|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
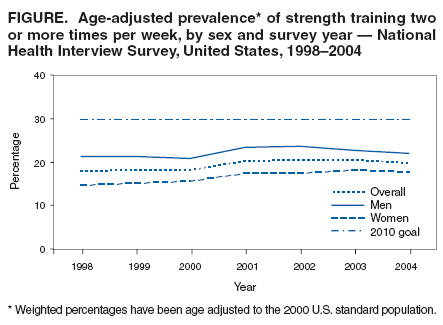
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Trends in Strength Training --- United States, 1998--2004Strength training is physical activity intended to increase muscle strength and mass. Adults who engage in strength training are less likely to experience loss of muscle mass (1), functional decline (2), and fall-related injuries than adults who do not strength train (3). Studies on strength-training interventions have indicated that inactive older adults who begin regular strength training achieve substantial strength gains within a few months (4). Because certain health benefits are linked to strength training, a national health objective for 2010 is to increase to 30% the proportion of adults who perform physical activities that enhance and maintain muscular strength and endurance on >2 days per week (objective 22-4) (5). This objective is also recommended by the American College of Sports Medicine (6). CDC analyzed 1998--2004 data from the National Health Interview Survey (NHIS) (7) to determine the annual prevalence of strength training among U.S. adults by age group and race/ethnicity. This report describes the results of that analysis, which demonstrated that although the national prevalence of strength training for U.S. adults increased slightly during 1998--2004, only 21.9% of men and 17.5% of women (age adjusted) in 2004 reported strength training two or more times per week. This is substantially lower than the national 2010 objective of 30% and underscores the need for additional programs to increase strength training among adults. NHIS consists of face-to-face interviews regarding health status, use of health-care services, and health behaviors of the U.S. civilian, noninstitutionalized population. Data on strength training were collected every year during 1998--2004. The sample size ranged from 30,801 (1999) to 33,326 (2001), and the response rate ranged from 69.6% (1999) to 74.3% (2002) (7). Respondents were asked to report the frequency with which they engaged in strength training by answering the following question: "How often do you do physical activities designed to strengthen your muscles, such as lifting weights or doing calisthenics?" The same question was asked each year and was available in Spanish for Spanish-speaking respondents beginning in 1999. Respondents were categorized as meeting the national strength training objective if they engaged in strength training two or more times per week (5). Prevalence estimates by age and sex were weighted to account for nonresponse and were age adjusted to the 2000 U.S. standard population (8). Statistical software was used to account for the complex sampling design of the survey. Pairwise comparisons were performed to calculate t statistics, and differences were considered significant at p<0.05. When multiple comparisons were made, the Bonferroni adjustment was used (p<0.05 / number of comparisons). Only significant differences are reported in the results. The age-adjusted prevalence of reported strength training two or more times per week among all respondents increased significantly, from 17.7% in 1998 to 19.6% in 2004. The difference between 1998 and 2004 was significant for women but not for men (Figure). In 2004, the age-adjusted prevalence of those who met recommended levels of strength training was significantly higher among men than women (21.9% versus 17.5%, respectively). In 2004, strength training was least prevalent among those aged >65 years (14.1% among men; 10.7% among women). Prevalence of strength training among men and women decreased significantly as age increased (p<0.001) (Table). However, men aged >65 years had a significant increase in prevalence during 1998--2004, and women aged 25--34, 45--64, and >65 years had significant increases during the same period. During 1998--2004, the prevalence of strength training increased significantly among non-Hispanic white men and women. In 2004, the prevalence of strength training among men was similar for non-Hispanic whites (23.1%), non-Hispanic blacks (22.9%), and those classified as "other" (21.3%). Strength training was least prevalent among Hispanic men (15.0%). In 2004, strength training among women was significantly higher among non-Hispanic whites (20.4%) than among non-Hispanic blacks (11.3%), Hispanics (9.1%), and those classified as "other" (12.9%). Reported by: J Kruger, PhD, S Carlson, MPH, H Kohl III, PhD, Div of Nutrition and Physical Activity, National Center for Chronic Disease Prevention and Health Promotion, CDC. Editorial Note:The findings in this report demonstrate that the national prevalence of strength training for U.S. adults increased slightly during 1998--2004. Nonetheless, only 21.9% of men and 17.5% of women (age adjusted) in 2004 reported strength training two or more times per week, which is substantially lower than the national 2010 objective of 30%. In addition, the greatest yearly increase was from 2000 to 2001 (p<0.001); however, since 2001, no further progress has been made. Although women experienced a significant increase during 1998--2004 and men did not, overall strength training levels among women remained lower than among men. The prevalence of strength training was lowest among respondents aged >65 years; nonetheless, respondents in this age group experienced the largest increase overall during 1998--2004. The factors that led to the increase in strength training in this group cannot be determined from this analysis, but possible explanations include increased promotion of active lifestyles among older adults (9) and programs that specifically promote strength training, such as Growing Stronger (10) and the Strong-for-Life program (4). Despite these gains, additional measures to promote strength training among adults are needed. Strength training throughout life can sustain functional independence for activities of daily living (1), such as the ability to carry groceries, rise from a chair, or walk up a flight of stairs. Findings from this analysis suggest that some racial/ethnic groups have a significantly lower prevalence of strength training than others. Strength-training prevalence was consistently lower among Hispanic respondents than among non-Hispanic white respondents during 1998--2004. However, all subgroups are at risk for not meeting national health objectives for 2010. Identification of barriers to strength training among all racial/ethnic groups, especially Hispanics, can guide the design of culturally appropriate interventions. One of the most important barriers for many adults, regardless of racial/ethnic subgroup, is initiating a strength-training program. Including another person in the program, such as a coworker, spouse, neighbor, or friend, can provide encouragement and motivation. The findings in this report are subject to at least two limitations. First, information on strength training is self reported and subject to response and recall bias. Second, misclassification errors in reporting might have affected prevalence estimates of strength training. For example, respondents might have interpreted the survey question differently or might not have understood the definitions of strength training and calisthenics. The survey question specified weight lifting and calisthenics, but because respondents were not asked to provide details, activities such as stair climbing might have been missed. Although the NHIS data indicate that the prevalence of strength training increased from 17.7% to 19.6%, the 2004 prevalence falls far short of the 2010 objective of 30%. Evidence-based studies have indicated that strength-training programs for older adults, such as Strong-for-Life (4), have resulted in strength improvements among participants; more programs like this are needed. Additional opportunities for adults to engage in strength training (e.g., in places where adults already pursue leisure-time physical activity, such as schools and community centers) could increase the prevalence of strength training. Additional opportunities are especially important for racial/ethnic groups with lower prevalences (9). The findings in this report also underscore the need to increase education on the benefits of strength training among targeted adult populations. References
|
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services. |
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Date last reviewed: 7/19/2006
|
|
|||||
|
HOME |
ABOUT MMWR |
MMWR SEARCH |
DOWNLOADS |
RSS
|
CONTACT
|
|||||
|
|
|||||
|