 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Surveillance for Dental Caries, Dental Sealants, Tooth Retention, Edentulism, and Enamel Fluorosis --- United States, 1988--1994 and 1999--2002Eugenio D. Beltrán-Aguilar, DMD,1 Laurie K.
Barker, MSPH,1 María Teresa Canto, DDS,2 Bruce A.
Dye, DDS,3 The material in this report originated in the National Center for Chronic Disease Prevention and Health Promotion, George A. Mensah, MD, Acting Director; and the Division of Oral Health, William Maas, DDS, Director. Corresponding author: Eugenio D. Beltrán-Aguilar, DMD, Division of Oral Health, National Center for Chronic Disease Prevention and Health Promotion, MS F-10, 4770 Buford Hwy, NE Atlanta, GA 30341; Telephone: 770-488-6069; Fax: 770-488-6080; E-mail: edb4@cdc.gov. Abstract Problem/Condition: Dental caries is a common chronic disease that causes pain and disability across all age groups. If left untreated, dental caries can lead to pain and infection, tooth loss, and edentulism (total tooth loss). Dental sealants are effective in preventing dental caries in the occlusal (chewing) and other pitted and fissured surfaces of the teeth. Enamel fluorosis is a hypomineralization of enamel related to fluoride exposure during tooth formation (first 6 years for most permanent teeth). Exposure to fluoride throughout life is effective in preventing dental caries. This is the first CDC Surveillance Summary that addresses these conditions and practices. Reporting Period: 1988--1994 and 1999--2002. System Description: The National Health and Nutrition Examination Survey (NHANES) is an ongoing survey of representative samples of the civilian, noninstitutionalized U.S. population aged >2 months in NHANES 1988--1994 and all ages during 1999--2002. The dental component gathered information on persons aged >2 years. Results: During 1999--2002, among children aged 2--11 years, 41% had dental caries in their primary teeth. Forty-two percent of children and adolescents aged 6--19 years and approximately 90% of adults had dental caries in their permanent teeth. Among children aged 6--19 years, 32% had received dental sealants. Adults aged >20 years retained a mean of 24 of 28 natural teeth and 8% were edentulous. Among persons aged 6--39 years, 23% had very mild or greater enamel fluorosis. Disparities were noticed across all age groups, among racial/ethnic groups, persons with lower education and income, and by smoking status. From 1988--1994 to 1999--2002, four trends were observed: 1) no change in the prevalence of dental caries in primary teeth among children aged 2--11 years, 2) a reduction in prevalence of caries in permanent teeth of up to 10 percentage points among persons aged 6--19 years and up to six percentage points among dentate adults aged >20 years, 3) an increase of 13 percentage points in dental sealants among persons aged 6--19 years, and 4) a six percentage point reduction in total tooth loss (edentulism) among persons aged >60 years. Interpretation: The findings of this report indicate that the dental caries status of permanent teeth has improved since the 1988--1994 survey. Despite the decrease in caries prevalence and severity in the permanent dentition and the increase in the proportion of children and adolescents who benefit from dental sealants, disparities remain. Public Health Action: These data provide information for public health professionals in designing interventions to improve oral health and to reduce disparities in oral health, for researchers in assessing factors associated with disparities and dental caries in primary teeth, and in designing timely surveillance tools to monitor total fluoride exposure. IntroductionSince 1996, a consortium formed by CDC and the National Institute of Dental and Craniofacial Research (NIDCR) has developed and implemented a plan to use the National Health and Nutrition Examination Survey (NHANES) to obtain epidemiologic estimates of dental conditions and preventive efforts. NHANES provides data for oral health surveillance at the national level. The specific objectives are to 1) assess the prevalence of major oral diseases and conditions, including dental caries, periodontal diseases, dental trauma, and enamel fluorosis; 2) assess efforts to prevent disease and disability, including prevalence of dental sealants and use/status of dentures; 3) monitor the oral health status of minority and underserved populations; and 4) provide estimates to evaluate the national health objectives for 2000 and 2010 related to oral health. Beginning in 1999, NHANES changed from a periodic, multiyear survey to a continuous, annual survey. Unlike previous NHANES surveys, beginning in 1999, data on a nationally representative sample of the U.S., noninstitutionalized civilian population from birth and all ages were released on a 2-year cycle. Oral health data were collected for persons aged >2 years, and data for NHANES 1999--2000 and for NHANES 2001--2002 were released for public use in March 2004 and in February 2005, respectively. This report was prepared by members of the consortium and provides summary data for study participants (SPs) for selected elements of the dental component (i.e., dental caries, dental sealants, enamel fluorosis, tooth retention, and edentulism [total tooth loss]). In this report, data from NHANES 1999--2000 and NHANES 2001--2002 were used in the aggregate and are referred to as NHANES 1999--2002. In addition, recalculated estimates for NHANES III (1988--1994), using comparable variables and age groups, were included to assess trends. MethodsNHANES 1999--2002 oversampled certain population subgroups to improve reliability of epidemiologic estimates. Expanded sampling included adolescents aged 12--19 years, persons aged >60 years, Mexican-Americans, non-Hispanic blacks, and persons of low-income. NHANES 1988--1994 oversampled children aged <6 years, persons aged >60 years, Mexican-Americans, and non-Hispanic blacks. Details of NHANES sample design, methods, and protocols are available at http://www.cdc.gov/nchs/about/major/nhanes/currentnhanes.htm. Oral health information was collected through face-to-face interviews by a trained interviewer in a participant's home and a dental examination conducted by a trained dentist in a mobile examination center (MEC). This report will focus on a selected group of oral health indicators obtained during the MEC examination. Further details on the home interview, MEC examination procedures, and technical notes are available in the documentation provided with the public release of the dataset (1). Reliability of ExaminationsDental examiners were calibrated periodically by the survey's reference dental examiner. Interrater and intrarater reliability were measured for each examiner by comparing examination findings with those of the reference examiner (for interrater reliability) and repeated examinations (for intrarater reliability). Both percent agreement and Cohen's Kappa (2,3) were calculated from paired observations. Kappa values ranged from 0.56 to 0.73 for enamel fluorosis and from 0.64 to 1.00 for dental caries and presence of dental sealants. Specific data points for quality assurance and reliability of examinations will be provided in a subsequent publication (4). Diagnostic CriteriaA list of terms and abbreviations is included to facilitate the reading and interpretation of the diagnostic criteria and results. Dental examiners were trained to use modified Radike's criteria (5) to diagnose dental caries and its sequelae (missing teeth [due to disease] and filled teeth). The modification consisted of eliminating the "extraction indicated" code. Dental examiners were asked to dry the tooth surfaces with compressed air and use a nonmagnifying mirror and a No. 23 dental explorer to assess for presence of carious and restored (filled) lesions. To be consistent with the NHANES 1988--1994 protocols and diagnostic criteria, pits and fissures were coded as carious if the explorer would catch after insertion with moderate, firm pressure, accompanied with either softness at the base of the lesion or an opacity adjacent or evidence of undermining enamel. Four surfaces of incisors and canines and five surfaces, including the occlusal surface, of premolars and molars were examined. No radiographs were taken. Detailed diagnostic and coding guidelines were included in the procedures manuals for dental examiners and recorders available at the NHANES website (1). Tooth- and surface-specific data points were used to calculate measures of caries prevalence and severity. Lower-case letters represent scores for primary teeth, and upper-case letters represent permanent teeth. Two measures of prevalence were calculated: the prevalence of tooth decay (caries experience, which includes untreated and restored lesions [see Terms and Abbreviations]) and the prevalence of untreated tooth decay. Indices used for severity of disease were the number of decayed and filled primary teeth (dft) or surfaces (dfs) and the number of decayed, missing, and filled permanent teeth (DMFT) or surfaces (DMFS) (6--9). The missing (m) component was not included in the calculation of indices for primary teeth. In addition, caries prevalence estimates for adults and seniors excluded missing teeth (see Terms and Abbreviations). These criteria have been used in previous surveys of dental caries to avoid misclassifying missing primary teeth that are normally exfoliated and permanent teeth that were extracted for reasons other than dental caries. In addition, the ratio of decayed or filled teeth or surfaces to the total number of decayed and filled teeth or surfaces among those who had experienced dental caries was calculated. This measure can be used to estimate the degree of unmet treatment need among the subset of the population with caries experience. In NHANES 1988--1994, the presence of dental root caries and restorations was assessed and recorded at the tooth-level (9); however, in NHANES 1999--2002, dental root conditions were assessed at the person level (one or more decayed root carious lesions or one or more filled root lesions). As a result, only prevalence of root caries and root restorations were included in this report. Dental sealants were assessed in permanent molars (occlusal and buccal surfaces in lower molars and occlusal and lingual surfaces in upper molars), premolars (occlusal surface), and upper lateral incisors (lingual surface). The same teeth were examined in NHANES 1988--1994 and NHANES 1999--2002, and dental examiners used a No. 23 dental explorer for tactile reference. In this report, a surface was considered sealed if any part of the surface remained covered with sealant material (10). A person was coded as having sealants when one or more permanent teeth were sealed (10). Prevalence of dental sealants was calculated among those having one or more permanent teeth eligible for placement of sealants. Tooth retention and complete tooth loss were based on 28 teeth (excluding third molars). The following case definitions from NHANES 1988--1994 (11) were used: an SP with at least one tooth present was considered "dentate," and an SP with all 28 teeth missing was considered "edentulous." Enamel fluorosis was assessed in all permanent teeth using Dean's Fluorosis Index (12). Each tooth was assigned to one of six categories: unaffected, questionable, very mild, mild, moderate, or severe fluorosis. A person was assigned a score corresponding to the two most affected teeth. If the two teeth were not equally affected, the score assigned was the lesser of the two. Russell's criteria were used in the differential diagnosis of fluorosis with other enamel opacities (13). Enamel fluorosis was not assessed in NHANES 1988--1994, and the only previously collected national data on enamel fluorosis were the 1986--1987 National Institute of Dental Research (NIDR) National Survey of Oral Health in U.S. School Children (14). Differences in study design between NIDR 1986--1987 and NHANES 1999--2002 should be considered when drawing inferences about changes in prevalence and severity of enamel fluorosis. Data Management and Analytic MethodsThe file structure of the public release data set differs between NHANES 1988--1994 and 1999--2002. Data users should review all pertinent documentation at the NHANES website (15) before conducting analyses comparing NHANES 1988--1994 to the current NHANES. The age categories used correspond generally to survey sampling domains (<5 years, 6--11 years, 12--19 years, 20--39 years, 40--59 years, and >60 years). The target population for the oral examination began at age 2 years. Adolescents aged 12--19 years were divided into two groups (12--15 years and 16--19 years) because the former category is the target age for placing sealants on second molars. Race/ethnicity was categorized as non-Hispanic white, non-Hispanic black, and Mexican-American. Estimates were not shown separately for persons of other race/ethnicity groups, although these persons were included in totals and strata by other characteristics. To minimize the impact of differences in age and sex distribution between surveys, all estimates were adjusted for age and sex to the U.S. 2000 standard population (16), except those stratified by sex, which were adjusted only for age. Data for dental caries and sealants among children and adolescents and enamel fluorosis were adjusted using single years of age. Data for dental caries, tooth retention, and edentulism among adults were adjusted using 10-year age groups. Despite the small difference observed between adjusted and nonadjusted estimates, this report includes adjusted estimates for NHANES 1999--2002 to allow comparisons with NHANES 1988--1994. Technical information on adjustment weights and coding for variable creation is available at the NIDCR/CDC Data Resource Center (DRC) (http://drc.nidcr.nih.gov). Poverty status was measured by the ratio of family income to the federal poverty level (FPL). Computed annually by the U.S. Census Bureau, FPL varies with family size and age of family members. In this report, poverty status was defined by three categories: family income <100% of the FPL, >100% but <200% of the FPL, and >200% of the FPL. Level of education was stratified into three categories: less than high school, high school graduate, and greater than high school. Smoking status was stratified into three categories: current smoker, former smoker, and never smoked. Statistical analyses were conducted using SAS® version 9.1 (SAS Institute, Inc.; Cary, North Carolina) and SUDAAN® version 9.0 (Research Triangle Institute; Research Triangle Park, North Carolina) to account for the complex sampling design. All analyses used sample weights to account for the unequal probability of selection and nonresponse to produce national estimates and standard errors. In this report, differences between 1988--1994 and 1999--2002 and differences between categories are noted if confidence intervals (CIs) do not overlap, a method that is less likely to detect differences than standard statistical tests (17). Sample sizes and population represented are presented by selected characteristics (Table 1). In this report, data are presented for 1) dental caries in primary teeth among children aged 2--11 years, 2) dental caries in the permanent teeth among children and adolescents aged 6--19 years, 3) dental sealants in permanent teeth among children and adolescents aged 6--19 years, 4) coronal and root caries among dentate adults aged >20 years, 5) tooth retention and edentulism among dentate adults aged >20 years, and 6) enamel fluorosis among persons aged 6--39 years. Because few participants had severe fluorosis, they were combined with those with moderate levels to increase the precision of the estimates. Data in the tables include overall estimates and are stratified by age, sex, race/ethnicity, and poverty status. In addition, data for adults aged >20 years include stratification by education level and smoking status. Bar charts have a similar structure but for adults, only age, sex, race/ethnicity, poverty, and smoking status were included. Results refer to the NHANES 1999--2002 survey unless otherwise noted. However, for comparison purposes, all tables and figures display data for the NHANES 1988--1994 and 1999--2002 surveys. ResultsDental Caries in Primary TeethAmong children aged 2--11 years, 41% had caries experience in their primary teeth (Table 2). Mexican-American children had higher caries experience (54.9%), compared with black (43.3%) or non-Hispanic white children (37.9%); children from families with incomes >200% of the FPL had lower caries experience (30.7%) compared with lower income groups (45.2% for those with family incomes >100% but <200% of the FPL and 55.3% for those with family incomes <100% of the FPL). Overall, no change was observed in the prevalence of dental caries in primary teeth among children from 1988--1994 to 1999--2002 (Table 2, Figure 1). Approximately 21% of children aged 2--11 years had untreated tooth decay in their primary teeth. Non-Hispanic white children and children from families with incomes >200% of the FPL had a lower prevalence (18.3% and 13.2%, respectively) of untreated tooth decay compared with non-Hispanic black (27.2%) and Mexican-American children (31.6%) or those from lower income groups, respectively (23.9% and 33.5%). Overall, no change was observed in the prevalence of untreated tooth decay in primary teeth among children from 1988--1994 to 1999--2002 (Table 3, Figure 2). The mean dft among children aged 2--11 years was 1.4 (Table 4). The mean dfs was 3.2 (Table 5). Mexican-American children had a mean dfs of 4.6, approximately one-and-a-half surfaces more than non-Hispanic white or black children. Children from families with incomes >200% of the FPL had a lower mean dfs (1.96) than did children from families with lower income (3.8 and 5.2). Overall, no change in mean dfs was observed from 1998--1994 to 1999--2002 (Table 5, Figure 3). Among those with at least one decayed or filled surface (dfs >0), 46.3% of dfs were decayed surfaces (%ds/dfs) (Table 6, Figure 4). Dental Caries in Permanent Teeth of Children and AdolescentsAmong children and adolescents aged 6--19 years, 42.0% had caries experience in their permanent teeth (Table 7). Caries experience in permanent teeth was higher among females (44.5%) than males (39.5%) in this age group. Mexican-American children and adolescents had higher caries experience (48.8%), compared with non-Hispanic white (39.9%) or black children and adolescents (38.8%). Children and adolescents from families with incomes >200% of the FPL had lower caries experience (36.1%), compared with lower income groups (46.7% for those with family incomes >100% but <200% of the FPL and 48.3% for those with family incomes <100% of the FPL). Overall, absolute reduction in the prevalence of dental caries from 1988--1994 to 1999--2002 was 7.4%; the decline was larger among adolescents aged 16--19 years (10.2%) and for children and adolescents from families with incomes >200% of the FPL (10.5%) (Table 7, Figure 5). Approximately 14% of children and adolescents aged 6--19 years had untreated tooth decay in their permanent teeth (Table 8). Non-Hispanic white children and adolescents had a lower prevalence (10.7%), compared with non-Hispanic black (18.1%) and Mexican-American children and adolescents (21.8%). Children and adolescents from families with incomes >200% of the FPL had a lower prevalence of untreated tooth decay (8.1%), compared with lower income groups (both 19.5%). A trend toward lower prevalence of untreated tooth decay was observed in 1999--2002 compared with 1988--1994, but CIs overlap. The largest absolute reduction was observed among non-Hispanic black children and adolescents (from 24.4% to 18.1%) (Table 8, Figure 6). The mean DMFT among children and adolescents aged 6--19 years was 1.6 (Table 9). The mean DMFS was 2.7 (Table 10). Children and adolescents from families with incomes >200% of the FPL had a lower mean DMFS (2.1), compared with families with lower income (3.2 and 3.3). Overall, DMFS was lower in 1999--2002 than in 1988--1994, with an absolute reduction of 0.57 surfaces. Absolute reductions were larger among adolescents aged 16--19 years (1.24 surfaces) and among children and adolescents from families with incomes >200% of the FPL and non-Hispanic black children and adolescents (0.80 and 0.78, respectively) (Table 10, Figure 7). Among those with at least one DMFS in permanent teeth (DMFS >0), 24.3% of DMFS were decayed surfaces (%DS/DMFS), 72.5% were filled surfaces (%FS/DMFS), and 3.2% were missing surfaces (%MS/DMFS). The %DS/DMFS among non-Hispanic white children and adolescents was lower (19.3%) than among Mexican-American (33.6%) and non-Hispanic black children and adolescents (35.9%). The %DS/DMFS was lower among children and adolescents from families with incomes >200% of the FPL (17.0% compared with 29.1% and 30.4% for lower family incomes) (Table 11, Figure 8). Dental SealantsAmong children and adolescents aged 6--19 years, 32% had one or more surfaces sealed on their permanent teeth (molars, premolars, or lateral incisors) (Table 12). Prevalence of dental sealants among children and adolescents aged 12--15 years (37.4%) was higher than among those aged 6--11 years (29.5%) and 16--19 years (31.4%). A larger proportion of non-Hispanic white children and adolescents had at least one sealed tooth (37.9%) than did Mexican-American (23.4%) or non-Hispanic black children and adolescents (22.7%). Children and adolescents from families with incomes >200% of the FPL were more likely to have one or more sealed teeth than were those from families with lower incomes (Table 12, Figure 9). The proportion of children and adolescents with one or more sealed permanent tooth surfaces increased approximately 13%, from 19.6% in 1988--1994 to 32.2% in 1999--2002 (Table 12). Increases occurred among males and females and all racial/ethnic, income, and age groups. The largest increase occurred among adolescents aged 16--19 years (from 13.3% to 31.4%) (Table 12, Figure 9). Children and adolescents aged 6--19 years with at least one sealed tooth had a mean of 4.5 sealed teeth (Table 13). The mean number of sealed teeth was 3.4 for children aged 6--11 years, 5.1 for adolescents aged 12--15 years, and 5.5 for persons aged 16--19 years (Table 13). First and second permanent molars were more likely to be sealed than were premolars (Table 14, Figure 10) and lateral incisors. Molars accounted for 85% of all sealed teeth; 98.2% of children with at least one sealed tooth had at least one sealed molar. Dental Caries in AdultsCoronal Caries Approximately 91% of dentate adults aged >20 years had caries experience (Table 15). Caries experience was lowest among dentate persons aged 20--39 years (86.8%), with little difference between persons aged >60 years (93.1%) and persons aged 40--59 years (95.1%). Dentate non-Hispanic white adults aged >20 years had higher coronal caries experience (93.3%) than did non-Hispanic black (84.6%) and Mexican-American (83.5%) adults. Dentate adults with family income >200% of the FPL had a higher caries experience (93.2%) than did those with lower incomes (89.1% for those with family incomes >100% but <200% of the FPL and 86.7% for those with family incomes <100% of the FPL). Overall, caries experience reduction among dentate adults aged >20 years was 3.3%, from 94.6% in 1988--1994 to 91.3% in 1999--2002. The greatest absolute reduction occurred among adults aged 20--39 years (6.4%) and those with less than a high school education (5.1%) (Table 15, Figure 11). Among dentate adults aged >20 years, 23% had untreated tooth decay (Table 16). The prevalence of untreated tooth decay was higher among males and adults aged 20--39 years. Dentate non-Hispanic white adults had a lower prevalence (18.4%) of untreated tooth decay than Mexican-American (35.9%) and non-Hispanic black (41.3%) adults. Dentate adults with family income >200% of the FPL had a lower prevalence (15.7%) of untreated tooth decay than did those with lower family incomes (35.3% and 40.9%). Prevalence of untreated tooth decay was inversely correlated with higher level of education; prevalence was 40.9% among those with less than a high school education, 29.8% among high school graduates, and 13.6% among those with more than a high school education. Dentate adults who were current smokers had a higher prevalence of untreated tooth decay (35.0%) than did those who never smoked (18.6%) and former smokers (17.7%). Overall, the prevalence of dentate adults with untreated tooth decay decreased 5.1%, from 27.9% in 1988--1994 to 22.7% in 1999--2002. The greatest absolute reductions (7%--8%) were observed among those with family income <200% of the FPL, those aged >60 years, and non-Hispanic black adults (Table 16, Figure 12). Dentate adults aged >20 years had a mean of 8.0 decayed and filled permanent teeth (DFT) (Table 17) and 20.9 decayed and filled permanent surfaces (DFS) (Table 18, Figure 13). Dentate non-Hispanic white adults had a higher mean DFS (23.1) than Mexican-American (13.9) and non-Hispanic black (12.1) adults. Dentate adults with family income >200% of the FPL had a higher mean DFS (23.1) than those with lower income (15.9 and 14.5). Education level was directly correlated with mean DFS (24.1 surfaces among those with more than a high school education, 19.4 surfaces among those with a high school education, and 14.2 surfaces among those with less than high school education) but inversely correlated with mean number of untreated decayed surfaces (Table 18). The mean DFS among dentate adults decreased from 23.5 surfaces in 1988--1994 to 20.9 surfaces in 1999--2002. The largest decreases were observed among adults aged 20--39 years and those with more than a high school education (approximately four surfaces) (Table 18). Among dentate adults aged >20 years who had at least one DFS (DFS>0), 12.3% of the DFS were decayed surfaces (%DS/DFS) (Table 19). Non-Hispanic white adults had the lowest percentage (8.7%), compared with Mexican-American (26.2%) and non-Hispanic black (31.0%) adults. Adults with family incomes >200% of the FPL had the lowest %DS/DFS (6.8%) compared with adults from families with lower income (20.7% and 29.6%). The %DS/DFS was inversely correlated with education level: 5.4% among those with more than a high school education, 15.1% among high school graduates, and 30.6% among those with less than a high school education. Dentate adults who were current smokers had a higher proportion of %DS/DFS (21.2%) then adults who never smoked (9.8%) and former smokers (8.4%) (Table 19, Figure 14). Root Caries Approximately 18% of dentate adults aged >20 years had root caries (including untreated and restored lesions) (Table 20). Prevalence of root caries increased with age: 9.4% among persons aged 20--39 years, 17.8% among those aged 40--59 years, and 31.6% among those aged >60 years. Ten percent had one or more untreated carious lesions in roots (untreated root caries). Women had a lower prevalence of untreated root caries (8.9%) than men (12.1%). Non-Hispanic white adults had a lower prevalence of untreated root caries (8.5%) than Mexican-American (14.9%) and non-Hispanic black (21.7%) adults. Prevalence of untreated root caries was lower among those with family incomes >200% of the FPL (6.8%) than among those with lower income (16.6% for those with family incomes >100% but <200% of the FPL and 22.8% for those with family incomes <100% of the FPL). Education was inversely correlated with prevalence of untreated root caries: 20.3% among those with less than a high school education, 13.0% among high school graduates, and 5.8% among those with greater than a high school education. Current smokers had a higher prevalence of untreated root caries (21.1%) compared with former and never smokers (both approximately 7%). Overall, the prevalence of untreated root caries decreased among dentate adults aged >20 years, from 13.5% in 1988--1994 to 10.3% in 1999--2002. Decreases were greater among those aged >60 years (from 20% to 12.8%), Mexican-Americans (from 21.3% to 14.9%), and those with family incomes between 100% and 200% of the FPL (from 22.9% to 16.6%) (Table 20, Figure 15). Approximately 9% of dentate adults aged >20 years had one or more filled roots (restored) (Table 20). The prevalence was greater for those aged >60 years (22.1%), compared with those aged 40--59 years (8.0%) and those aged 20--39 years (1.7%). Prevalence of filled roots was higher among non-Hispanic white adults (9.0%) than among non-Hispanic black adults (4.5%). Tooth Retention and EdentulismOn average, dentate adults aged >20 years have approximately 24 teeth (a full dentition is equivalent to 28 teeth) (Table 21). Mean number of teeth was inversely correlated with age: 26.6 teeth among adults aged 20--39 years, 23.9 teeth among adults aged 40--59 years, and 19.4 teeth among adults aged >60 years. Non-Hispanic white and Mexican-American adults had more teeth (24.3 and 24.1, respectively) than non-Hispanic black adults (22.0). Adults with family income >200% of the FPL had more teeth (24.6) than those with family income >100% but <200% of the FPL (22.5) and those with family incomes <100% of the FPL (22.1). Adults with more than a high school education had more teeth (25.0) than high school graduates (23.2) or adults with less than a high school education (21.9). Persons who reported never smoking had more teeth (24.7) than former smokers (24.0) and current smokers (22.0). On average, adults aged >20 years retained one more tooth during 1999--2002 than during 1988--1994 (Table 21, Figure 16). Approximately 8% of adults aged >20 years had lost all their natural teeth (edentulism) (Table 22). Prevalence of edentulism increased with age: <1% among adults aged 20--39 years, 4.9% among those aged 40--59 years, and 24.9% among those aged >60 years. Mexican-American adults had a lower prevalence of edentulism (5.6%) than non-Hispanic blacks (9.5%). Adults with family income >200% of the FPL had a lower prevalence of edentulism (4.8%) than adults with lower family incomes (11.6% and 14.6%). An inverse correlation was observed between edentulism and education: 13.5% of adults with less than a high school education, 9.1% of adults who graduated from high school, and 3.5% of adults with more than a high school education were edentulous. A correlation also was observed between edentulism and smoking: 14.4% among current smokers, 7.9% among former smokers, and 4.5% among those who never smoked. Overall, edentulism decreased from 10.8% in 1988--1994 to 7.7% in 1999--2002. The largest decreases were observed among adults with family incomes between 100% and 200% of the FPL, for those with less than a high school education, and among adults aged >40 years (Table 22, Figure 17). Enamel FluorosisVery mild or greater enamel fluorosis was observed in 23% of persons aged 6--39 years (Table 23, Figure 18). The prevalence of fluorosis was lowest among persons aged 20--39 years (Figure 18). Non-Hispanic blacks had higher proportions of very mild and mild fluorosis than did non-Hispanic white participants (Figure 19). Posterior teeth were more affected by enamel fluorosis than were anterior teeth (Figure 20). A nine percentage point increase in the prevalence of very mild or greater fluorosis was observed among children and adolescents aged 6--19 years when data from 1999--2002 were compared with those from the NIDR 1986--1987 survey of school children (from 22.8% in 1986--1987 to 32% in 1999--2002) (18). DiscussionDental CariesDental caries and tooth loss were among the most common causes for rejection of young men from military service during the Civil War and the two World Wars (19). So widespread was the disease in the early 20th century that Klein designed and introduced the DMFT index as a sensitive tool to describe the distribution of the disease by counting the number of decayed, missing, and filled teeth affected (6). The introduction of fluorides for preventing dental caries, starting with water fluoridation in the mid-1940s, changed the pattern of disease occurrence. During 1960--1962, NCHS conducted the first national survey that included clinical assessments of dental caries in adults (20). This was followed by two similar national surveys during 1963--1970 among children aged 6--11 years and youth aged 12--17 years (21,22). These three surveys were part of the NCHS National Health Examination series, which later were reorganized as NHANES. NCHS surveys and those conducted by NIDR (since 1998, NIDCR) (14,23,24) were used to document a decline in dental caries the United States in both primary and permanent teeth (25). Data from NHANES 1988--1994 and NHANES 1999--2002 suggest no change in the prevalence and severity of dental caries in primary teeth but a decrease in permanent teeth. Historically, a decline in dental caries in primary teeth was reported until the mid-1980s, when data from the two NIDR surveys were compared (26). However, later reports have suggested that this decline has slowed or reversed in the United States and elsewhere (26,27). Data from this report support those findings. During 1999--2002, declines in caries prevalence and severity in the permanent dentition were observed across all age groups and for certain racial/ethnic groups, poverty level, education, and smoking characteristics when compared with data from 1988--1994. These reductions in dental caries also are reflected in increased tooth retention and reduced levels of edentulism, as has been reported elsewhere for selected populations (28). However, as the population ages and persons retain more teeth, more root surfaces become exposed and are at increased risk for tooth decay (29). These findings highlight the importance of developing strategies for preventing and controlling dental caries in older adults. Despite gains in oral health associated with dental caries, disparities remain. Overall, non-Hispanic white survey participants had a lower prevalence and severity of disease and lower prevalence of untreated decay compared with non-Hispanic black and Mexican-American participants. In addition, those with family incomes >200% of the FPL also had lower prevalence and severity of disease than others with lower family incomes. These results are consistent with reports that associate poverty, lower income and education, and certain racial/ethnic groups with higher levels of dental caries among adults and children (30). In addition, these results also support an association between tobacco use, dental caries, and tooth loss (31--33), which might have both a biologic and socioeconomic etiologic link. Dental SealantsDental sealants are highly effective in preventing dental caries that occur on the surfaces of teeth that have pits and fissures. Fully retained sealants are 100% effective (34,35). In examining the effectiveness of school-based or school-linked dental sealant programs, the Guide to Community Preventive Services documented a 60% decrease in tooth decay on the chewing surfaces of posterior teeth up to 5 years after sealant application (36). School-based sealant programs also are cost-saving (37). In 2002, the Task Force on Community Preventive Services strongly recommended school-based or school-linked sealant programs for the prevention and control of dental caries (36). Although sealant prevalence increased >12% from 1988--1994 to 1999--2002 (from 19.6% to 32.2%), it is still well below the national health objective for 2010 of 50% (38). The increase in sealant prevalence might be attributable to increases in both dental office-delivered and school-based and -linked sealant programs. The increased prevalence of sealants from 1988--1994 to 1999--2002 was observed across all sociodemographic groups and might have contributed to the reported decrease in dental caries in permanent teeth. Data from this report also suggest that disparities by race/ethnicity and income, as related to sealant use, might be decreasing. The proportional increase in sealant prevalence among racial/ethnic minorities was about three times that of non-Hispanic white children and adolescents, and the proportional increase among lower income children and adolescents was almost twice that of their counterparts in families with higher incomes. Despite these gains, profound disparities still exist. Non-Hispanic white children and adolescents and those from families with higher incomes who were documented in this report as having lower levels of tooth decay were at least 60% more likely to have received a sealant than were other racial/ethnic minorities and those from families with lower incomes. School-based and -linked programs in the United States generally target vulnerable populations less likely to receive private dental care (e.g., populations attending schools with a large proportion of students eligible for free or reduced-cost meal programs). An expansion in the number of these programs might decrease disparities in the prevalence of sealants (39). Tooth Retention and EdentulismThe findings in this report indicate that the prevalence of tooth loss continues to decline in the United States and provides further evidence that edentulism is not inevitable with advanced age. The decrease in the prevalence of edentulism between the two surveys might in part be attributed to the increased adoption of preventive regimens such as dental sealants, community water fluoridation, use of fluoride toothpaste and mouth rinse, and support for these approaches by health-care providers, health decision makers, and public health officials. Despite improvements in tooth loss and edentulism, disparities remain. Older adults and smokers were consistently worse off than their counterparts. These population subgroups are probably at increased risk for adverse consequences of tooth loss and other dental problems on quality of life and general health. These consequences can include limitations in chewing, dissatisfaction with appearance, avoidance of social contacts, and trouble speaking (30,40). Racial/ethnic differences in tooth loss exist, with non-Hispanic black adults retaining fewer teeth than non-Hispanic white and Mexican-American adults. Findings also suggest that Mexican-Americans continue to have the lowest prevalence of edentulism, although non-Hispanic whites also have experienced a decline in edentulism since 1988--1994. Tooth loss and edentulism reflect differences in healthy behaviors, attitudes toward oral health and dental care, and access to and use of dental services and types of treatment received (30,41--43). In addition, tooth loss is influenced by expectations about health. Further research is needed to determine why Mexican-Americans retain more teeth than non-Hispanic blacks and non-Hispanic whites despite having more dental caries in the younger cohorts. In addition, findings are influenced by the oral health status of the oldest cohorts (>60 years), who experienced higher rates of dental caries and tooth extractions and might have had different expectations toward retaining teeth earlier in life than persons aged <60 years (41,43). Certain studies have focused on tooth loss and its relation to diet and nutritional status. Two studies have documented that the intake of fruits and vegetables was negatively affected by the loss of teeth (44,45). Persons who have lost all or a substantial number of their teeth consumed fewer important nutrients, including dietary fiber (44,46--50). Biochemical levels of important nutrients were lower among those missing all or a substantial number of teeth (48--50). In addition, persons who had lost a substantial number of teeth were more likely to be obese than those with more teeth (48,51). These findings underscore the concept of a possible threshold number of teeth necessary for a "functional dentition" (52--54). Despite the overall decrease in tooth loss, continued research and tailored preventive efforts to eliminate those disparities are needed. Enamel FluorosisEnamel fluorosis is a hypomineralization of enamel, characterized by greater surface and subsurface porosity than normal enamel, and is related to fluoride ingestion during periods of tooth development by young children (55) (first 6 years of life for most permanent teeth). Although use of fluoride in various modalities has been important in the prevention and control of dental caries, it also introduces the risk for enamel fluorosis. The milder forms of enamel fluorosis typically are not noticeable; however, more severe levels might be objectionable for cosmetic reasons. Historically, a low prevalence of the milder forms of fluorosis has been accepted as a reasonable and minor consequence balanced against the substantial protection afforded by dental caries from the use of fluoridated drinking water and foods, beverages, and oral care products that contain fluoride. Reported risk factors for the more severe forms of fluorosis include drinking water with high natural fluoride levels, dietary fluoride supplements (particularly when prescribed for children with other sources of systemic fluoride), ingestion of fluoride toothpaste, and having multiple sources of ingested fluoride (56--61). The data in this report identify a group of children and adolescents with higher levels of very mild, mild, and moderate/severe fluorosis compared with children and adolescents of similar age examined during 1986--1987 (9 percentage point increase). These two surveys are the only sources of national data on enamel fluorosis. The surveys differed in sampling and representation (schoolchildren versus household survey) and in procedures followed (14 examiners during 1986--1987 versus four during 1999--2002). Examiner reliability was considered acceptable in both surveys (4,14). Cohorts aged 12--15 and 16--19 years during 1999--2002 generally had higher proportions of very mild, mild, and moderate/severe fluorosis than did the age 20--39 years cohort. The cohort aged 6--11 years had fewer premolars and molars erupted, limiting comparison to other cohorts (Figure 18). In analyzing these cohort effects and their causes, two things need to be considered: the time at which the teeth of these cohorts were at risk of fluorosis and the different sources of systemic fluoride available at that time. Studies on use of fluorides exist (62--65), but they do not provide information on combined exposures. Furthermore, not until the early 1990s were public health approaches introduced to limit the exposure to systemic fluoride from toothpaste and supplements (66), when the risk for fluorosis for most teeth in the age 12--19 year cohort was no longer subject to change. A potentially important source of fluoride is toothpaste. From approval of the first fluoride toothpaste by the American Dental Association in 1964, the total market share of fluoride toothpaste increased from <20% to 90% in 1980 (63). By 1980, proportionately more young children were using fluoride toothpaste than were earlier cohorts (62,64). In addition, although professional interest in limiting the amount of fluoride toothpaste delivered to young children and supervising their toothbrushing was expressed earlier in the 1980s (65), only during the early 1990s was this approach adopted broadly as a public health measure (66), which was too late to alter the risk for fluorosis among the 12--19 year age cohort in NHANES 1999--2002. No clear explanation exists why fluorosis was more severe among non-Hispanic black children than among non-Hispanic white or Mexican-American children. This observation has been reported elsewhere (67--70), and different hypotheses have been proposed, including biologic susceptibility or greater fluoride intake (70). Anterior teeth were less affected by enamel fluorosis than were posterior teeth. This finding also was reported in the NIDR 1986--1987 survey (71) and has been attributed to cohort effects, attrition, or a combination of the smaller anatomical surface and longer formation time of posterior teeth compared with anterior teeth (18,71). Further research also is needed to improve public health surveillance of fluoride exposure. The difficulties observed in comparing data from the NIDR 1986--1987 and NHANES 1999--2002 surveys and the time lapse between exposure and clinical presentation suggest the need for new and more timely methods to measure total fluoride exposure. Methods such as fingernail analysis (72--74) and urinary fluoride excretion (75--77) have shown promise, but only with limited samples. Research in these areas could result in the development of valid and reliable techniques to monitor total fluoride exposure in children, allowing adjustment in public health practice and recommendations to reduce the cosmetic consequences of fluoride exposure while preventing and controlling dental caries. CDC recommendations for the use of fluorides in the United States include using just a "pea-sized" amount of toothpaste for children aged <6 years, supervising children's toothbrushing to avoid excessive swallowing of toothpaste, and risk-based targeting of other fluoride modalities (66). Epidemiologic data from Australia indicate that targeting reduction in discretionary intake of supplements and toothpaste can reduce the prevalence of enamel fluorosis (78). Information is not available to evaluate the effects of these changes in the United States after they were implemented in the early 1990s. Increased efforts are needed to disseminate published recommendations about appropriate use of fluoride to health professionals and the public. ConclusionsThis report documents improvements in the oral health of the civilian, U.S. population. The report documented important differences in disease prevalence and severity by sociodemographic characteristics that public health officers, the dental profession, and the community should consider in implementing interventions to prevent and control disease and to reduce the disparities observed. The following is a list of seven important findings in this report:
Recommendations for Public Health Action
Acknowledgments The authors thank former members of the U.S. Public Health Service Oral Health Coordination Committee and the agencies they represented at that time: Dr. Dushanka Kleinman and Dr. Deborah Winn (NIDCR), Dr. Donald W. Marianos (CDC Division of Oral Health---DOH), Dr. William R. Maas (Agency for Health Care Policy and Research---AHCPR), Dr. Stephen Corbin (Public Health Service), John P. Rosetti (Health Resources and Services Administration), Dr. R. Frank Martin (Indian Health Service), and Dr. Carolyn Tylenda (Food and Drug Administration) for their vision and support that led to the inclusion of an oral health component at the NHANES cycle beginning in 1999. We would also like to thank Dr. Stuart Lockwood, former Dental Officer at DOH and Dr. Dolores Malvitz, former Team Leader for the DOH Surveillance, Investigation and Research Team, for fostering the idea of this surveillance summary during their tenure at DOH. Finally, our thanks to Dr. William R. Maas, Dr. William Kohn, Dr. Scott Presson, and Amy Collins from DOH, for their comments and suggestions. References
Terms and Abbreviations Used in the Report
Table 1 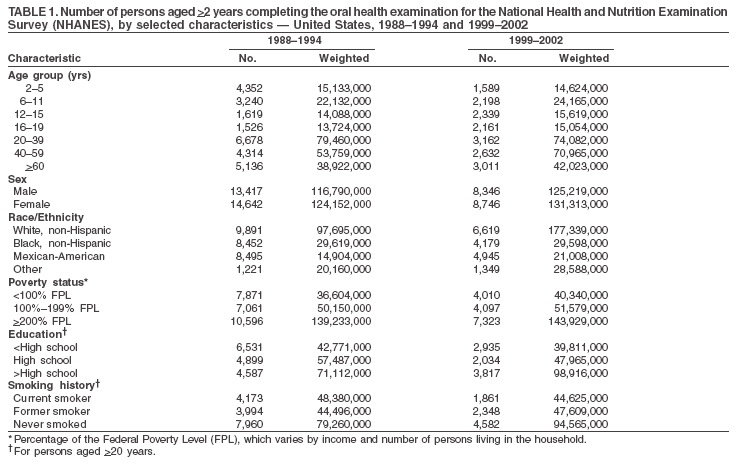 Return to top. Figure 1 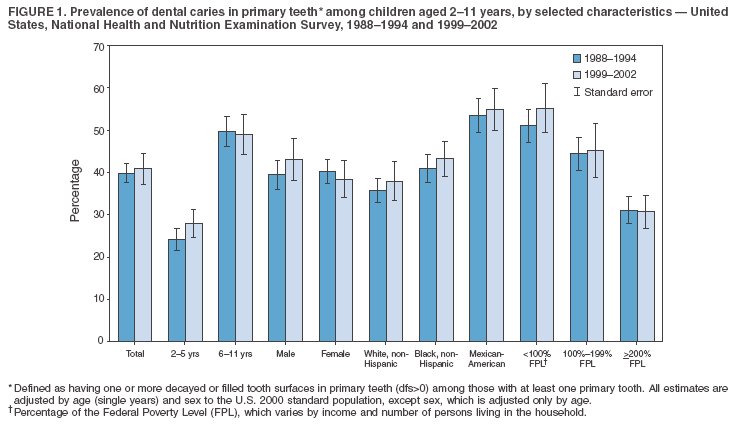 Return to top. Table 2 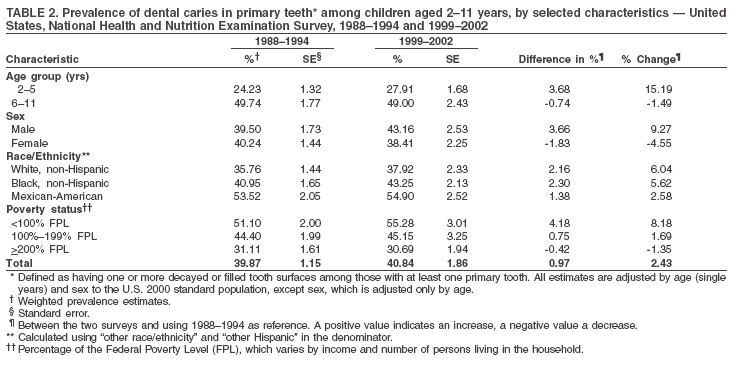 Return to top. Figure 2 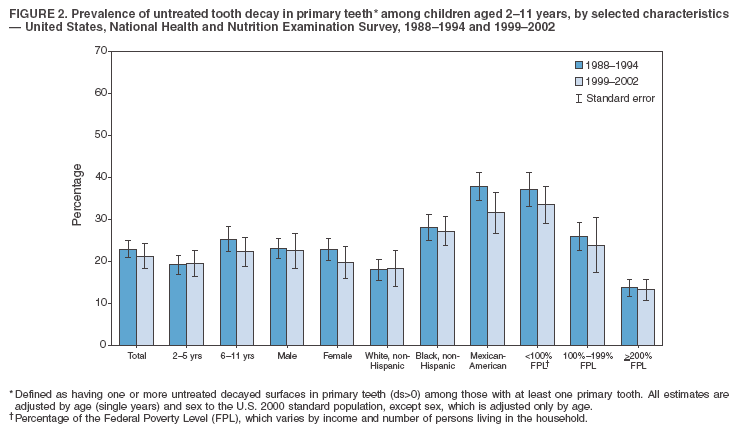 Return to top. Table 3 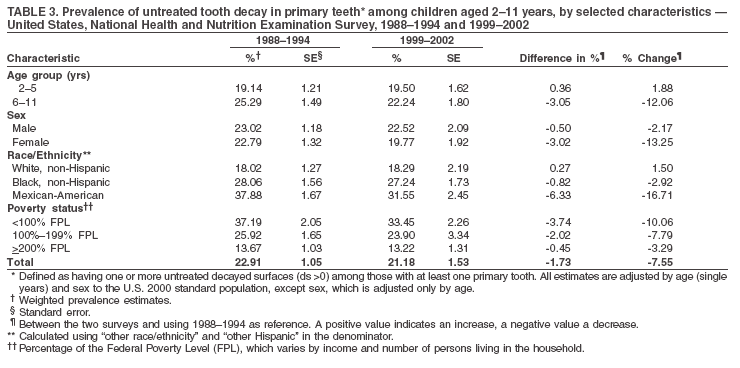 Return to top. Figure 3 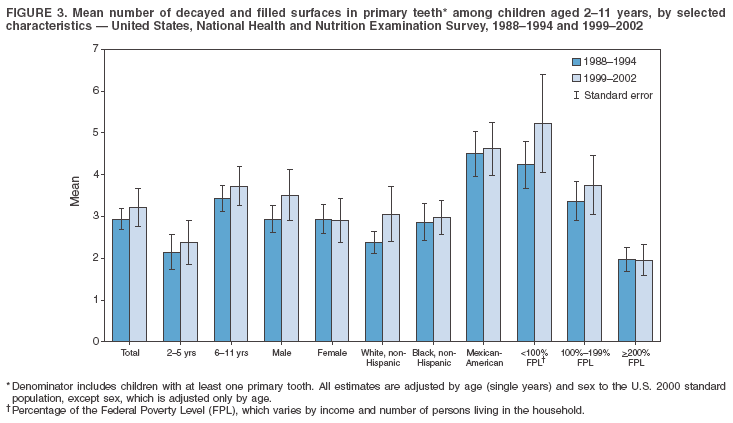 Return to top. Table 4 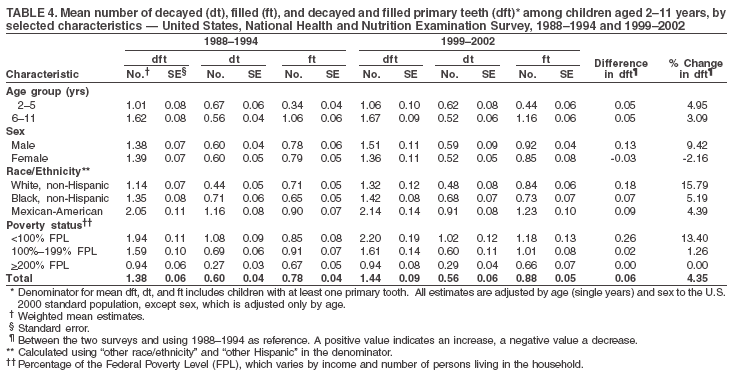 Return to top. Figure 4 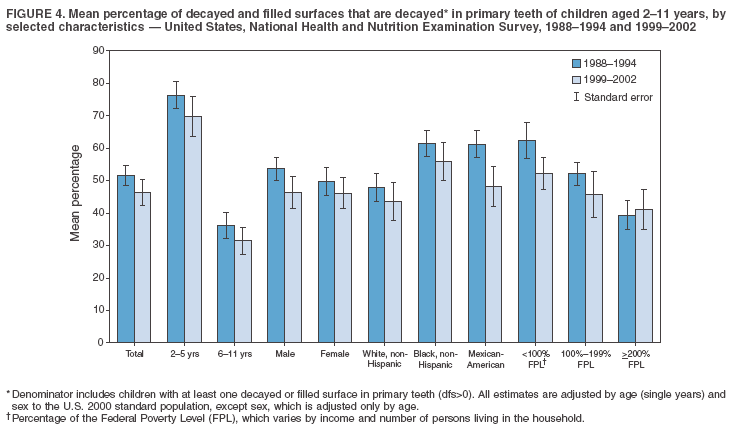 Return to top. Table 5  Return to top. Figure 5 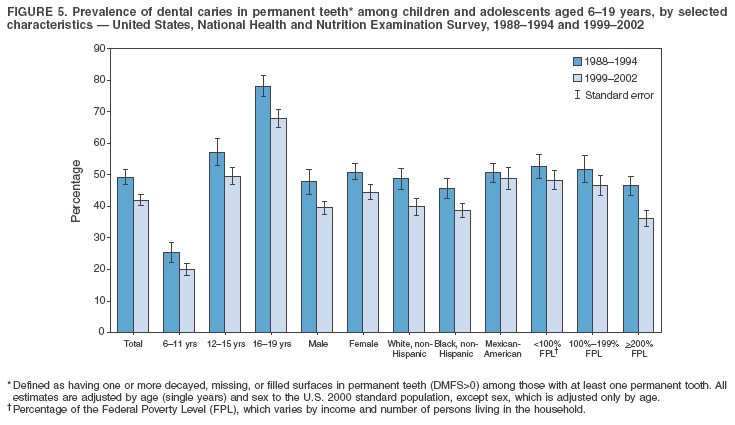 Return to top. Table 6 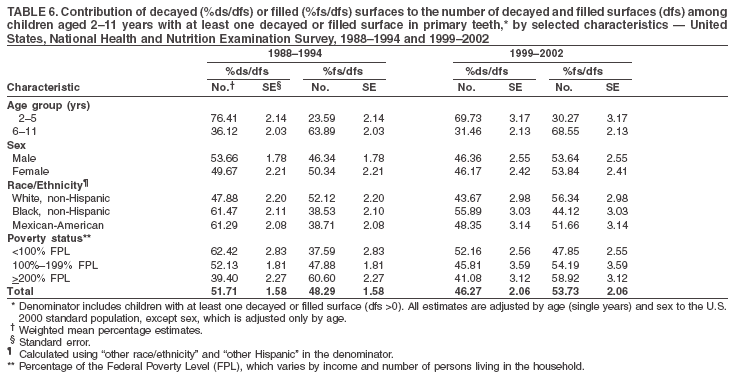 Return to top. Figure 6 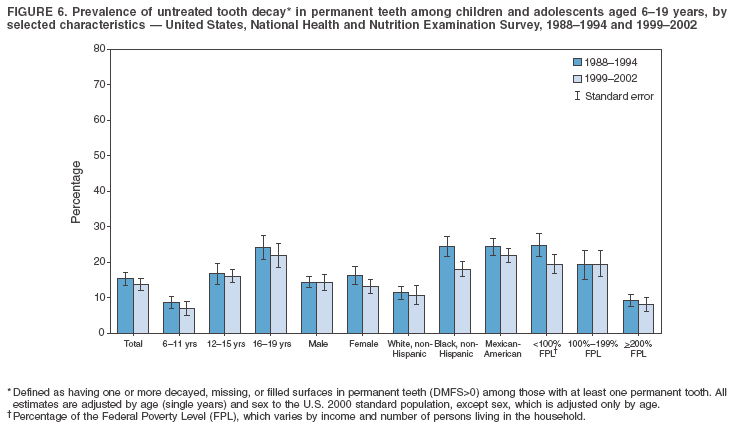 Return to top. Table 7 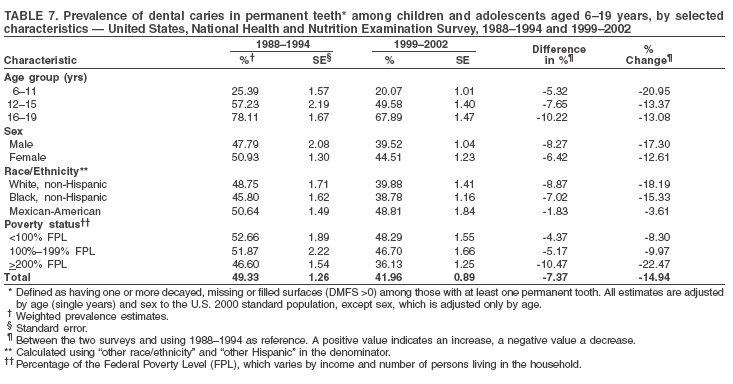 Return to top. Figure 7  Return to top. Table 8 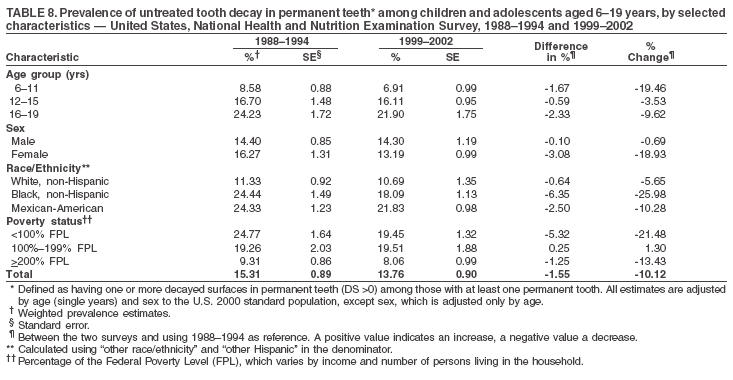 Return to top. Figure 8 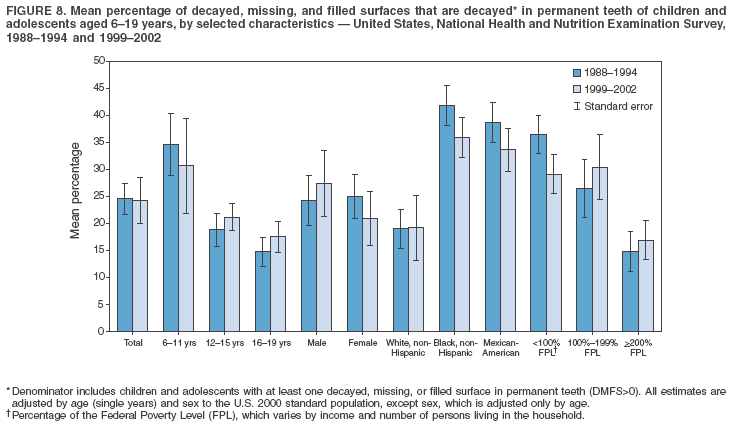 Return to top. Table 9 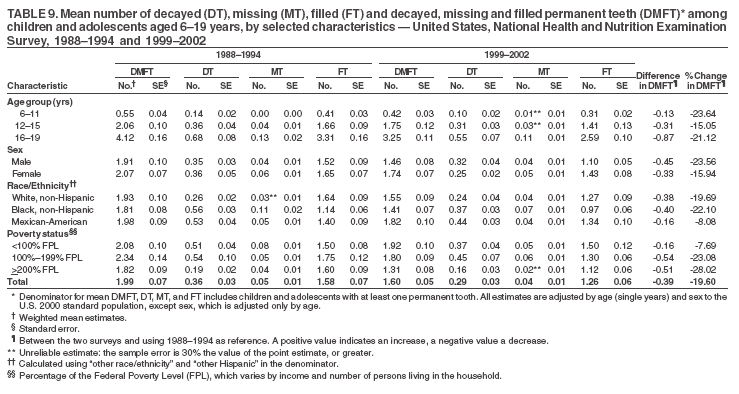 Return to top. Figure 9 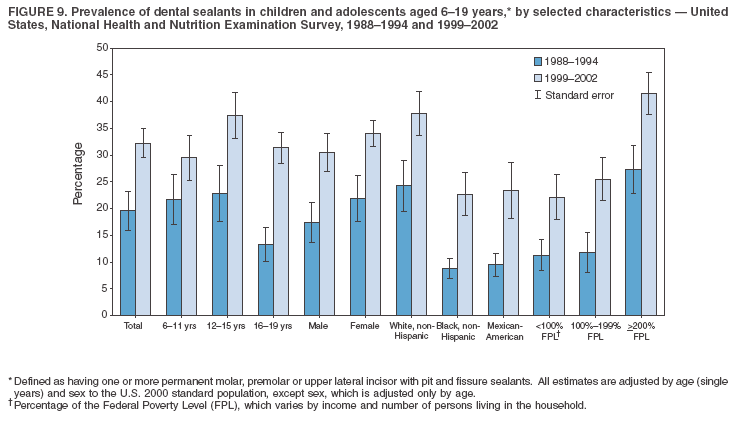 Return to top. Table 10 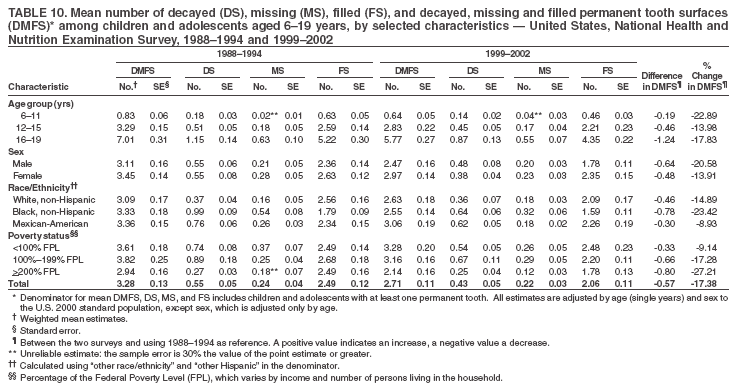 Return to top. Figure 10 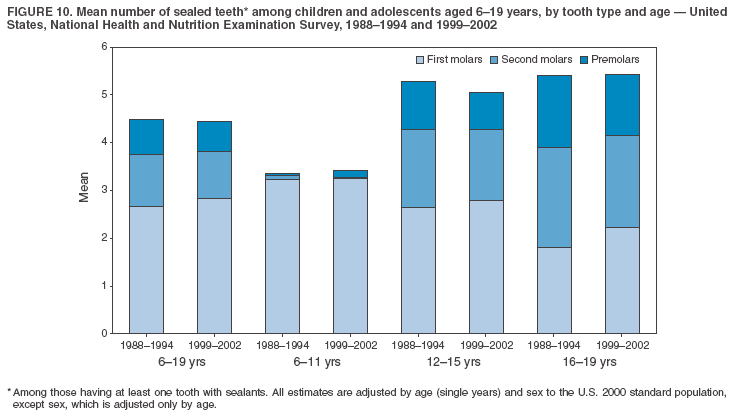 Return to top. Table 11 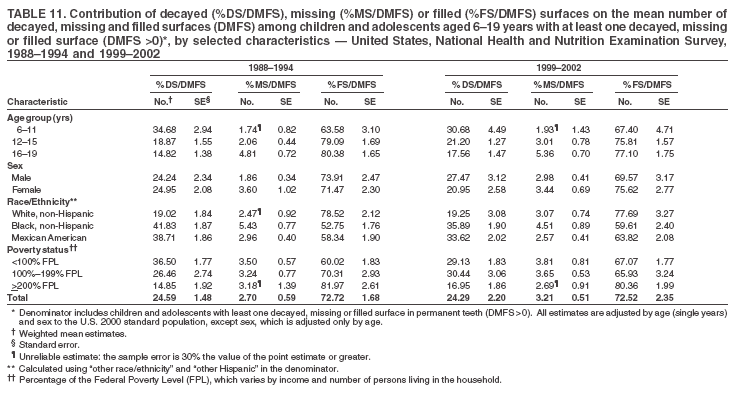 Return to top. Figure 11  Return to top. Table 12 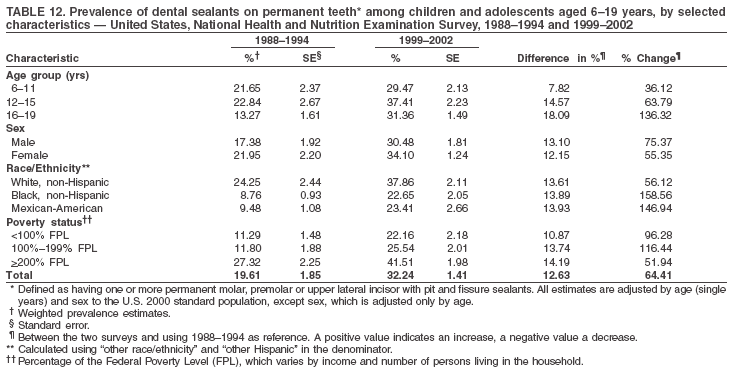 Return to top. Figure 12 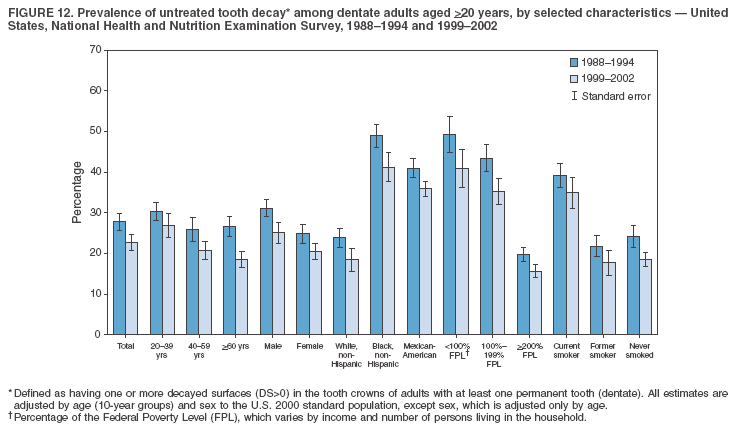 Return to top. Table 13 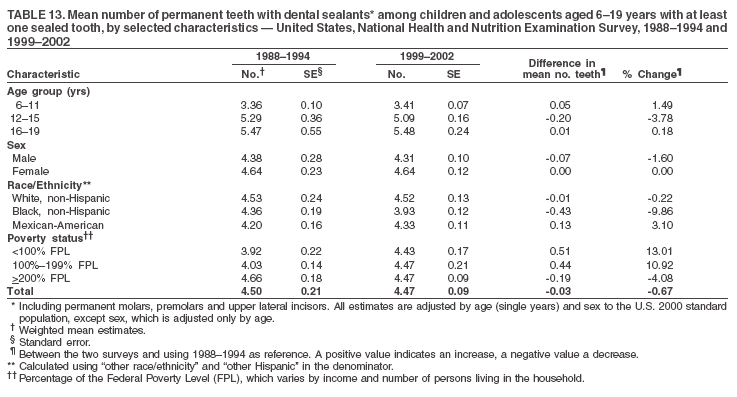 Return to top. Figure 13 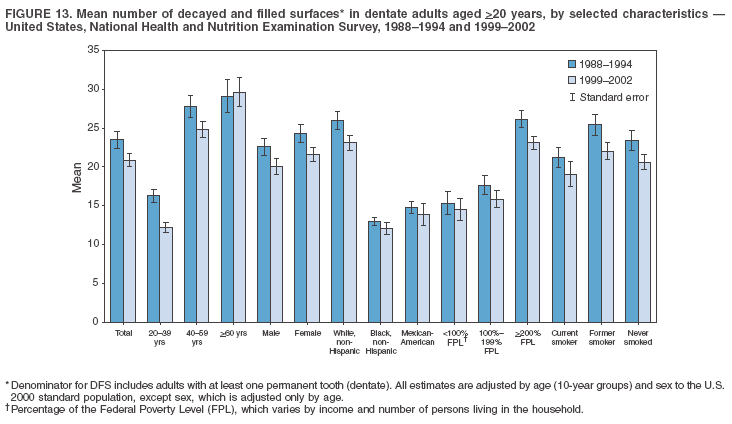 Return to top. Table 14 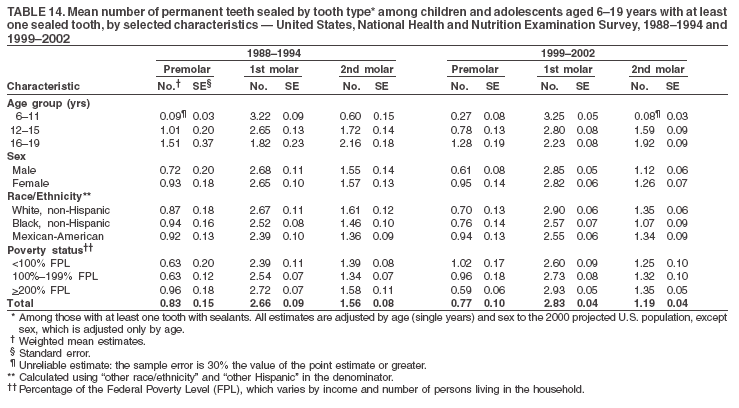 Return to top. Figure 14 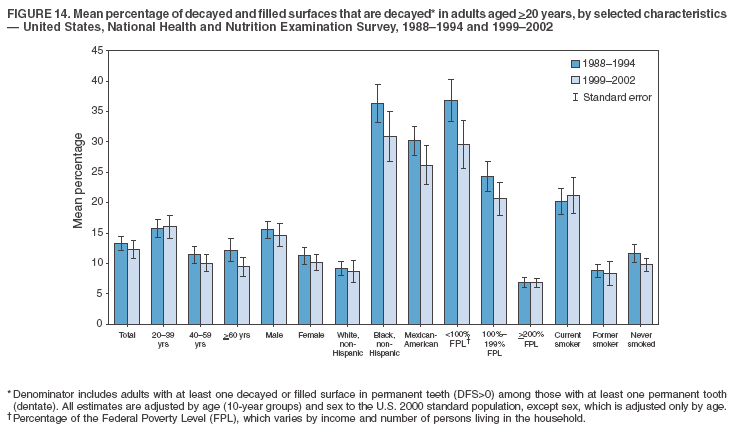 Return to top. Table 15 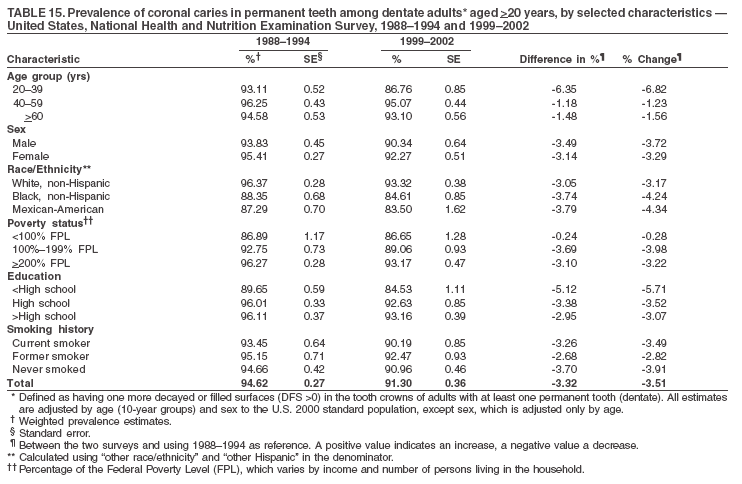 Return to top. Figure 15 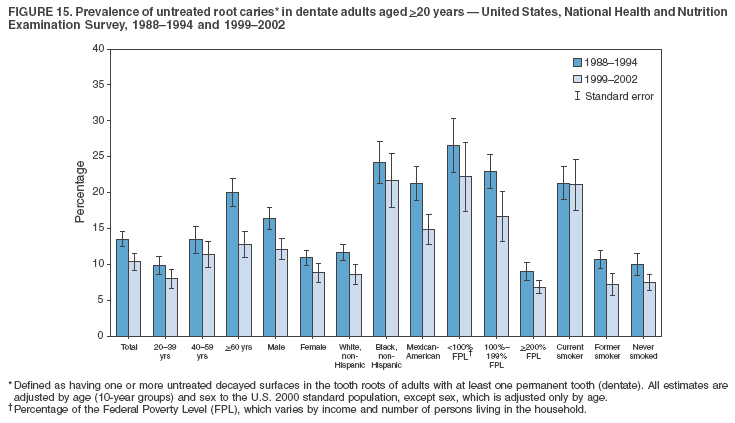 Return to top. Table 16 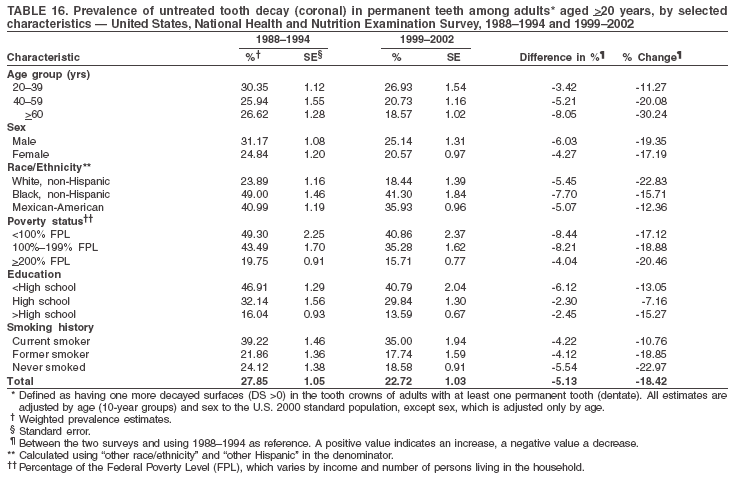 Return to top. Figure 16 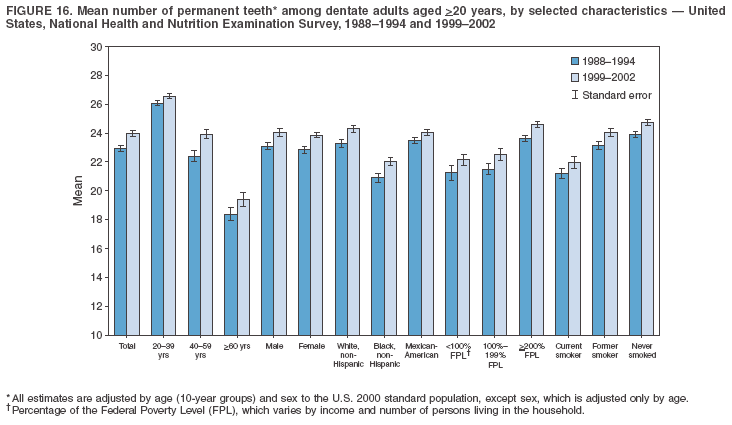 Return to top. Table 17 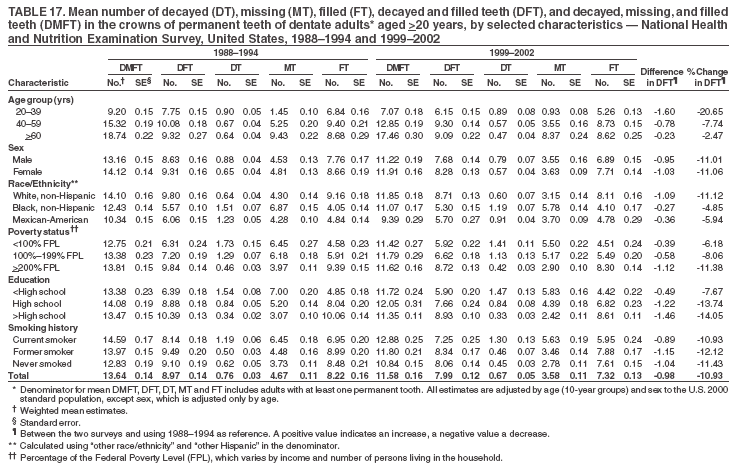 Return to top. Figure 17  Return to top. Table 18 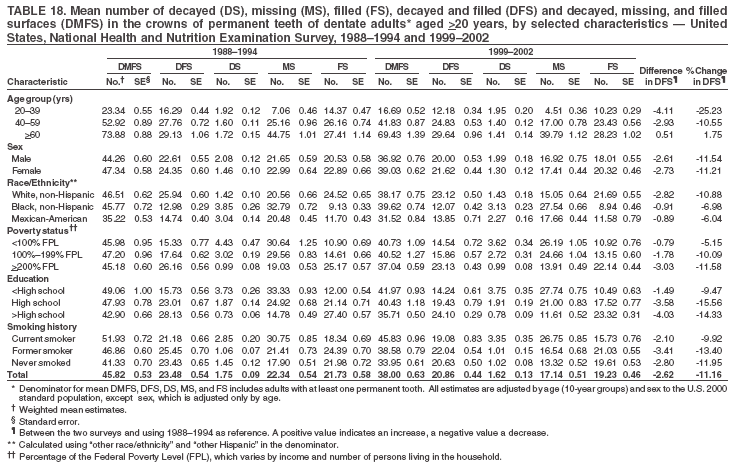 Return to top. Figure 18 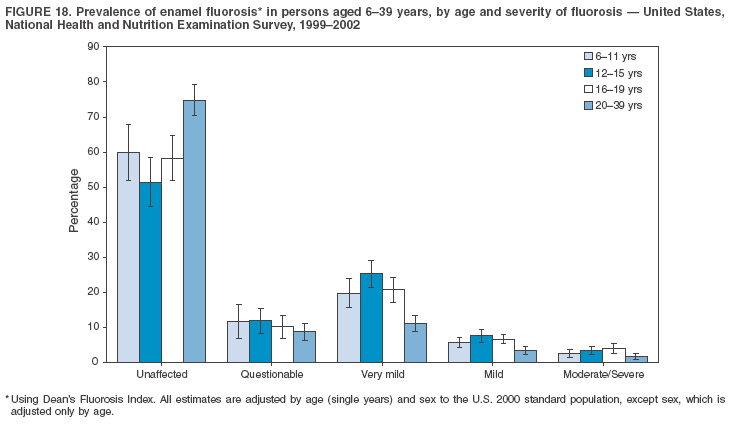 Return to top. Table 19 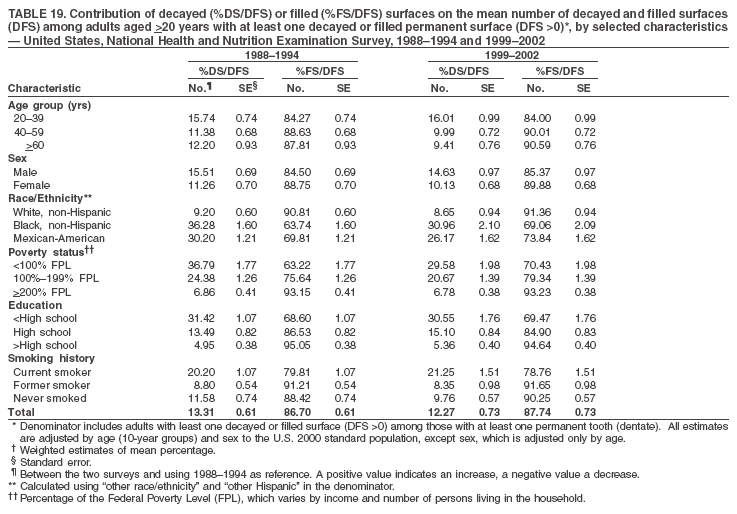 Return to top. Figure 19 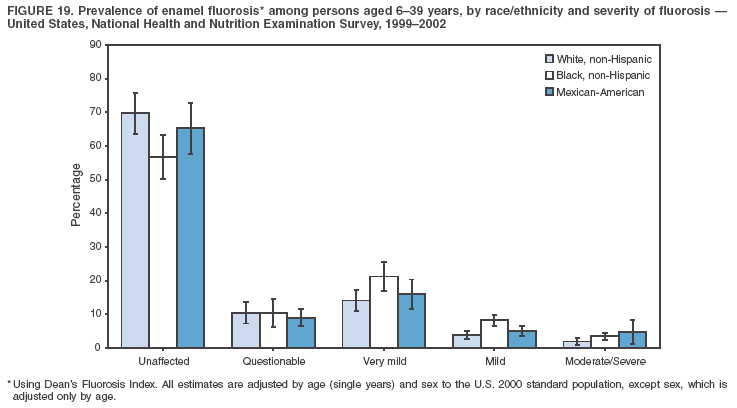 Return to top. Table 20 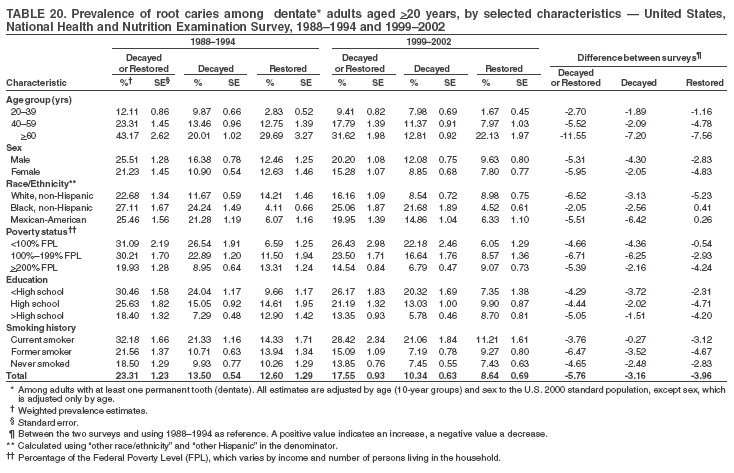 Return to top. Figure 20 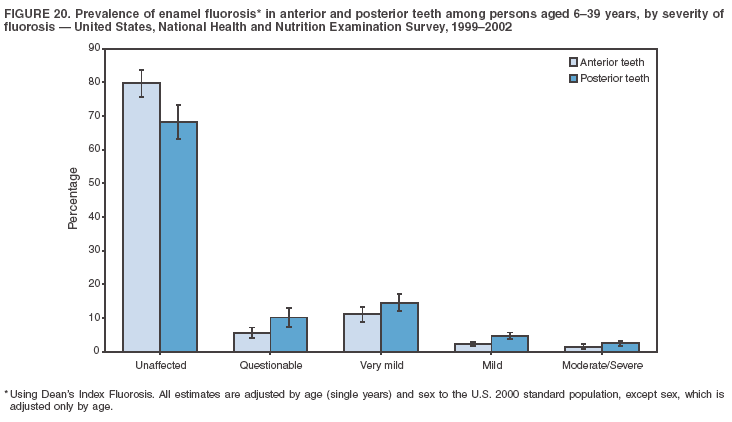 Return to top. Table 21 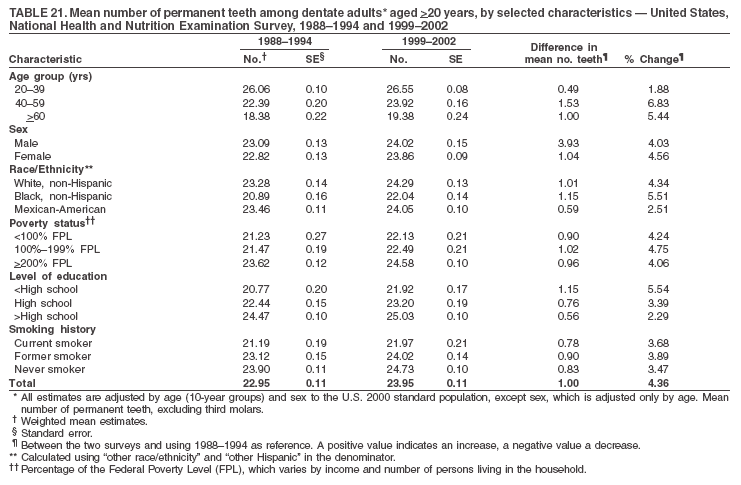 Return to top. Table 22 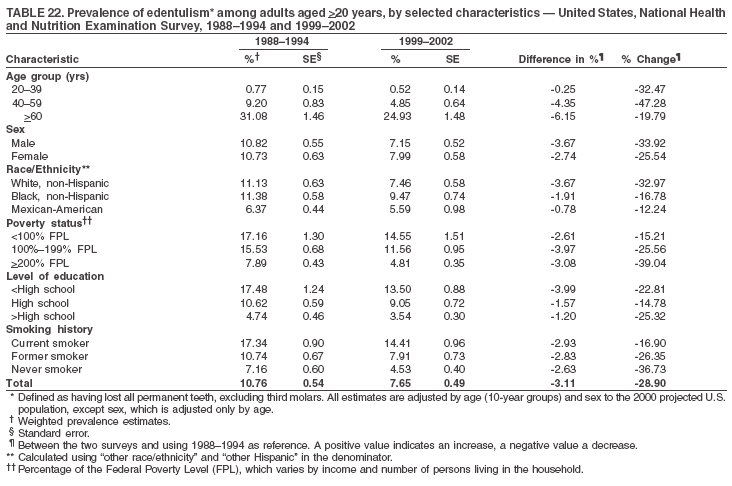 Return to top. Table 23 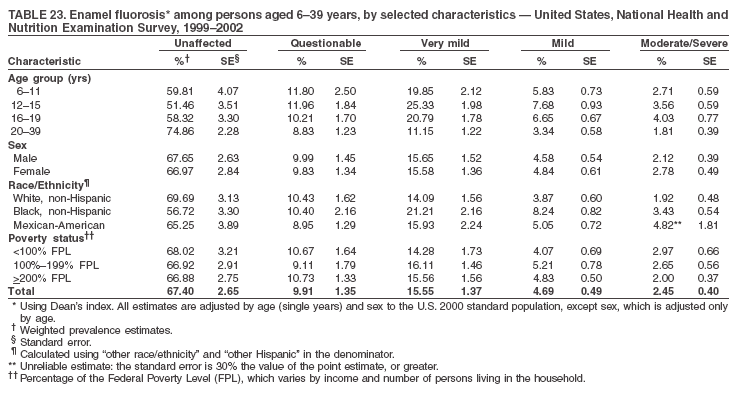 Return to top.
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Date last reviewed: 8/15/2005 |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|