Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail.
Overview of Syndromic Surveillance
What is Syndromic Surveillance?
Kelly J. Henning
New York City Department of Health and Mental Hygiene, New York, New York
Corresponding author: Kelly J. Henning, New York City Department of Health and Mental Hygiene, 125 Worth Street, CN-6, New York,
NY 10013. Telephone: 212-788-0234; Fax: 212-788-4473; E-mail: khenning@health.nyc.gov.
Abstract
Innovative electronic surveillance systems are being developed to improve early detection of outbreaks attributable to
biologic terrorism or other causes. A review of the rationale, goals, definitions, and realistic expectations for these surveillance systems is a crucial first step toward establishing a framework for further research and development in this area. This
commentary provides such a review for current syndromic surveillance systems.
Syndromic surveillance has been used for early detection of outbreaks, to follow the size, spread, and tempo of outbreaks,
to monitor disease trends, and to provide reassurance that an outbreak has not occurred. Syndromic surveillance systems seek
to use existing health data in real time to provide immediate analysis and feedback to those charged with investigation
and
follow-up of potential outbreaks. Optimal syndrome definitions for continuous monitoring and specific data sources best
suited to outbreak surveillance for specific diseases have not been determined. Broadly applicable signal-detection methodologies and response protocols that would maximize detection while preserving scant resources are being sought.
Stakeholders need to understand the advantages and limitations of syndromic surveillance systems. Syndromic
surveillancesystems might enhance collaboration among public health agencies, health-care providers, information-system
professionals, academic investigators, and industry. However, syndromic surveillance does not replace traditional public health surveillance, nor does it substitute for direct physician reporting of unusual or suspect cases of public health importance.
Introduction
The desire to expand and improve upon traditional methods of public health surveillance is not new. Even before the
2001 terrorist attacks on the United States and the subsequent anthrax outbreak, public health officials had begun to enhance detection of emerging infections and illnesses caused by biologic agents. A primary objective of a 1998 CDC plan was to develop programs for early detection and investigation of outbreaks
(1). CDC's 2000 strategic plan for biologic and
chemical preparedness called for early detection by integrating terrorism preparedness into existing systems and developing "new mechanisms for detecting, evaluating, and reporting suspicious events"
(2). Although the need for innovative
surveillance techniques had already been identified, the anthrax outbreak after
Bacillus anthracis spores were released through the mail
in 2001 (3) accelerated the implementation of syndromic surveillance systems across the United States. An overview of the location and scope of the earliest systems implemented before and after fall 2001 has been published
(4).
Goals and Rationale
Although syndromic surveillance was developed for early detection of a large-scale release of a biologic agent,
current surveillance goals reach beyond terrorism preparedness.
Medical-provider reporting remains critical for identifying
unusual disease clusters or sentinel cases. Nevertheless, syndromic surveillance might help determine the size, spread, and tempo of
an outbreak after it is detected (5), or provide reassurance that a large-scale outbreak is not occurring, particularly in times of enhanced surveillance (e.g., during a high-profile event). Finally, syndromic surveillance is beginning to be used to
monitor disease trends, which is increasingly possible as longitudinal data are obtained and syndrome definitions refined.
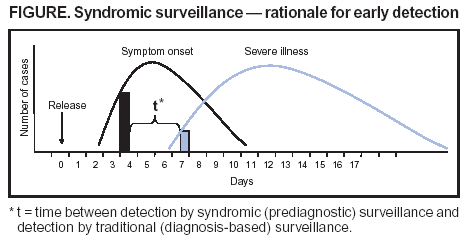
The fundamental objective of syndromic surveillance is to identify illness clusters early, before diagnoses are confirmed and reported to public health agencies, and to mobilize a rapid response, thereby reducing morbidity and mortality.
Epidemic curves for persons with earliest symptom onset and those with severe illness can be depicted graphically (Figure). The time between symptom onset for an increasing number of cases caused by deliberate release of a biologic agent and
subsequent patient visits to a health-care facility resulting in a definitive diagnosis is represented by
t. Syndromic surveillance aims to identify a threshold number of early symptomatic cases,
allowing detection of an outbreak t days earlier than
would conventional reporting of confirmed cases. The ability of syndromic surveillance to detect outbreaks earlier than
conventional surveillance methods depends on such factors as the size of the outbreak, the population dispersion of those affected, the data sources and syndrome definitions used, the criteria for investigating threshold alerts, and the health-care provider's ability
to detect and report unusual cases (6). CDC's framework for evaluating public health surveillance systems for early detection of outbreaks should be useful for comparing syndromic surveillance across jurisdictions and for evaluating system
performance (7).
Specific definitions for syndromic surveillance are lacking, and the name itself is imprecise. Certain programs
monitor surrogate data sources (e.g., over-the-counter prescription sales or school absenteeism), not specific disease
syndromes. Meanwhile, certain well-defined disease or clinical syndromes (e.g., hemolytic uremic syndrome or Kawasaki's syndrome) are not included in syndrome definitions, often leading to confusion about what "syndromic" surveillance actually monitors. Diverse names used to describe public health surveillance systems for early outbreak detection include
early warning systems (8,9);
prodrome surveillance (10);
outbreak detection systems
(11);
information system-based sentinel surveillance
(12);
biosurveillance systems
(13--15);
health indicator surveillance
(16);and
symptom-based surveillance
(17).
However, syndromic surveillance is the term that has
persisted.
In defining syndromic surveillance, certain authors have emphasized the importance of monitoring the frequency of
illnesses with a specific set of clinical features
(18), a definition that does not account for nonclinical data sources. Others
have emphasized the importance of prediagnostic data to estimate a community's health status, particularly by relying on
outpatient visits (19).Inherent in the use of existing electronic data to describe prediagnostic health indicators is the central role of timeliness in the analysis, detection, and investigation of alerts. Perhaps the most comprehensive definition to date, and
likely the one to be broadly adopted, is provided by CDC's evaluation framework, which describes syndromic surveillance as
"an investigational approach where health department staff, assisted by automated data acquisition and generation of
statistical alerts, monitor disease indicators in real-time or near real-time to detect outbreaks of disease earlier than would otherwise be possible with traditional public health methods"
(7).
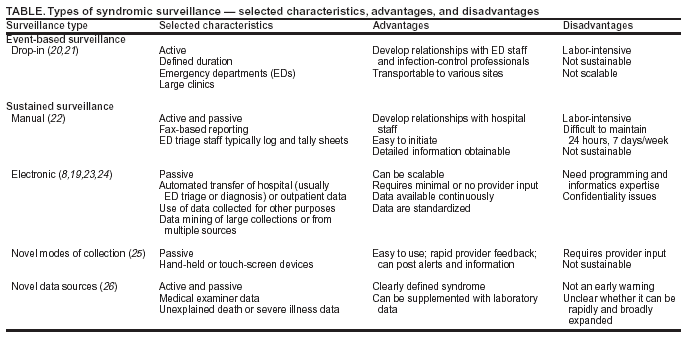
Syndromic surveillance systems vary by their planned duration and their manner of acquiring data (Table).
Short-duration, event-based systems are usually used to provide enhanced surveillance around a discrete event (e.g., the Olympic Games or a national political convention) (20,23). Historically, these short-term syndromic surveillance projects, sometimes termed drop-in surveillance, have required medical providers or others to collect nonroutine information
(20). More recent event-based surveillance systems have
relied on rapid implementation of electronically transferred data
(23). Manual data entry, which occurred after September 11, 2001, in 15 New York City emergency departments (EDs), is difficult to sustain (21). Using pre-existing health data for syndromic surveillance offers immediate accessibility and poses limited burden to providers and health-care institutions.
Categorizing symptoms and diagnoses into syndromes is a fundamental component of syndromic surveillance systems
that use clinical data sets. Although the majority of investigators have devised broad categories aimed at early detection of
biologic terrorism, validation of syndrome definitions is only beginning. Respiratory, gastrointestinal, rash, neurologic and sepsis syndromes have been monitored consistently
(19,22). Because numerous ED and outpatient settings have International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) data available electronically, ICD-9-CM
codes have been used to categorize syndromes. To facilitate comparability between surveillance systems, a CDC working
group published lists of candidate syndrome groups based on ICD-9-CM codes
(27). The usefulness of ICD-9-CM codes
compared with other data streams, particularly with regard to the data's timeliness, requires evaluation by each surveillance program.
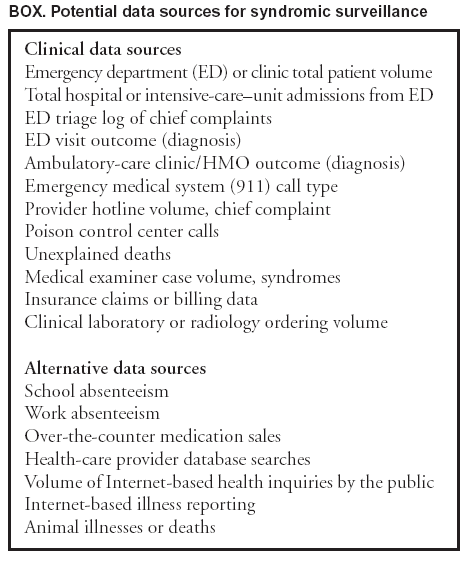
Syndromic surveillance focuses on the early symptom (prodrome) period before clinical or laboratory confirmation of
a particular disease and uses both clinical and alternative data sources (Box). Strictly defined, syndromic surveillance
gathers information about patients' symptoms (e.g., cough, fever, or shortness of breath) during the early phases of illness. However, in practice, certain syndromic surveillance systems collect surrogate data indicating early illness (e.g., school or work absenteeism data or veterinary data such as unexpected avian deaths or other potential precursors of human
illness). Alternative data sources have potential problems, including a presumed low specificity for syndromes of interest, high probability of influence by factors unrelated to personal health (e.g., weather or holidays), and difficulty in retracing data aberrations to individual patients. Despite these qualifiers, the optimal system might be one that integrates data from multiple sources, potentially increasing investigators' confidence in the relevance of an alert from any single data source.
Analytic Methods for Signal Detection
The analytic challenge in using syndromic surveillance for outbreak detection is to identify a signal corresponding to
an outbreak or cluster amid substantial "background noise" in the data. Syndromic surveillance systems use an array of aberration-detection methods to identify increases in syndromes above predetermined thresholds. However, signal-detection methods have not yet been standardized. Temporal and spatio-temporal methods have been used to assess day-to-day and day and
place variability of data from an expected baseline
(27,28).
Response Protocols
Response protocols for investigating syndromic surveillance alerts are under development by multiple programs. Obstacles
to effective, efficient follow-up include the difficulty of predicting how well the syndromes themselves correlate with target
diseases under surveillance; the extremely low positive predictive value of any given signal based on the high level of system sensitivity; and investigators' relative lack of experience with syndromic surveillance under real-world conditions
(30).
Programmatic requirements for effective signal response (e.g., documented procedures; staff with appropriate expertise;
24-hour/day, 7-day/week analysis and response; and plans for information dissemination) are complex. Certain circumstances surrounding an alert might prompt rapider investigation, including clustering of cases by location; severe symptoms; unexplained deaths; sudden, substantial case numbers; simultaneous alerts from multiple data sources; or restriction of an alert to a particular population (e.g., age group or sex)
(31). Diagnostic confirmation is a paramount step in investigating
alerts, particularly given the nonspecific nature of certain syndrome categories. Developing protocols to address alerts from data sources in which individual cases are unidentifiable (e.g., over-the-counter medication sales) is particularly challenging.
Perspectives and Challenges
Distinguishing those points on which multiple investigators agree from those that are less well-delineated might be helpful in defining realistic expectations for syndromic surveillance. Investigators usually agree on the following:
Syndromic surveillance is being used in numerous states and localities to detect a potential large-scale biologic
attack.
Pre-existing electronic health data will likely become
increasingly available, thereby enhancing system development.
Syndromic surveillance does not replace traditional public health surveillance.
Syndromic surveillance is unlikely to detect an individual case of a particular illness.
Syndromic surveillance cannot replace the critical contribution of physicians in early detection and reporting of
unusual diseases and events.
Although syndromic surveillance's ability to detect a
terrorism-related outbreak earlier than traditional
surveillance remains unknown, it will likely be useful for defining the scope of an outbreak, providing reassurance that a large-scale outbreak has not occurred, and conducting surveillance of noninfectious health problems (e.g., monitoring nicotine replacement therapy sales following tobacco-tax increases). However, integral components of syndromic surveillance require additional research and evaluation, including the
following:
clarifying the use of simulation data sets to test systems; and
advancing the debate regarding resource commitment for syndromic versus traditional surveillance.
On a broader policy level, defining the role of academic partners in bridging any potential analytic gaps, defining the
role and scope of a national syndromic data repository, and developing policy for integrating laboratory testing and laboratory information systems with syndromic surveillance are on the horizon.
Acknowledgments
Farzad Mostashari, Don Weiss, Rick Heffernan, and other members of the New York City Department of Health and Mental Hygiene syndromic surveillance team provided data and program information.
References
CDC. Preventing emerging infectious diseases: a strategy for the
21st century. Atlanta, GA: US Department of Health and Human Services,
1998. Available at http://www.cdc.gov/ncidod/emergplan/index.htm.
Wagner MM, Tsui F-C, Espino JU, et al. The emerging science of very early detection of disease outbreaks. J Public Health Manag Pract
2001;7:50--8.
Brinsfield KH, Gunn JE, Barry MA, McKenna V, Syer KS, Sulis C. Using volume-based surveillance for an outbreak early warning
system [Abstract]. Acad Emerg Med 2001;8:492.
Mostashari F, Karpati A. Towards a theoretical (and practical) framework for prodromic surveillance [Abstract]. International Conference
on Emerging Infectious Diseases, Atlanta, GA, March 24--27, 2002.
Stern L, Lightfoot D. Automated outbreak detection: a quantitative retrospective analysis. Epidemiol Infect 1999;122:103--10.
Lober WB, Karras BT, Wagner MM, et al. Roundtable on bioterrorism detection: information systems-based surveillance. J Am Med Inform
Assoc 2002;9:105--15.
Cochrane DH, Allegra JR, Rothman J. Comparison of physician's choice of charting template to ICD-9 codes for biosurveillance using
an emergency department electronic medical records database
[Abstract]. Acad Emerg Med 2003;10:525.
Olson KL, Mandl K. Geocoding patient addresses for biosurveillance [Abstract]. Proc AMIA Symp 2002;1119.
Mocny M, Cochrane DG, Allegra JR, et al. A comparison of two methods of biosurveillance of respiratory disease in the emergency
department: chief complaint vs. ICD-9 diagnosis code [Abstract]. Acad Emerg Med 2003;10:513.
Pavlin JA, Mostashari F, Kortepter MG, et al. Innovative surveillance methods for rapid detection of disease outbreaks and bioterrorism:
results of an interagency workshop on health indicator surveillance. Am J Public Health 2003;93:1230--5.
Osaka K, Takahashi H, Ohyama T. Testing a symptom-based surveillance system at high-profile gatherings as a preparatory measure of
bioterrorism. Epidemiol Infect 2002;129:429--34.
Reingold A. If syndromic surveillance is the answer, what is the question? Biosecur Bioterror 2003;1:1--5.
US Department of Defense. Electronic Surveillance System for the Early Notification of Community-Based Epidemics (ESSENCE). Silver
Spring, MD: US Department of Defense, Global Emerging Infections Surveillance and Response System. Available at http://www.geis.ha.osd.mil/geis/surveillanceactivities/essense/essence.asp.
County of Los Angeles, Department of Health Services, Acute Communicable Disease Control. Special studies report 2000: Democratic
National Convention---bioterrorism syndromic surveillance. Los
Angeles: County of Los Angeles Department of Health Services, 2000. Available at
http://www.lapublichealth.org/acd/reports/spclrpts/spcrpt00/demonatconvtn00.pdf.
Begier EM, Sockwell D, Branch LM, et al. The National Capitol Region's emergency department syndromic surveillance system: do chief
complaint and discharge diagnosis yield different results? Emerg
Infect Dis 2003;9:393--6.
Gesteland PH, Wagner MM, Chapman WW, et al. Rapid deployment of an electronic disease surveillance system in the state of Utah for the
2002 Olympic Winter Games. Proc AMIA Symp 2002;285--289.
Lazarus R, Kleinman K, Sashevesky I, et al. Use of automated ambulatory-care encounter records for detection of acute illness
clusters, including potential bioterrorism events. Emerg Infect Dis 2002;8:753--60.
Zelicoff A, Brillman J, Forslund DW, et al. The rapid syndrome validation project. Proc AMIA Symp 2001;771--5.
Kluger MD, Sofair AN, Heye CJ, Meek JI, Sodhi RK, Hadler JL. Retrospective validation of a surveillance system from unexplained illness
and death: New Haven County, Connecticut. Am J Public Health 2001; 91:1214--9.
CDC. Syndrome definitions for diseases associated with critical bioterrorism-associated agents. Atlanta, GA: US Department of Health and
Human Services, CDC. Available at
http://www.bt.cdc.gov/surveillance/syndromedef/index.asp.
Hutwagner L, Thompson W, Seeman GM, Treadwell T. The bioterrorism preparedness and response early aberration reporting system (EARS).
J Urban Health 2003;80(2 Suppl 1):i89--96.
Das D, Weiss D, Mostashari F, et al. Enhanced drop-in syndromic surveillance in New York City following September 11, 2001. J Urban
Health 2003;80(2 Suppl 1):i76--88.
Duchin JS. Epidemiological response to syndromic surveillance signals. J Urban Health 2003;80(2 Suppl 1):i115--6.
Pavlin JA. Investigation of disease outbreaks detected by syndromic surveillance systems. J Urban Health 2003;80(2 Suppl 1):i107--4.
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services.References to non-CDC sites on the Internet are
provided as a service to MMWR readers and do not constitute or imply
endorsement of these organizations or their programs by CDC or the U.S.
Department of Health and Human Services. CDC is not responsible for the content
of pages found at these sites. URL addresses listed in MMWR were current as of
the date of publication.
Disclaimer
All MMWR HTML versions of articles are electronic conversions from ASCII text
into HTML. This conversion may have resulted in character translation or format errors in the HTML version.
Users should not rely on this HTML document, but are referred to the electronic PDF version and/or
the original MMWR paper copy for the official text, figures, and tables.
An original paper copy of this issue can be obtained from the Superintendent of Documents,
U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800.
Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to
mmwrq@cdc.gov.