|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
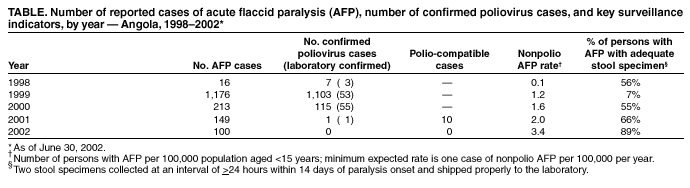
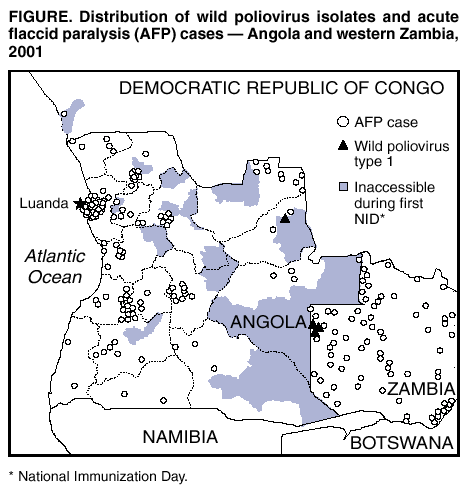
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Progress Toward Poliomyelitis Eradication --- Angola, January 1998--June 2002Since the World Health Assembly resolved in 1988 to eradicate poliomyelitis, the estimated number of polio cases worldwide has declined >99% (1). Angola began polio eradication activities in 1996. Although polio eradication efforts have been hampered by the country's 27-year-long civil war, both the incidence of polio cases and the geographic circulation of poliovirus in Angola have decreased substantially (2). The cessation of hostilities on April 4, 2002, presents a new opportunity to reach populations that had been inaccessible and undervaccinated previously. This report summarizes progress made during January 1998--June 2002 and highlights the remaining challenges to eradicating polio in Angola. Routine VaccinationDuring 1990--2000, the reported national coverage of children aged 0--11 months with 3 doses of oral polio virus vaccine (OPV3) ranged from 21% to 45%. The 2001 Multiple Indicator Cluster Survey conducted by the Angolan National Institute of Statistics estimated OPV3 coverage at 63% among children aged 12--23 months. Supplementary Immunization ActivitiesSince 1996, annual National Immunization Days* (NIDs) have been conducted in Angola targeting approximately 4 million children aged <5 years. Two annual rounds were held during 1996--1998, and three annual rounds have been held since 1999. Although access to children in conflict areas was limited as a result of the war, Angolan Ministry of Health (MoH) reports indicate that access improved during 1999--2001; the number of municipalities not accessible during all three NID rounds decreased from 51 (31%) of 164 in 1999 to 24 (15%) in 2000 and to 10 (6%) in 2001. Beginning in June 2000, a national house-to-house vaccination strategy was implemented to locate and vaccinate children. Extra rounds of Sub-National Immunization Days† (SNIDs) were organized in high-risk areas in 2001 and 2002. The May 2002 SNIDs targeted 40 municipalities with an estimated 2.6 million children aged <5 years. The number of children reported vaccinated was 3.1 million, which included children living in 28 camps for internally displaced persons (IDPs) and in five quartering areas for former combatants and their families. Acute Flaccid Paralysis SurveillanceAngola established surveillance for acute flaccid paralysis (AFP) in 1997. The quality of AFP surveillance is evaluated by two key World Health Organization (WHO)--established indicators: sensitivity of reporting (target: nonpolio AFP rate of >1 case per 100,000 children aged <15 years per year) and completeness of specimen collection (target: two adequate stool specimens from >80% of all persons with AFP). Angola achieved a nonpolio AFP rate of 1.2 in 1999 (Table). As of June 30, 2002, the projected annual nonpolio AFP rate was 3.4, with 17 of 18 provinces reporting AFP cases. The proportion of persons with AFP from which two adequate stool specimens were collected was 66% during 2001 and 89% during January--June 2002. The nonpolio enterovirus isolation rate (target: >10%), a marker for laboratory performance and the integrity of the reverse cold chain for specimen transport, was 14% in 2000 and 22% in 2002. In 2001, Angola shifted from a clinical to a virological AFP case classification system (i.e., only AFP cases with wild poliovirus isolates are classified as confirmed polio); AFP cases in which paralytic polio cannot be ruled out reliably are classified as polio-compatible. In 2001, a total of 10 AFP cases from five provinces were classified as polio-compatible. As of June 30, 2002, no AFP cases had been classified as polio-compatible. Incidence of PolioDuring 1999, a polio outbreak in Angola affected 1,103 children, with 53 cases confirmed virologically and 113 reported deaths (3,4). The outbreak was caused primarily by wild poliovirus type 3 (P3), although wild poliovirus type 1 (P1) also was isolated. In 2000, Angola reported 55 polio cases, including 52 cases with isolation of P1 and three cases with isolation of P3. In 2001, one polio case with isolation of P1 was reported from Angola (Figure). During 2000, an outbreak of polio with a high case-fatality rate (56 cases, 17 deaths) occurred on the Cape Verde Islands (5). Genetic sequence analysis showed that the isolated P1 was imported from Angola. During December 2001--February 2002, five polio cases with isolation of P3 were detected among Angolan refugees in western Zambia. Genetic sequence analysis showed that these isolates were related to wild poliovirus strains last isolated in Angola and the Democratic Republic of Congo (DRC) during 2000. Reported by: Angolan Ministry of Health, Country Office of the World Health Organization, Luanda, Angola. Regional Office of the World Health Organization for Africa, Harare, Zimbabwe. Vaccines and Biologicals Dept, World Health Organization, Geneva, Switzerland. Div of Viral and Rickettsial Diseases, National Center for Infectious Diseases; Global Immunization Div, National Immunization Program, CDC. Editorial Note:Although armed conflict in Angola posed many challenges to surveillance and vaccination activities, data during January 1999--June 2002 indicate substantial progress toward interruption of wild poliovirus transmission. Following the 1999 outbreak, MoH, WHO, and the United Nations Children's Fund (UNICEF) have increased the number of staff working on polio eradication. As a result, the percentage of adequate stool specimens collected increased during the last quarter of 2001 to >80%, and Angola has met WHO-recommended standards of surveillance quality through June 2002. The cessation of hostilities in Angola has improved access to areas never before covered by supplementary immunization activities or AFP surveillance. Emergency assistance is needed for approximately 800,000 persons living in areas that became accessible recently and for approximately 1.9 million persons in areas that had been accessible previously. An estimated 250,000 family members have gathered around 37 quartering areas for former combatants, and 300,000 IDPs are living temporarily in transit centers. Approximately 80,000 of an estimated 470,000 Angolan refugees now living in neighboring countries are expected to return to Angola (United Nations Office for the Coordination of Humanitarian Affairs [OCHA], unpublished data, 2002). The recent isolation of wild poliovirus from five unvaccinated children of Angolan refugees in western Zambia highlights the potential for circulation of wild poliovirus in areas where children of refugees and IDP groups might congregate. Undervaccinated children in mobile high-risk groups should be targeted for vaccination. Angola implemented NID rounds in June, July, and August 2002, synchronized with rounds conducted in the DRC, Republic of Congo, Gabon, Zambia, Namibia, and São Tomé and Principe. An AFP surveillance review is scheduled for October 2002, followed by the first meeting of an international technical advisory group for polio eradication in Angola. Future plans include expansion of AFP surveillance and vaccination activities to include newly accessible areas and populations. Interruption of wild poliovirus transmission in Angola will require that the overall security situation remain stable, existing shortfalls in financial and human resources are met, surveillance quality is improved further, and children in high-risk groups are vaccinated successfully. Close collaboration between the local government and its global partners§ has been critical in sustaining eradication "activities in Angola and will continue to be essential. References
* Nationwide mass campaigns over a short period (days to weeks) in which 2 doses of OPV are administered to all children (usually aged <5 years), regardless of vaccination history, with an interval of 4--6 weeks between doses.
|
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services. |
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices.
Page converted: 8/29/2002
|
|
|||||
|
HOME |
ABOUT MMWR |
MMWR SEARCH |
DOWNLOADS |
RSS
|
CONTACT
|
|||||
|
|
|||||
|
This page last reviewed 8/29/2002