|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
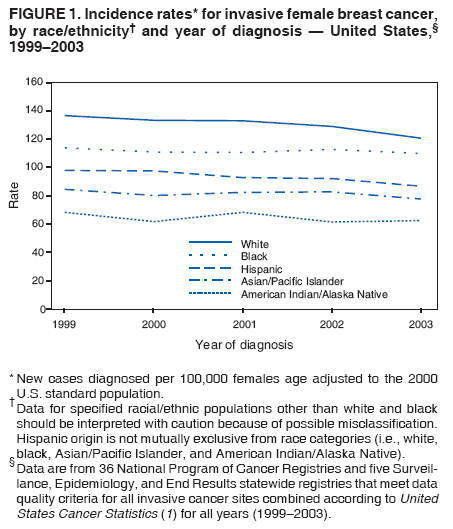
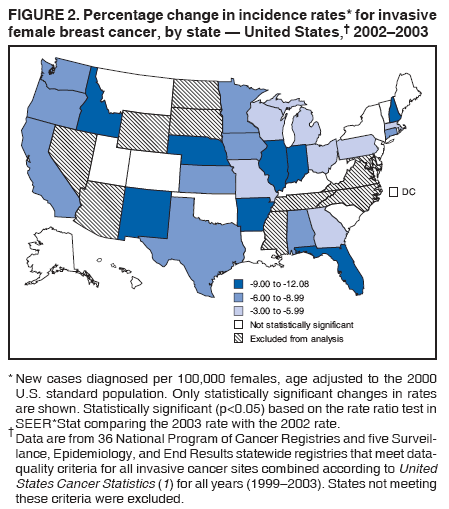
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Decline in Breast Cancer Incidence --- United States, 1999--2003Breast cancer is the most commonly diagnosed cancer among females in the United States (1). The 2006 Annual Report to the Nation on the Status of Cancer (2) described a stabilization in female breast cancer incidence rates during 2001--2003, ending increases that began in the 1980s, and a decline in the number of breast cancer cases diagnosed in 2003. In addition, researchers who used 1990--2003 data from the National Cancer Institute's (NCI's) Surveillance, Epidemiology, and End Results (SEER) program, representing approximately 14% of the U.S. population, reported a 7% decrease in invasive breast cancer rates from 2002 to 2003 (3). To further assess breast cancer annual incidence rates during 1999--2003, CDC analyzed data collected by CDC's National Program of Cancer Registries (NPCR) and the NCI SEER program. These combined data account for approximately 86% of the U.S. population (1). The results of this analysis indicated that age-adjusted incidence rates for invasive breast cancer decreased each year during 1999--2003, with the greatest decrease (6.1%) occurring from 2002 to 2003; women aged >50 years experienced a significant decrease during this period. Rates of in situ (i.e., noninvasive) breast cancer increased each year during 1999--2002 and then decreased from 2002 to 2003; women aged 50--79 years experienced a significant decrease during this period. Future studies should focus on determining potential causes for these decreases. The most recent data available from population-based cancer registries affiliated with NPCR or the SEER program were used in this analysis; new cases of cancer were those reported to CDC (NPCR) as of January 31, 2006, or NCI (SEER) as of November 1, 2005*; data from four statewide NPCR/SEER registries are indicated as reported to CDC as of January 31, 2006. Data were evaluated according to United States Cancer Statistics eligibility criteria,† which require >90% case ascertainment and an unduplication procedure within each registry to ensure that each cancer case is counted only once. Thirty-six NPCR and five SEER statewide registries met these criteria, representing 86.4% of the U.S. population for the years 1999--2003 (1). Because of the 86.4% population coverage, cancer rates derived from these data are considered to approximate actual incidence rates. A total of 1,043,480 diagnosed cases of breast cancer (in situ and invasive) among females were reported by these registries for the years 1999 to 2003 and used in this analysis. Annual incidence rates with confidence intervals were calculated. In situ and invasive breast cancer incidence rates were categorized by age at diagnosis; invasive cancer incidence rates were categorized by stage at diagnosis, race/ethnicity, and state of residence at diagnosis. Invasive breast cancer cases diagnosed during 1999--2000 were staged as localized, regional, or distant§ using the 1977 SEER summary staging system, and cases diagnosed during 2001--2003 were staged using the newer 2000 SEER summary staging system (2). Incidence rates, per 100,000 females, are age adjusted to the 2000 U.S. standard population. Population estimates used as denominators in the rate calculations are from the U.S. Census Bureau and modified by SEER to increase the accuracy of rates for the Hawaiian population (1). Statistically significant differences in rates between the years 2002 and 2003 were determined by using the rate ratio test in SEER*Stat (http://seer.cancer.gov/seerstat/index.html). Age-adjusted annual incidence rates for invasive breast cancer decreased each year from 1999 to 2003, with the greatest decrease in rates occurring from 2002 to 2003 (Table). The rate from 2002 to 2003 decreased 6.1%, with a significant decrease occurring for all women aged >50 years. The largest decrease (9.1%) occurred among women aged 60--69 years. For in situ cancers, rates increased each year from 1999 to 2002 and then decreased from 2002 to 2003, although the percentage decrease (2.7%) was smaller than that for invasive cancers (6.1%). Women aged 50--79 years experienced a significant decrease in incidence rates of in situ breast cancer from 2002 to 2003. Whites had the highest incidence rates of invasive female breast cancer among racial/ethnic populations during 1999--2003, and American Indians/Alaska Natives (AI/ANs) had the lowest rates (Figure 1). From 2002 to 2003, all racial/ethnic groups other than AI/ANs experienced a significant decrease in incidence rates (blacks, 2.7%; Hispanics, 5.8%; Asians/Pacific Islanders [A/PIs], 6.1%; and whites, 6.4%) (Figure 1). Rates of invasive breast cancer by stage at diagnosis declined during 1999--2003, with the largest decline (6.9%) (excluding unstaged cancer) occurring for localized cancer diagnosed from 2002 to 2003 (Table). Incidence rates of localized, regional, and unstaged female breast cancer decreased from 2002 to 2003; no significant change occurred in incidence rates of distant female breast cancer from 2002 to 2003. Twenty-four of the 41 states included in this analysis experienced a significant decrease in incidence rates from 2002 to 2003 (range: 3.5% in Pennsylvania to 12.1% in Indiana) (Figure 2). Rates decreased by >6% in 17 states, and no significant change occurred in 17 states. No significant increase occurred in any state included in the analysis, and no geographic pattern was observed. Reported by: SL Stewart, PhD, SA Sabatino, MD, SL Foster, MPH, LC Richardson, MD, Div of Cancer Prevention and Control, National Center for Chronic Disease Prevention and Health Promotion, CDC. Editorial Note:The findings in this report suggest that invasive female breast cancer rates have been decreasing in recent years, with a sharper decline occurring from 2002 to 2003. Furthermore, both in situ and invasive female breast cancer rates decreased from 2002 to 2003 across several age and stage groups and across most racial/ethnic populations. Decreases in 2003 occurred primarily among women aged >50 years, a finding consistent with those of other studies (3). The overall decrease from 2002 to 2003 occurred in 24 states. Decreases in rates of invasive female breast cancer from 2002 to 2003 were detected for all racial/ethnic populations analyzed except AI/ANs, although this population had the lowest overall incidence rate throughout the 5 years examined. In addition, the decrease in rates for black females was smaller than the decreases for other populations. Additional study is needed to determine possible reasons for these differences. From 2002 to 2003, significant decreases occurred in incidence rates for localized, regional, and unstaged breast cancer but not distant breast cancer; the reason for the absence of a decrease in distant breast cancer is unknown. The 9.5% decrease in unstaged breast cancer cases might have resulted, in part, from more complete data collection about stage of disease at diagnosis, resulting in fewer unstaged cases. This finding is consistent with a SEER data analysis that attributed improvements in tumor staging to the substantial decrease (13.5 per 100,000 in 1975 to 4.9 per 100,000 in 2003) in unknown staged cases observed over the duration of the SEER program (4). Several factors might affect breast cancer incidence and contribute to differences in rates over time and among populations. One such factor is hormone replacement therapy (HRT). Evidence collected, in part, through the National Institute of Health's Women's Health Initiative suggested an increased risk for invasive breast cancer among women who used HRT (5). The same year, the United States Preventive Services Task Force began recommending against the routine use of HRT (primarily combined estrogen and progestin regimens) for the prevention of chronic conditions, such as cardiovascular disease, in postmenopausal women.¶ The mechanism by which HRT use might result in an increase in breast cancer incidence is unknown. One study suggested that hormones play a role in the promotion of breast carcinogenesis, increasing the rate at which certain preexisting but undetectable cancers grow (6). A population-based study in California of women aged 50--74 years who were members of a health-care plan determined that age-adjusted rates of hormone therapy decreased 68% from 2001 to 2003; during the same period, breast cancer incidence rates decreased 10% among the health-plan members and 11% among all women in California (7). Because the breast cancer incidence rate began decreasing before 2002 (i.e., before the decrease in HRT use), other factors (e.g., differences in risk-factor prevalence, diet, and lifestyle) might be used to explain changes in breast cancer incidence rates. Mammography screening rates also might influence breast cancer incidence. A study in Connecticut that analyzed breast cancer incidence rates during 1943--2002 indicated that although incidence rates increased over time, they increased more quickly after initiation of mammography screening recommendations in the early 1980s, suggesting that more cases were being detected through screening (8). Data from another recent report indicate that the number of women aged >40 years who reported having received a mammogram within the preceding 2 years decreased significantly, by 2.4%, from 2000 to 2005 (9). Similar decreases were indicated by National Health Interview Survey data; in 2003, 69.5% of women aged >40 years had a mammogram within the preceding 2 years, compared with 70.4% in 2000.** Moreover, similar decreases in mammography screening rates were reported among persons enrolled in several types of health plans (i.e., commercial, Medicare, and Medicaid).†† The extent to which the decreases in mammography screening rates might affect breast cancer incidence is unknown. The findings in this report are subject to at least four limitations. First, although the data are the most geographically comprehensive data available, data are not included from all U.S. states; therefore, some populations might not be well represented. Second, data for A/PIs, AI/ANs, and Hispanic populations might be underestimated because of misclassification in medical records. Third, no additional information about tumor characteristics (e.g., estrogen receptor status), screening, and risk factors was available in the data set used in this analysis; therefore, the role of such factors in the observed changes cannot be assessed. Finally, reporting delays for cancers, such as breast cancer, that are commonly diagnosed in outpatient settings might result in numerous additional cases being added to totals from previous years. NPCR and SEER registries require 2--3 years to compile and report complete information about cancer cases in their respective CDC and NCI databases. Revised and updated information about cancer cases for previous years are submitted to CDC and NCI each year along with current statistics. However, a recent study demonstrated no statistically significant difference between breast cancer incidence in the delay-adjusted trend compared with the non--delay-adjusted trend (2). Therefore, the non--delay-adjusted rates and trends described in this report are not expected to vary significantly because of reporting delays. Analyses of future breast cancer incidence rates are needed to confirm the findings in this report. Studies should focus on examining possible causes for this decrease and analyzing 2004 data, which will become available in 2007. References
* Medical records are the primary source of cancer incidence data. Staff members at health-care facilities abstract cancer incidence data from patients' medical records, enter the data into the facility's own cancer registry, if it has one, and then send the data to the regional or state registry. Both NPCR and SEER registries collect data using uniform data items and codes as documented by the North American Association of Central Cancer Registries. Additional information on NPCR and SEER methodology is available at http://www.cdc.gov/cancer/npcr/npcrpdfs/uscs_2003_technical_notes.pdf. † Available at http://wonder.cdc.gov/wonder/help/cancer/uscs_2002_registry_eligibility_criteria.html. § Localized: cancer that is confined to the primary site. Regional: cancer that has spread directly beyond the primary site or to regional lymph nodes. Distant: cancer that has spread to other organs. ¶ United States Preventive Services Task Force. Recommendations and rationale: hormone replacement therapy for primary prevention of chronic conditions. Available at http://www.ahrq.gov/clinic/uspstf/uspspmho.htm. ** National Center for Health Statistics. Health, United States, 2005. Available at http://www.cdc.gov/nchs/data/hus/hus05.pdf#086. †† National Committee for Quality Assurance. The state of health care quality: industry trends and analysis. 2006. Available at http://www.ncqa.org/communications/sohc2006/sohc_2006.pdf.
Figure 1
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Date last reviewed: 6/7/2007 |
|||||||||
|