|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
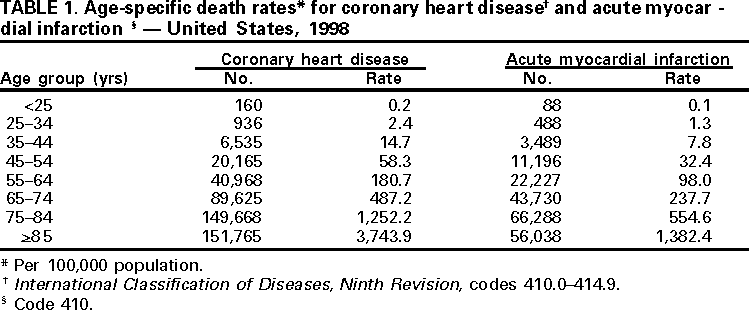
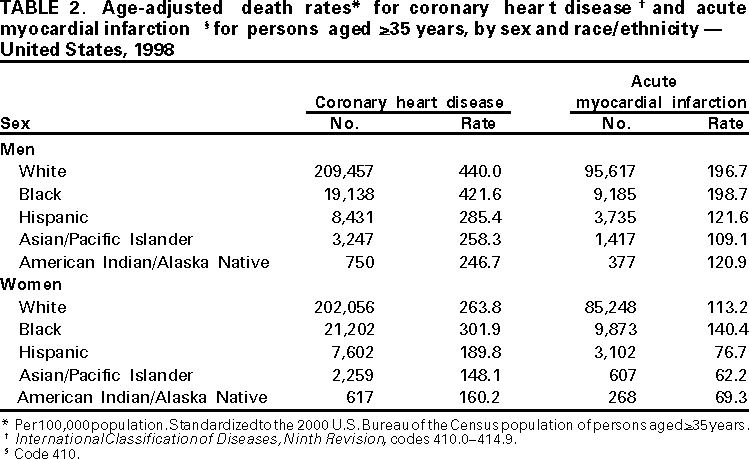
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Mortality From Coronary Heart Disease and Acute Myocardial Infarction --- United States, 1998Despite improved clinical care, heightened public awareness, and widespread use of health innovations, coronary heart disease (CHD) remains the leading cause of death in the United States (1,2), and the decline in rates from CHD that began during the 1960s slowed during the 1990s (3). This report provides national and state-specific death rates for CHD and for acute myocardial infarction (AMI). During 2001, approximately 1.1 million persons are expected to have a CHD event (1). Prevention remains the key strategy for reducing CHD mortality. National and state mortality statistics are based on information from death certificates filed in state vital statistics offices and are compiled by CDC's National Center for Health Statistics (4). Demographics (e.g., age and race/ethnicity) listed on death certificates are reported by funeral directors or provided by family members of the decedent. CHD deaths are those in which the underlying cause of death listed on the death certificate by a physician, medical examiner, or coroner is International Classification of Diseases, Ninth Revision, codes 410.0--414.9 (5). CHD includes AMI (410), other acute and subacute forms of ischemic heart disease (411), old myocardial infarction (412), angina pectoris (413), and other forms of chronic ischemic heart disease (414.0--414.9). Populations at risk are defined on the basis of U.S. Bureau of Census estimates of resident populations. Age-adjusted estimates are standardized to the 2000 U.S. population. Because only 0.2% of CHD deaths and 0.3% of AMI deaths occur among persons aged <35 years, the age-adjusted death rates have been limited to persons aged >35 years. The annual percentage change in U.S. death rates for CHD during 1950--1959, 1960--1969, 1970--1979, 1980--1989, and 1990--1997 was 2.1, 0.2, --3.1, --3.3, and --2.7, respectively (3). During 1998, CHD was reported as the underlying cause of 459,841 deaths; 203,551 (44%) were attributed to AMI. During 1998, age-specific death rates per 100,000 persons increased among successive age groups for CHD and AMI. Among persons aged >85 years, the 1998 CHD death rate was 3743.9, which was three times higher than the rate among persons aged 75--84 years (1252.2), seven times higher than among persons aged 65--74 years (487.2), and 21 times higher than among persons aged 55--64 years (180.7) (Table 1). The age-adjusted death rate among persons aged >35 years was higher among men than women (222.4 versus 135.8 per 100,000 for CHD and 99.7 versus 58.8 per 100,000 for AMI, respectively). CHD death rates were highest among white men (440.0) and second highest among black men (421.6). AMI deaths were similar among both groups (196.7 and 198.7 for white and black men, respectively) (Table 2). Compared with white men, American Indian/Alaska Native men and Asian/Pacific Islander men had much lower death rates for CHD (246.7 and 258.3, respectively) and AMI (120.9 and 109.1, respectively). Black women had the highest death rates for CHD (301.9) and AMI (140.4), followed by white (263.8 and 113.2 for CHD and AMI, respectively), American Indian/Alaska Native, (160.2 and 69.3 for CHD and AMI, respectively) and Asian/Pacific Islander (148.1 and 62.2 for CHD and AMI, respectively) women (Table 2). Compared with black and white men and women, Hispanics had lower death rates for CHD (285.4 and 189.8 for men and women, respectively) and AMI (121.6 and 76.7 for men and women, respectively) (Table 2). State variations in age-adjusted death rates for CHD and AMI ranged from 208.1 (New Mexico) to 440.6 (New York) for CHD and from 80.5 (New Mexico) to 252.6 (Arkansas) for AMI (Table 3). Reported by: Cardiovascular Health Studies Br, Div of Adult and Community Health, National Center for Chronic Disease Prevention and Health Promotion; and EIS officers, CDC. Editorial Note:An estimated 12 million persons in the United States have CHD (3). Of the 1.1 million persons who are expected to have a CHD event during 2001, approximately 650,000 will be first events and 450,000 will be recurrences. Each year, approximately 220,000 fatal CHD events occur suddenly among unhospitalized persons (1). The slowing decline in CHD death rates may be explained by the pattern of CHD risk factors reported during the 1990s (3). Minimal, if any, improvement has occurred in preventive behaviors (e.g., adequate physical activity, cessation of smoking, and the control of high blood pressure) (3). In addition, an increase has been reported in caloric consumption and the prevalence of obesity and diabetes (3). Factors that may have contributed to the racial/ethnic differences, particularly those between black and white women, include differences in CHD risk factors, case fatality rates, medical care, socioeconomic status, and state of residence (6). The findings in this report are subject to at least two limitations. First, the data are subject to misclassification of race/ethnicity in the population census and on death certificates, which may result in undercounting of deaths among American Indians/Alaska Natives, Asians/Pacific Islanders, and Hispanics and overcounting of deaths among black and white populations (7). Second, there is no medical record verification of death certificate data on multiple-cause mortality records. The reliability and accuracy of underlying cause depends on the certifier of each death and the state and national nosologists who determine the codes and the underlying causes. CDC funds 25 state-based cardiovascular health programs designed to prevent the first heart attack and promote a greater decline in death and disability from CHD. Measures intended to prevent a first AMI promote policy changes (e.g., health-care providers implementing American Heart Association AMI prevention guidelines) and behavioral changes that affect cardiovascular-related risk factors (e.g., high blood pressure, high cholesterol, cigarette smoking, physical inactivity, and poor nutrition). Myocardial damage, disability, and death can be forestalled if affected persons recognize AMI warning symptoms and reach medical care quickly (8). To reduce delays in receiving treatment (8) and preventing disability following a CHD event, emergency medical care often can be obtained rapidly by telephoning 911. Other interventions consist of therapeutic measures to minimize the risk for a second heart attack and subsequent heart failure (9), education to promote physician adherence to clinical practice guidelines, and recommendations for the appropriate treatment of CHD patients. References
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 2/15/2001 |
|||||||||
This page last reviewed 5/2/01
|