|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
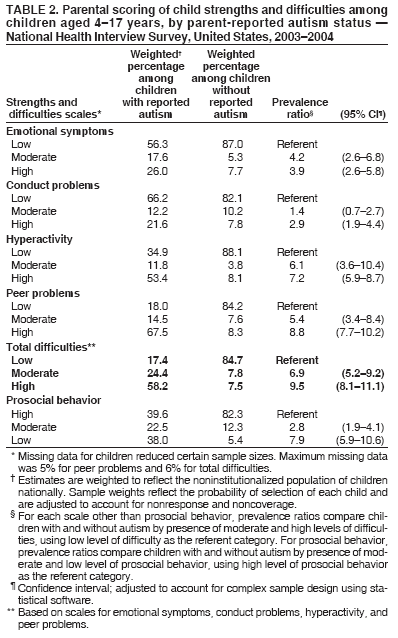
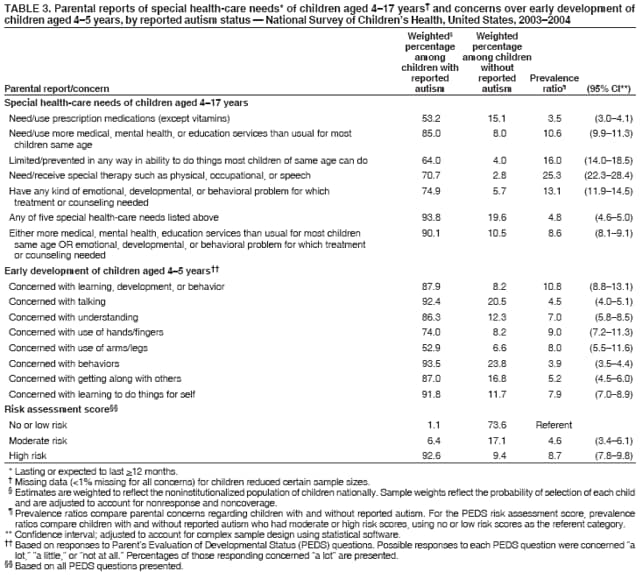
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Mental Health in the United States: Parental Report of Diagnosed Autism in Children Aged 4--17 Years --- United States, 2003--2004Autism is a lifelong neurodevelopmental disorder characterized by early onset of impairments in social interaction and communication and unusual, stereotyped behaviors. Autism (i.e., autistic disorder) often is classified with two related, although less severe, developmental disorders: Asperger disorder and pervasive developmental disorder--not otherwise specified. These three constitute the autism spectrum disorders (ASDs). Diagnosis of ASDs is based exclusively on developmental pattern and behavioral observation (Box). Two population-based studies conducted by CDC in selected U.S. locations reported ASD prevalence of 3.4 and 6.7 per 1,000 children, respectively (1,2). CDC also conducts two nationally representative surveys, the National Health Interview Survey (NHIS) and the National Survey of Children's Health (NSCH), in which parents are asked whether their child ever received a diagnosis of autism. Because of similarities in methodology used by the two surveys, CDC analyzed 2003--2004 data from NHIS and data from the first-ever NSCH (collected during January 2003--July 2004) to 1) estimate the population-based prevalence of parental report of diagnosed autism in the United States and 2) assess parental reporting of child social, emotional, and behavioral strengths and difficulties and special-health care needs among children with and without reported autism. This report describes the results of that analysis, which indicated that the prevalence of parent-reported diagnosis of autism was 5.7 per 1,000 children in NHIS and 5.5 per 1,000 children in NSCH. Prevalence estimates in the two studies were similar across age, sex, and racial/ethnic populations. The consistency in estimates between the two surveys suggests high reliability for parental report of autism. These estimates suggest that, as of 2003--2004, autism had been diagnosed in at least 300,000 U.S. children aged 4--17 years. In addition, parental reports of autism were associated with reported social, emotional, and behavioral symptoms and specialized needs. Thus, these surveys might be useful to assess health, education, and social service needs of children with autism. NHIS is an ongoing, annual, in-person survey of the civilian, noninstitutionalized U.S. population, based on a multistage sampling of housing units. NHIS includes a child survey component in which one child aged <17 years is selected randomly as the interview subject from each applicable household. Responses to questions about the child are obtained from parents or other knowledgeable adults. For this report, the analysis was based on 24,673 children from the combined NHIS surveys of 2003 and 2004, the most recent reporting years and a period comparable to that of the first NSCH interviews. Response rates for the child survey component of NHIS for 2003 and 2004 were 81.1% and 79.4%, respectively. NSCH is a random-digit--dialed telephone survey conducted by CDC as part of the State and Local Area Integrated Telephone Survey sponsored by the Maternal and Child Health Bureau of the Health Resources and Services Administration. NSCH was initiated in 2003 to estimate the prevalence of physical, emotional, and behavioral child health indicators in combination with information on the family context and neighborhood environment. The survey uses a multistage sampling method based on identification of households with one or more children aged <17 years and random selection of a sample child as the interview subject. Parents or guardians of 102,353 children completed the interview during January 2003--July 2004. The response rate was 55.5%. CDC plans to conduct this survey approximately every 4 years. In both surveys, autism was ascertained from the question: "Has a doctor or health-care provider ever told you that [child's name] has autism?" For both surveys, children who were aged 4--17 years at the time of the survey were selected; children with missing data on autism (<0.2%) were excluded. The final samples included 18,885 children from NHIS and 79,590 children from NSCH. Population-based estimates of parent-reported autism used weighted data to reflect the noninstitutionalized population of children nationally. From NHIS, the consistency between parent-reported autism and parental responses to the Strengths and Difficulties Questionnaire (SDQ) was examined. The SDQ is a 25-item behavioral screening instrument that includes both positive and negative psychological attributes. The items are divided into five scales: emotional symptoms, conduct problems, hyperactive behavior, peer relationships, and prosocial behavior. For each scale, children are categorized as having low, moderate, or high levels of difficulties on the basis of established criteria for U.S. children (3). From NSCH, the extent to which children reported to have autism also were reported to have special health-care needs was examined (4). Additionally, for children aged 4--5 years in the NSCH survey, a risk score for developmental delay was computed from responses to a series of questions from the Parent's Evaluation of Developmental Status (PEDS) questionnaire (5). PEDS is designed to identify children who have or are at risk for developmental problems generally, including developmental problems associated with ASD. Total prevalence estimates of parent-reported diagnosis of autism and estimates by sex, age, and race/ethnicity were similar for the two surveys (Table 1). Prevalence was 5.7 per 1,000 children (95% confidence interval [CI] = 4.5--7.2) in NHIS and 5.5 per 1,000 children (CI = 4.7--6.4) in NSCH. In both surveys, prevalence was 3.7 times as high for males as for females, peak prevalence was observed at ages 6--11 years, and lower rates were observed among children of Hispanic ethnicity. On the basis of NHIS data, children with parent-reported autism were more likely than children without autism to have moderate or high levels of emotional symptoms, conduct problems, hyperactivity, peer problems, and total difficulties (Table 2). Approximately 83% of children reported with autism had moderate or high levels of total difficulties compared with 15% of children without autism. The most notable differences were for peer problems (82.0% versus 15.9%) and hyperactivity (65.2% versus 11.9%). Substantially fewer children reported with autism had a high level of social skills (39.6%) compared with children without autism (82.3%). On the basis of NSCH data, 93.8% of children with parent-reported autism were classified as having special health-care needs lasting or expected to last >12 months; 90.1% were reported as needing more medical, mental health, or educational services than usual for a child of the same age or needing treatment or counseling for an emotional, developmental, or behavioral problem (Table 3). These percentages compared with 19.6% and 10.5%, respectively, for children reported without autism. Substantial differences also were observed among children aged 4--5 years regarding their risk for developmental delay, on the basis of the PEDS questions. Among those with reported autism, 92.6% were classified as at high risk for developmental delay, 6.4% were classified as at moderate risk, and 1.1% as at low risk. Among children without autism, 9.4% were classified as at high risk for developmental delay, 17.1% were classified as at moderate risk, and 73.6% as at low risk or no risk (Table 3). Reported by: LA Schieve, PhD, C Rice, PhD, C Boyle, PhD, Div of Birth Defects and Developmental Disabilities, SN Visser, MS, Div of Human Development and Disability, National Center on Birth Defects and Developmental Disabilities; SJ Blumberg, PhD, Div of Health Interview Statistics, National Center for Health Statistics, CDC. Editorial Note:Because diagnosis of autism is made only by assessment of developmental patterns and observation of behavioral symptoms, establishing and tracking prevalence is difficult; thus, multiple methods for case ascertainment can be useful. Parental report of autism diagnosis has not been assessed previously. However, a study of parental report of birth defects (6) documented high specificity; sensitivity varied depending on the defect. Validation studies of self-reported medical conditions among adults have reported similar findings (7,8). Although the autism diagnosis question from NHIS and NSCH has not been externally validated, the consistency of results from these two independent surveys of the U.S. population during the same approximate period suggests a degree of reliability of these estimates. The associations between reported autism and 1) parental rating of difficulties with SDQ items included in NHIS and 2) reports of special health-care needs and risk for developmental delay in NSCH suggest consistency between reported autism and expected behavioral and emotional symptoms and health-care use patterns. Moreover, the estimates of autism in this report and the male-to-female prevalence ratios are consistent with estimates from recent population-based studies of autism and ASD prevalence on the basis of clinical examination and medical and educational record review (1,2). Additionally the finding that parent-reported autism prevalence was highest during early school age (i.e., 6--11 years) appears similar to that of a 1996 study using medical and education record review in metropolitan Atlanta in which peak prevalence was observed among children aged 5--8 years (1). The findings in this report of parental report of diagnosed autism complement other CDC studies of the prevalence of autism, such as population-based surveillance conducted in Atlanta and other areas of the United States that compose the Autism and Developmental Disabilities Monitoring (ADDM) Network. Estimates from ADDM surveillance are on the basis of medical and education record review of eligible children aged 8 years and provide more detail regarding the prevalence of ASDs in selected U.S. populations. In addition, ADDM surveillance provides information on the clinical characteristics of children with ASDs and will provide data to track ASD prevalence trends in these populations. NHIS and NSCH data supplement ADDM data by providing national estimates of parent-reported diagnoses of autism. Because these surveys contain information on health-care use and family functioning, they might be helpful for future analyses examining the impact of ASDs on children and their families. Previous reports on parent-reported estimates of other developmental disabilities from NHIS (9) and of attention-deficit/hyperactivity disorder from NSCH (10) have provided valuable data on the national prevalence and insight into the impact of these disorders on children in the United States. Because autism is defined behaviorally, autism usually is not diagnosed before age 4 years. Later identification of children with autism might suggest an underestimate of autism prevalence among younger age groups. Similarly, although autism is considered a chronic condition, to what extent the "ever diagnosed" cases described in this report reflect parental report of current levels of clinical symptomatology rather than past diagnoses is unclear; thus, the peak prevalence estimates for children aged 6--11 years might be reflective of peak ages for diagnosis and treatment. Although Hispanic children had lower rates of reported autism in the two surveys, whether the lower rates resulted from etiologic differences or differential cultural factors related to autism symptom recognition and access to services for diagnosis and treatment could not be determined. Thus, differences observed between age or race/ethnicity subgroups should not be used to infer potential etiologic associations. Nonetheless, such differences point to the need to consider potential underdiagnosis in certain populations. CDC has recognized the need to improve early detection of autism and has begun a public education campaign with national partner groups (Learn the Signs. Act Early) to educate parents and professionals about early warning signs of autism and other developmental disorders and to encourage developmental screening and intervention. The findings in this report are subject to at least four limitations. First, the NSCH response rate was lower than the NHIS response rate; however, the comparability of the prevalence estimates suggests a differential nonresponse bias did not occur. Second, parental report of autism is dependent on access to appropriate health or educational services for diagnosis and communication of that diagnosis to the parent. Third, because the survey asked only about autism, how parents of children with diagnoses of other, less severe, ASD disorders (i.e., pervasive developmental disorder--not otherwise specified or Asperger disorder) might have responded is unclear. However, because prevalence estimates from NHIS and NSCH are greater than the estimate for ASDs (3.4 per 1,000 population) reported in a previous study (1) and the estimate for autism (4.0 per 1,000 population [compared with 6.7 per 1,000 for ASDs]) reported in another (2), the findings in this report might indicate that children with the other two ASDs were reported by their parents as having autism. Finally, the findings in this report represent cross-sectional analyses of NHIS and NSCH data from interviews conducted during the same approximate period and do not assess trends in the rate of autism. Results from these two national surveys of parental report of diagnosed autism suggest that, as of 2003--2004, autism had been diagnosed in at least 300,000 U.S. children aged 4--17 years. Parents who reported that their children had autism also reported these children experienced moderate or high levels of social, emotional, and behavioral difficulties and needed special health-care and educational services. These population-based surveys might be useful to assess the specialized health and educational needs of families and children with disabilities such as autism. References
|
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services. |
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Date last reviewed: 5/4/2006
|
|
|||||
|
HOME |
ABOUT MMWR |
MMWR SEARCH |
DOWNLOADS |
RSS
|
CONTACT
|
|||||
|
|
|||||
|