 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Outbreak of Bacterial Conjunctivitis at a College --- New Hampshire, January--March, 2002During February 1--14, 2002,approximately 100 students presented to a New Hampshire college's student health service with clinical signs of conjunctivitis (Figure 1). The cause of conjunctivitis was initially thought to be viral. However, because of the high number of cases, eye cultures were collected from 12 consecutive students; Streptococcus pneumoniae was isolated from cultures of all 12 students. The medical director of the student health service notified the New Hampshire Department of Health and Human Services about the outbreak and on February 22, the state health department requested assistance from CDC. This report summarizes preliminary results of the investigation of this outbreak, which indicate that an uncommon strain of pneumococcus caused this outbreak and that health-care providers should consider pneumococcus as a cause of conjunctivitis among college students. Students at the college are entitled to medical care at the student health service, and school officials estimate that approximately 95% of students use the health service for nonemergency health care. Discharge diagnoses of visits to the student health center were reviewed to identify episodes of conjunctivitis. A case of probable pneumococcal conjunctivitis was defined as a diagnosis of conjunctivitis-unspecified (International Classification of Diseases, Ninth Revision [ICD-9] code 372.30), pink eye or mucopurulent conjunctivitis (ICD-9 code 372.03), or viral conjunctivitis (ICD-9 code 077.99) in a student who presented to the student health service during January 15--March 7, 2002. A case of confirmed pneumococcal conjunctivitis was defined as a diagnosis of conjunctivitis with S. pneumoniae isolated from eye secretions. Among 5,060 students enrolled for the winter term, 493 (9.7%) students had probable pneumococcal conjunctivitis, and 81 (1.6%) had confirmed pneumococcal conjunctivitis (Figure 1). The attack rate was highest among freshmen (18.0%) followed by sophomores (14.9%), juniors (12.8%), seniors (12.0%), and graduate students (1.7%). A survey of college faculty and interviews with local child care centers, schools, ophthalmologists, and primary-care physicians did not identify excessive episodes of conjunctivitis in persons other than college students. A systematic clinical examination of 80 students with conjunctivitis found that most reported eye crusting on awakening. The findings of eye examinations were variable, ranging from mildly inflamed conjunctiva with a clear watery discharge to severe conjunctival inflammation with purulent discharge and preauricular adenopathy (Figure 2). Students examined by an ophthalmologist showed a papillary rather than follicular conjunctival response. Giemsa stains of conjunctival discharge from seven students showed lancet-shaped diplococci in a preponderance of neutrophils. No smears showed a predominantly lymphocytic response or viral inclusions. Students were treated with topical antibiotics. Of eye specimens cultured from 189 students, 81 (42.9%) grew bacteria identified as S. pneumoniae by optochin sensitivity and bile solubility tests. Strains were resistant to erythromycin but susceptible to balcitracin, sulfonamides, and quinolones. Thirty strains were sent to CDC for serotyping but could not be typed using the Quellung reaction. Viral cell cultures of specimens from 70 students were negative for adenovirus (no cytopathic effect after 10 days' incubation). School health officials used campus-wide e-mail, posters, and the college newspaper to notify students, faculty, and staff about the outbreak and ways to reduce transmission. The messages instructed students to wash their hands frequently; to avoid sharing towels, drinking glasses, or other utensils; and to make an appointment with the student health service if they developed signs or symptoms of conjunctivitis. The student health service provided topical antibiotic therapy to students presenting with signs or symptoms of conjunctivitis. In addition, bottles of alcohol-based anti-septic gel were provided to all undergraduate students along with an information sheet that provided instructions on proper hand antisepsis using the gel. Local primary-care physicians and ophthalmologists were notified about the outbreak and asked to obtain cultures from patients presenting with conjunctivitis and to report cases to the investigating team. A student health service listserv was used to notify other student health services in the United States about the outbreak. The college's winter term ended March 14, 2002, and students will be departing for spring break. As of March 13, the student health service was still reporting new cases of conjunctivitis. Reported by: JH Turco, MD, JH Pryor, MA, YY Baumgartner, MBA, Dartmouth College Health Svc; ME Zegans, MD, P Sanchez, Dartmouth Medical School; A Bashir, MD, JD Schwertzman, MD, Dartmouth Hitchcock Medical Center, Hanover; J Puffer, JT Montero, MD, New Hampshire Dept of Health and Human Svcs. S Sodha, J Elliott, PhD, CG Whitney, MD, Div of Bacterial and Mycotic Diseases, National Center for Infectious Diseases; M Martin, MD, EIS Officer, CDC. Editorial Note:This report describes an outbreak of conjunctivitis attributed to an unusual nontypeable strain of S. pneumoniae. Outbreaks caused by nontypeable pneumococci have been reported previously (1,2). Person-to-person transmission of the outbreak strain may be occurring from eye secretions, respiratory droplets, or hands. Prevention messages were intended to reduce contact that would encourage transmission. The use of alcohol-based antiseptic gel improves hand hygiene in the hospital setting (3); however, its benefit in the setting of a community outbreak is unknown. Some of the college's students will have left campus for spring break with active S. pneumoniae conjunctivitis. Others will have left during the incubation period of the infection or might be asymptomatic carriers of the epidemic strain of S. pneumoniae. Some students will be traveling to popular college student vacation spots. Crowding and limited access to handwashing facilities might result in further transmission of this highly infectious strain of S. pneumoniae. Students who develop symptoms of conjunctivitis (e.g., red eyes, crusting of eyes in the morning, or increased eye discharge) should seek medical care. Health-care providers who see college students with conjunctivitis should suspect a bacterial etiology, and consider obtaining a culture of eye secretions, treating with a topical antibiotic, and ensuring that standard infection-control practices are followed (4). Outbreaks of conjunctivitis attributed to S. pneumoniae should be reported to state health departments, and state health department personnel should notify CDC, telephone (404) 639-2215. AcknowledgementsThis report is based on data contributed by J Greenblatt, MD, S Macrae, MS, M Sweeney, MS, New Hampshire Dept of Health and Human Svcs. M Richardson, MS, C Bradley, S Power, D Fisk, D Cook, S Robinson, L Clancy, J Karlen, C Henderson, and clinicians and staff, Dartmouth College Health Svc; Nathan Smith Pre-Med Society, Dartmouth College, Hanover, New Hampshire. A Schuchat, MD, RR Facklam, PhD, DM Jackson, MS, Div of Bacterial and Mycotic Diseases; N Khetsuriani, MD, U Parashar, MPH, DD Erdman, DrPH, Div of Viral and Rickettsial Diseases; SK Fridkin, MD, Div of Healthcare Quality Promotion, National Center for Infectious Diseases, CDC. References
Figure 1 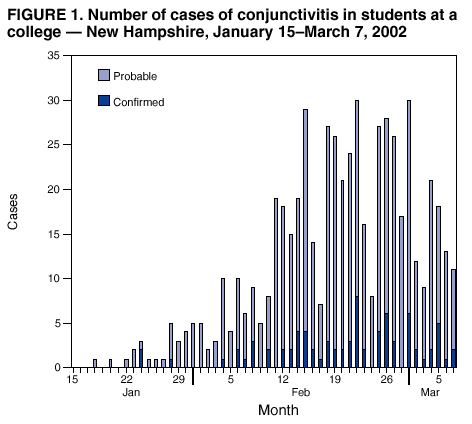 Return to top. Figure 2 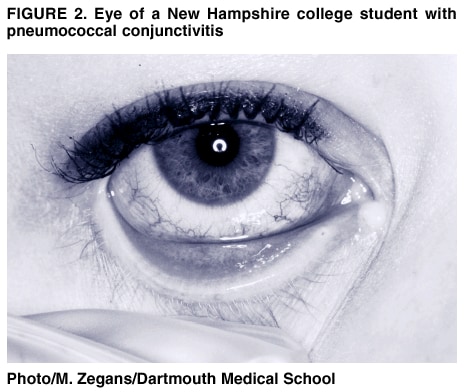 Return to top.
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 3/14/2002 |
|||||||||
This page last reviewed 3/14/2002
|