatic children were excluded from school. Implementing prevention measures in this setting was difficult. Teachers reported that increased hand washing at school was disruptive to classes, and excluding symptomatic students from school placed a burden on parents. One student from the index school was reported as having conjunctivitis during Thanksgiving recess (November 25--29), and no children were reported with conjunctivitis after the recess. Five students at other schools were reported to have had conjunctivitis after the recess. Surveillance for additional cases of conjunctivitis at area schools is continuing. Reported by: C Leighton, Westbrook School District, Westbrook; D Piper, MS, NorDx Laboratories, Scarborough; J Gunderman-King, V Rea, MPH, K Gensheimer, MD, J Randolph, R Danforth, L Webber, E Pritchard, MS, G Beckett, MPH, Maine Bur of Health. V Shinde, MPH, R Facklam, PhD, C Whitney, MD, Div of Bacterial and Mycotic Diseases, National Center for Infectious Diseases; N Hayes, MD, Div of Applied Public Health Training, Epidemiology Program Office; B Flannery, PhD, EIS Officer, CDC. Editorial note: This report describes an outbreak in an elementary school of conjunctivitis attributed to a nontypeable strain of S. pneumoniae. Nontypeable pneumococci have been implicated previously in outbreaks of conjunctivitis among university students (1,2) and military recruits (2,3) and in sporadic cases of conjunctivitis (4). This is the first report of an outbreak of conjunctivitis caused by nontypeable pneumococci involving young children, with documented transmission to persons in the community outside the institutional setting. Although children were not seriously ill, the outbreak resulted in lost school days for ill children and in economic losses and inconvenience for parents of ill children for health-care provider visits and missed work. The effectiveness of prevention measures for interrupting the transmission of conjunctivitis is not known. Person-to-person transmission of the outbreak strain is believed to occur through contact with eye secretions or respiratory droplets. In schools, ensuring regular hand washing might improve hygiene among students but might not be sufficient to stop transmission of a highly contagious organism, especially one transmitted through respiratory droplets. Use of alcohol-based hand gels has been shown to prevent the transfer of pathogens in health-care settings (5), but their use in schools has not yet been evaluated. Although the effectiveness of excluding students with symptoms of conjunctivitis from school to limit a recognized outbreak is not known, such exclusion is recommended during the acute phase of symptoms (6). In the absence of clinical signs of systemic infection, the American Academy of Pediatrics recommends readmission of school children with conjunctivitis after therapy is initiated (7). Although antibiotic eye drops are prescribed commonly as empiric therapy for conjunctivitis, the effect of topical antibiotic therapy on transmission of pneumococcal conjunctivitis is unknown. The results from one trial indicated that persons treated with bacitracin/polymyxin opthalmic ointment were more likely to have eradication of eye pathogens at 3--5 days than persons treated with a placebo (8). Health-care providers who see a substantial increase in visits for conjunctivitis should consider obtaining bacterial and viral cultures of eye secretions to determine the etiology. CDC is interested in evaluating the effectiveness of control measures and the usefulness of topical antibiotic therapy in future outbreaks caused by S. pneumoniae. Outbreaks of S. pneumoniae conjunctivitis should be reported to state health departments, which may contact CDC, telephone 404-639-2215, for additional assistance. Acknowledgments This report is based on data contributed by J Flaherty, P Sanfino, L Allen, E Greaterex, D Bruns, Westbrook School District; A Hebert, T Levesque, D Porter, Westbrook; local health-care providers, Cumberland County, Maine. J Elliott, PhD, D Jackson, MS, R Besser, MD, Div of Bacterial and Mycotic Diseases; W Trick, MD, S Fridkin, MD, Div of Healthcare Quality Promotion, National Center for Infectious Diseases, CDC. References
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 1/30/2003 |
|||||||||
This page last reviewed 1/30/2003
|