|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
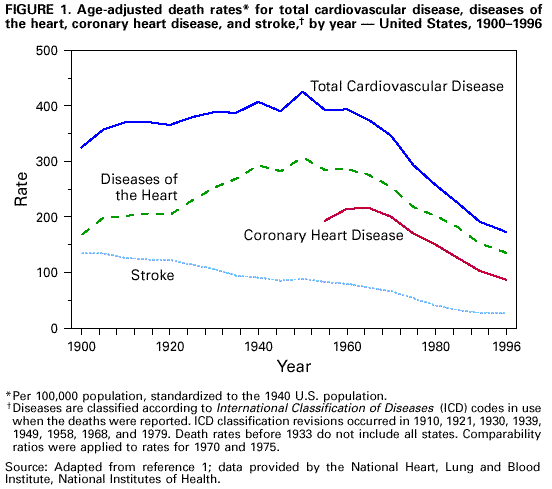
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Achievements in Public Health, 1900-1999: Decline in Deaths from Heart Disease and Stroke -- United States, 1900-1999Heart disease has been the leading cause of death in the United States since 1921, and stroke has been the third leading cause since 1938 (1); together they account for approximately 40% of all deaths. Since 1950, age-adjusted death rates from cardiovascular disease (CVD) have declined 60%, representing one of the most important public health achievements of the 20th century. This report summarizes the temporal trends in CVD, advances in the understanding of risk factors for CVD, development of prevention interventions to reduce these risks, and improvements in therapy for persons who develop CVD. Decline in CVD Death Rates Age-adjusted death rates per 100,000 persons (standardized to the 1940 U.S. population) for diseases of the heart (i.e., coronary heart disease, hypertensive heart disease, and rheumatic heart disease) have decreased from a peak of 307.4 in 1950 to 134.6 in 1996, an overall decline of 56% (1) (Figure 1). Age-adjusted death rates for coronary heart disease (the major form of CVD contributing to mortality) continued to increase into the 1960s, then declined. In 1996, 621,000 fewer deaths occurred from coronary heart disease than would have been expected had the rate remained at its 1963 peak (1). Age-adjusted death rates for stroke have declined steadily since the beginning of the century. Since 1950, stroke rates have declined 70%, from 88.8 in 1950 to 26.5 in 1996. Total age-adjusted CVD death rates have declined 60% since 1950 and accounted for approximately 73% of the decline in all causes of deaths during the same period (1). Disease Epidemiology Intensive investigation into the CVD epidemic largely began in the 1940s following World War II, although causal hypotheses about CVD and recognition of geographic differences in disease rates occurred earlier (2-4). Landmark epidemiologic investigations, including the cross-country comparisons of Ancel Keys (5) (see box) and the Framingham Heart Study (6), established the major risk factors of high blood cholesterol, high blood pressure, and smoking and dietary factors (particularly dietary cholesterol, fat, and sodium). The risk factor concept--that particular biologic, lifestyle, and social conditions were associated with increased risk for disease--developed out of CVD epidemiology (3,4). In addition to the major risk factors (i.e., high blood pressure, high blood cholesterol, and smoking), other important factors include socioeconomic status, obesity, and physical inactivity (7). Striking regional differences were noted particularly for stroke mortality, with the highest rates observed in the southeastern United States (1). Cross-national and cross-cultural studies highlighted the importance of social, cultural, and environmental factors in the development of CVD. Coronary heart disease and stroke, the two major causes of CVD-related mortality, are not influenced to the same degree by the recognized risk factors. For example, elevated blood cholesterol is a major risk factor for coronary heart disease, and hypertension is the major risk factor for stroke. Physical activity, smoking cessation, and a healthy diet, which can lower the risk for heart disease, also can help lower the risk for stroke (8). Advances in Prevention Early intervention studies in the 1960s sought to establish whether lowering risk factor levels would reduce risk for CVD (2-4). During the 1970s and 1980s, along with numerous clinical trials demonstrating the efficacy of antihypertensive and lipid-lowering drugs, community trials sought to reduce risk at the community level (9). Public health interventions to reduce CVD have benefitted from a combination of the "high risk" approach--aimed at persons with increased risk for CVD--and the population-wide approach--aimed at lowering risk for the entire community (10). National programs that combine these complementary approaches and that are aimed at health-care providers, patients, and the general public include the National High Blood Pressure Education Program (11), initiated in 1972, and the National Cholesterol Education Program, initiated in 1985 (12). Although earlier CDC community demonstration projects focused on cardiovascular health (9), CDC established its National Center for Chronic Disease Prevention and Health Promotion in 1989, with a high priority of promoting cardiovascular health. Factors Contributing to the Decline in CVD Deaths Reasons for the declines in heart disease and stroke may vary by period and across region or socioeconomic groups (e.g., age, sex, and racial/ethnic groups). Prevention efforts and improvements in early detection, treatment, and care have resulted in a number of beneficial trends (Table 1), which may have contributed to declines in heart disease and stroke. These trends include
Challenges for the 21st Century Despite remarkable progress, heart disease and stroke remain leading causes of disability and death. Estimated costs for morbidity and mortality from CVD, including health expenditures and lost productivity, are expected to be $286.5 billion in 1999 (18). In addition, the overall declines in heart disease and stroke mortality mask important differences in rates of decline by race/ethnicity, sex, socioeconomic status, and geographic region. During 1985-1996, for example, heart disease age-adjusted mortality declined 29% among white men, but only 10% among American Indian/ Alaskan Native women (13). Persons of lower socioeconomic status have higher mortality, morbidity, and risk factor levels for heart disease and stroke than persons of higher socioeconomic status (13,19). In addition, the social class gap in heart disease deaths may be increasing as the rates of heart disease decline faster among higher social classes (19). Geographically, declines in heart disease deaths did not occur at the same time for all communities. Areas with poorer socioeconomic profiles were more likely to experience a later onset of the decline of heart disease (19). Public health programs at the state level for heart disease and stroke have been limited. In fiscal year 1999, through a new program, CDC funded 11 states with the highest CVD mortality rates to plan, develop, and implement state-based efforts for CVD prevention. In addition to activities such as surveillance, these programs will emphasize policy and environmental interventions, both social and physical, aimed at sustaining positive health behavior change. Although many trends have been positive, trends for some important indicators have not improved substantially, have leveled off, or are reversing. For example, approximately 70% of persons with hypertension do not have the condition controlled at levels below 140/90 mm Hg, and death rates for stroke have not declined in recent years (1,11,13). Heart failure has emerged as a health concern for older adults (20), and adults who survive a myocardial infarction or other hypertension-related diseases remain at increased risk for heart failure. In addition, the prevalence of obesity has increased among both children and adults in the United States (13). Major public health challenges for the 21st century include
Reported by: Cardiovascular Health Br, Div of Adult and Community Health, National Center for Chronic Disease Prevention and Health Promotion, CDC. References
TABLE 1. Estimated change in risk factors and correlates for heart disease and stroke, by selected characteristics -- United States =================================================================================================================================== Characteristic Baseline year Baseline estimate Follow-up year Follow-up estimate -------------------------------------------------------------------------------------------------------------------------------- Adults aged 20-74 years with hypertension*+ 1960-1962 37% 1988-1994 23% Persons with hypertension who are taking action to control their blood pressure (e.g., medication, diet, reducing salt intake, and exercise) 1985 79% 1990 90% Persons with hypertension whose blood pressure is controlled 1976-1980 11% 1988-1991 29% Adults aged 20-74 years with high blood cholesterol+& 1960-1962 32% 1988-1994 19% Mean serum cholesterol levels mg/dL of adults aged >=18 years+ 1960-1962 220 1988-1994 203 Adults aged >=18 years who are current smokers+ 1965 42% 1995 25% Persons who are overweight+@ 1960-1962 24% 1988-1994 35% Percentage of calories in the diet from fat** 1976-1980 36% 1988-1994 34% Percentage of calories in the diet from saturated fat** 1976-1980 13% 1988-1994 12% Number of physicians indicating cardiovascular diseases as their primary area of practice 1975 5,046 1996 14,304 -------------------------------------------------------------------------------------------------------------------------------- * Systolic pressure >=140 mm Hg, diastolic pressure >=90 mm Hg, or taking antihypertensive medication. + Estimate is age-adjusted to the 1940 U.S. population. & Serum cholesterol level >=240 mg/dL (6.2 mmol/L). @ Defined as a body mass index >=27.8 kg/m² among men and 27.2 kg/m² among women. ** Based on 1-day dietary recall. Source: References 11-14. ===================================================================================================================================
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 8/5/1999 |
|||||||||
This page last reviewed 5/2/01
|