Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail.
Diagnosis and Management
of Foodborne Illnesses
A Primer for Physicians and Other Health
Care Professionals
Produced collaboratively by the
American Medical Association
American Nurses Association--American Nurses Foundation
Centers for Disease Control and Prevention
Center for Food Safety and Applied Nutrition, Food and Drug Administration
Food Safety and Inspection Service, US Department of Agriculture
An earlier edition of this Primer, covering different
foodborne illnesses, was published in
MMWR in 2001 (MMWR 2001;50[No. RR-2]) and also as a separate publication
by the American Medical Association, CDC, the Food and Drug
Administration, and the U.S. Department of Agriculture. This report
updates and supplements the previous edition. It is being reprinted here
as a courtesy to the collaborating agencies and the MMWR readers.
Preface
Foodborne illness is a serious public health problem. CDC estimates
that each year 76 million people get sick, more than 300,000 are
hospitalized, and 5,000 die as a result of foodborne illnesses. Primarily
the very young, the elderly, and the immunocompromised are affected.
Recent changes in human demographics and food preferences, changes in food
production and distribution systems, microbial adaptation, and lack of
support for public health resources and infrastructure have led to the
emergence of novel as well as traditional foodborne diseases. With
increasing travel and trade opportunities, it is not surprising that now
there is a greater risk of contracting and spreading a foodborne illness
locally, regionally, and even globally.
Physicians and other health
care professionals have a critical role in the prevention and control of
food-related disease outbreaks. This primer is intended to provide
practical and concise information on the diagnosis, treatment, and
reporting of foodborne illnesses. It was developed collaboratively by the
American Medical Association, the American Nurses Association-American
Nurse Foundation, CDC, the Food and Drug Administration's Center for Food
Safety and Nutrition, and the United States Department of Agriculture's
Food Safety and Inspection Service.
Clinicians are encouraged to review the primer and participate in the
attached continuing medical education (CME) program.
Background
This primer is directed to primary care and emergency physicians, who
are likely to see the index case of a potential food-related disease
outbreak. It is also a teaching tool to update physicians and other health
care professionals about foodborne illness and remind them of their
important role in recognizing suspicious symptoms, disease clusters, and
etiologic agents, and reporting cases of foodborne illness to public
health authorities.
Specifically, this guide urges physicians and other health care
professionals to
Recognize the potential for a foodborne etiology in a patient's
illness;
Realize that many but not all cases of foodborne illness have
gastrointestinal tract symptoms;
Obtain stool cultures in appropriate settings, and recognize that testing
for some specific pathogens, eg,
E. coli O157:H7, Vibrio spp., must be requested;
Report suspect cases to appropriate public health officials;
Talk with patients about ways to prevent food-related diseases; and
Appreciate that any patient with foodborne illness may represent the
sentinel case of a more widespread outbreak.
Foodborne illness is considered to be any illness that is related to
food ingestion; gastrointestinal tract symptoms are the most common
clinical manifestations of foodborne illnesses. This document provides
detailed summary tables and charts, references, and resources for health
care professionals. Patient scenarios and clinical vignettes are included
for self-evaluation and to reinforce information presented in this primer.
Also included is a CME component.
This primer is not a clinical guideline or definitive resource for the
diagnosis and treatment of foodborne illness. Safe food handling practices
and technologies (eg, irradiation, food processing and storage) also are
not addressed. More detailed information on these topics is available in
the references and resources listed in this document, as well as from
medical specialists and medical specialty societies, state and local
public health authorities, and federal government agencies.
For additional copies, please contact
Litjen (L.J.) Tan, PhD
American Medical Association
515 North State Street
Chicago, Illinois 60610
(312) 464-4147
(312) 464-5841 (fax)
srt@ama-assn.org (e-mail)
Food-related disease threats are numerous and varied, involving
biological and nonbiological agents. Foodborne illnesses can be caused by
microorganisms and their toxins, marine organisms and their toxins, fungi
and their related toxins, and chemical contaminants. During the last 20
years, some foods that have been linked to outbreaks include milk (Campylobacter);
shellfish (noroviruses); unpasteurized apple cider (Escherichia coli
O157:H7), raw and undercooked eggs (Salmonella); fish (ciguatera
poisoning); raspberries (Cyclospora); strawberries (hepatitis A
virus); and ready-to-eat meats (Listeria).
While physicians and other health care professionals have a critical role
in surveillance for and prevention of potential disease outbreaks, only a
fraction of the people who experience gastrointestinal tract symptoms from
foodborne illness seek medical care. In those who do seek care and submit
specimens, bacteria are more likely than other pathogens to be identified
as causative agents. Bacterial agents most often identified in patients
with foodborne illness in the United States are Campylobacter,
Salmonella, and
Shigella species, with substantial variation occurring by geographic area
and season. Testing for viral etiologies of diarrheal disease is rarely
done in clinical practice, but viruses are considered the most common
cause of foodborne illness.
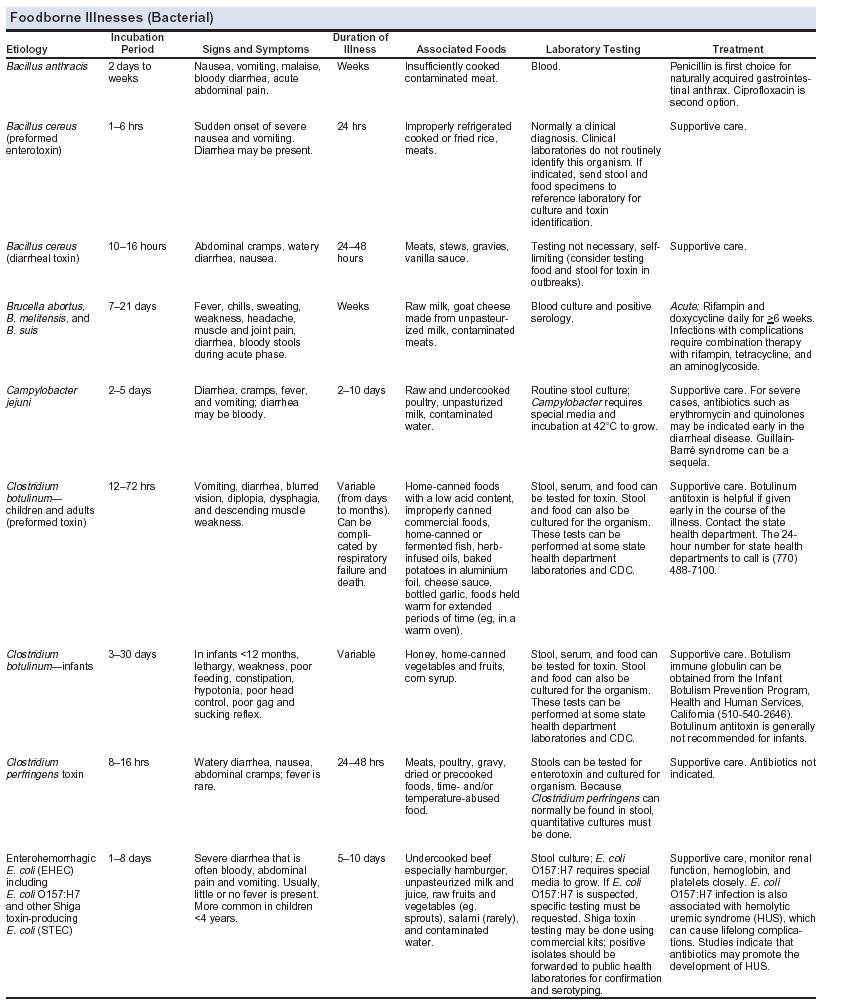
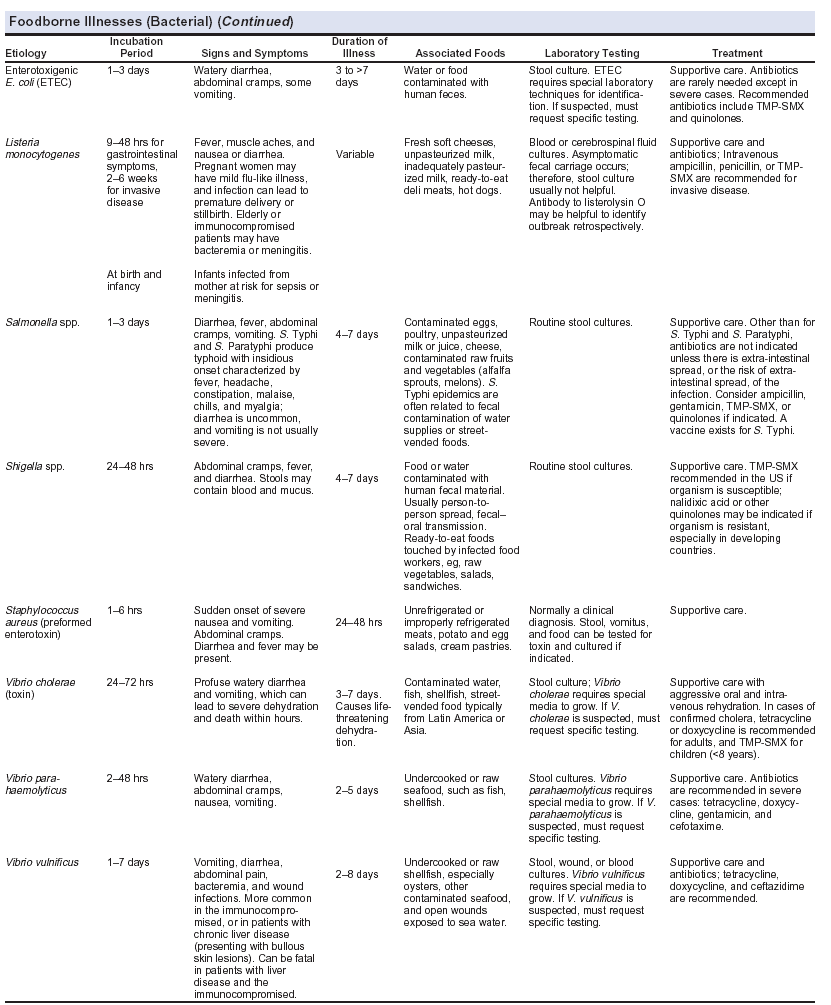
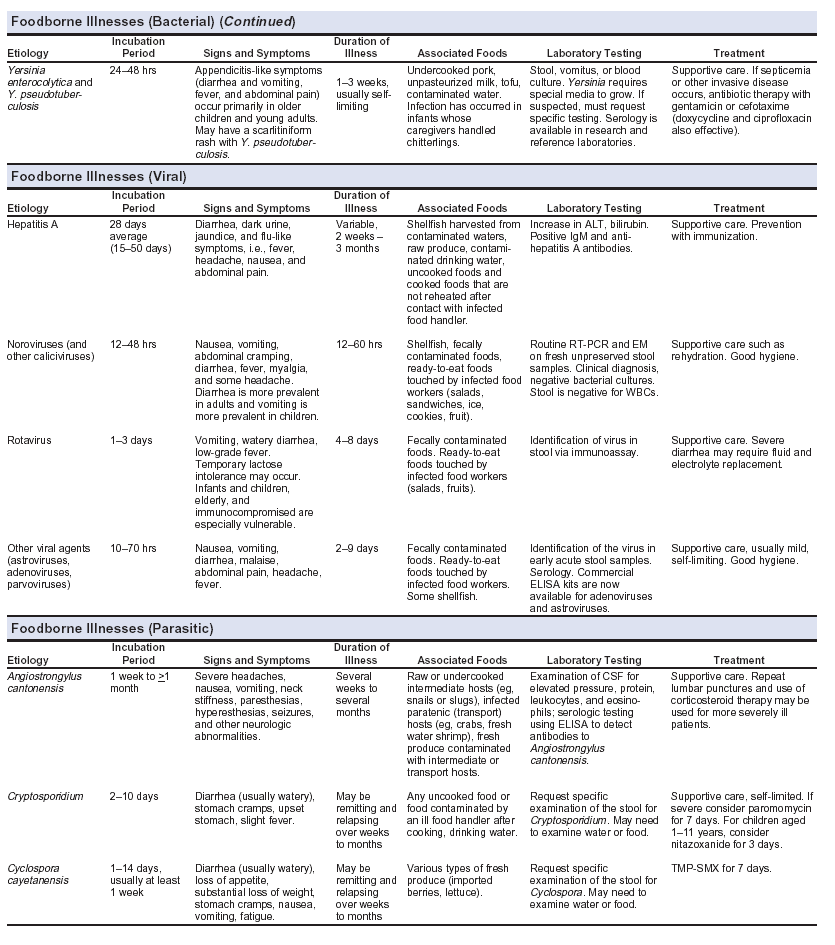
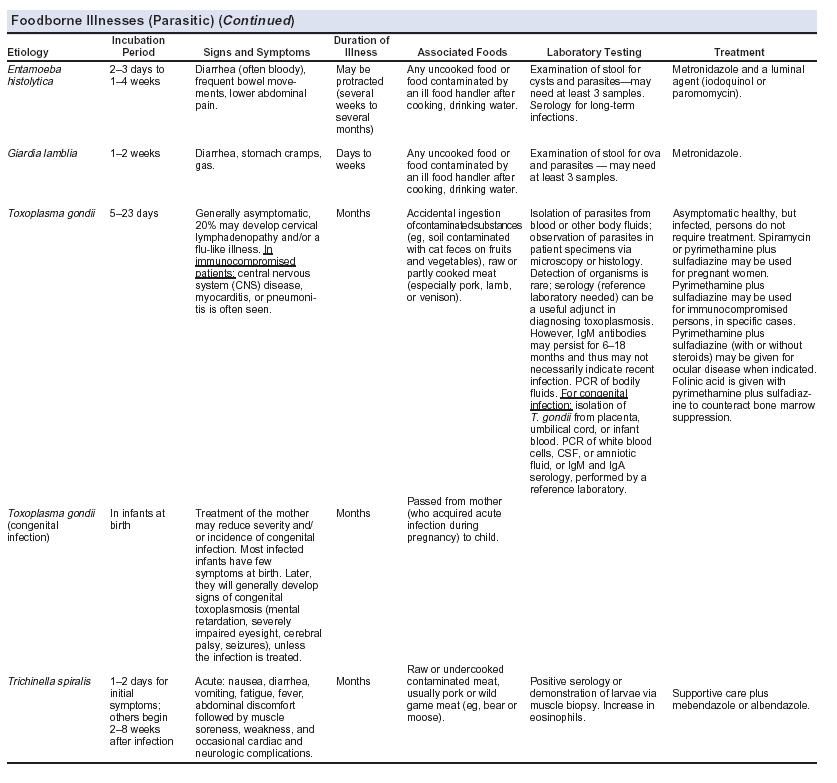
This section and the accompanying Foodborne Illnesses Tables summarize
diagnostic features and laboratory testing for bacterial, viral,
parasitic, and noninfectious causes of foodborne illness. For more
specific guidance, consult an appropriate medical specialist or medical
specialty society, as well as the various resources listed in this primer.
Also refer to this section and the accompanying Foodborne Illnesses Tables
when working through the various Patient Scenarios and the Clinical
Vignettes portion of this primer.
Recognizing Foodborne Illness
Patients with foodborne illnesses typically present with
gastrointestional tract symptoms (eg, vomiting, diarrhea, abdominal pain);
however, nonspecific symptoms and neurologic symptoms may also occur.
Every outbreak begins with an index patient who may not be severely ill. A
physician or health care professional who encounters this person may be
the only one with the opportunity to make an early and expeditious
diagnosis. Thus, the physician or health care professional must have a
high degree of suspicion and ask appropriate questions to recognize that
an illness may have a foodborne etiology.
Important clues to determining the etiology of a foodborne disease are
the
Incubation period;
Duration of the resultant illness;
Predominant clinical symptoms; and
Population involved in the outbreak.
Additional clues may be derived by asking whether the patient has
consumed raw or poorly cooked foods (eg, raw or undercooked eggs, meats,
shellfish, fish), unpasteurized milk or juices, home-canned goods, fresh
produce, or soft cheeses made from unpasteurized milk. Inquire as to
whether any of the patient's family members or close friends have similar
symptoms. Inquiries about living on or visiting a farm, pet contact, day
care attendance, occupation, foreign travel, travel to coastal areas,
camping excursions to mountains or other areas where untreated water is
consumed, and attendance at group picnics or similar outings also may
provide clues for determining the etiology of the illness.
If a foodborne illness is suspected, submit appropriate specimens for
laboratory testing and contact the state or local health department for
advice about epidemiologic investigation. For the physician or other
health care professional, implication of a specific source in disease
transmission is difficult from a single patient encounter. Attempts to
identify the source of the outbreak are best left to public health
authorities.
Because infectious diarrhea can be contagious and is easily spread, rapid
and definitive identification of an etiologic agent may help control a
disease outbreak. Early identification of a case of foodborne illness can
prevent further exposures. An individual physician who obtains testing can
contribute the clue that ultimately leads to identification of the source
of an outbreak.
Finally, health care professionals should recognize
that while deliberate contamination of food is a rare event, it has been
documented in the past. The following events may suggest that intentional
contamination has occurred: an unusual agent or pathogen in a common food,
a common agent or pathogen affecting an unusually large number of people,
or a common agent or pathogen that is uncommonly seen in clinical
practice, as might occur with pesticide poisoning.
Diagnosing Foodborne Illnesses
Differential Diagnosis
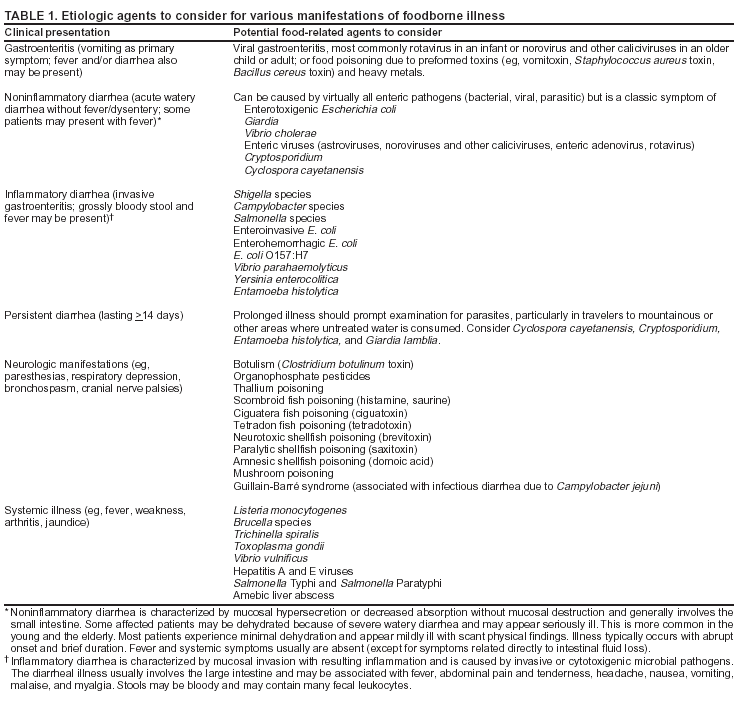
As shown in Table 1 and the Foodborne Illnesses
Tables, a variety of infectious and noninfectious agents should be
considered in patients suspected of having a foodborne illness.
Establishing a diagnosis can be difficult, however, particularly in
patients with persistent or chronic diarrhea, those with severe abdominal
pain, and when there is an underlying disease process. The extent of
diagnostic evaluation depends on the clinical picture, the differential
diagnosis considered, and clinical judgment.
The presentation of a patient with a foodborne illness is often only
slightly different from that of a patient who presents with a viral
syndrome. In addition, viral syndromes are so common that it is reasonable
to assume that a percentage of those diagnosed with a viral syndrome have
actually contracted a foodborne illness. Therefore, the viral syndrome
must be excluded in order to suspect the foodborne illness and take
appropriate public health action. Fever, diarrhea, and abdominal cramps
can be present or absent in both cases so they are not very helpful. The
absence of myalgias or arthralgias would make a viral syndrome less likely
and a foodborne illness (that does not target the neurologic system) more
likely. Foodborne illnesses that do target the neurologic system tend to
cause paraesthesias, weakness and paralysis that are distinguishable from
myalgias or arthralgias (see below). The presence of dysentery (bloody
diarrhea) is also more indicative of a foodborne illness, particularly if
it is early in the course.
If any of the following signs and symptoms occur in patients, either
alone or in combination, laboratory testing may provide important
diagnostic clues (particular attention should be given to very young and
elderly patients and to immunocompromised patients, all of whom are more
vulnerable):
Bloody diarrhea
Weight loss
Diarrhea leading to dehydration
Fever
Prolonged diarrhea (3 or more unformed stools per day, persisting several
days)
Neurologic involvement, such as paresthesias, motor weakness, cranial
nerve palsies
Sudden onset of nausea, vomiting, diarrhea
Severe abdominal pain
In addition to foodborne causes, a differential diagnosis of
gastrointestinal tract disease should include underlying medical
conditions such as irritable bowel syndrome; inflammatory bowel diseases
such as Crohn's disease or ulcerative colitis; malignancy; medication use
(including antibiotic-related
Clostridium difficile toxin colitis); gastrointestinal tract surgery or
radiation; malabsorption syndromes; immune deficiencies; and numerous
other structural, functional, and metabolic etiologies. Consideration also
should be given to exogenous factors such as the association of the
illness with travel, occupation, emotional stress, sexual habits, exposure
to other ill persons, recent hospitalization, child care center
attendance, and nursing home residence.
The differential diagnosis of patients presenting with neurologic
symptoms due to a foodborne illness is also complex. Possible food-related
causes to consider include recent ingestion of contaminated seafood,
mushroom poisoning, and chemical poisoning. Because the ingestion of
certain toxins (eg, botulinum toxin, tetrodotoxin) and chemicals (eg,
organophosphates) can be life-threatening, a differential diagnosis must
be made quickly with concern for aggressive therapy and life support
measures (eg, respiratory support, administration of antitoxin or
atropine), and possible hospital admission.
Clinical Microbiology Testing
When submitting specimens for microbiologic testing, it is important
to realize that clinical microbiology laboratories differ in protocols
used for the detection of pathogens. To optimize recovery of an etiologic
agent, physicians and other health care professionals should understand
routine specimen-collection and testing procedures as well as
circumstances and procedures for making special test requests. Some
complex tests (eg, toxin testing, serotyping, molecular techniques) may
only be available from large commercial or public health laboratories.
Contact your microbiology laboratory for more information.
Stool cultures are indicated if the patient is immunocompromised,
febrile, has bloody diarrhea, has severe abdominal pain, or if the illness
is clinically severe or persistent. Stool cultures are also recommended if
many fecal leukocytes are present. This indicates diffuse colonic
inflammation and is suggestive of invasive bacterial pathogens such as
Shigella, Salmonella, and
Campylobacter species and invasive E. coli. In most laboratories,
routine stool cultures are limited to screening for Salmonella and
Shigella species and
Campylobacter jejuni/coli. Cultures for Vibrio and Yersinia
species, E. coli O157:H7, and Campylobacter species other
than
jejuni/coli require additional media or incubation conditions and
therefore require advance notification or communication with laboratory
and infectious disease personnel.
Stool examination for parasites generally is indicated for patients with
suggestive travel histories, who are immunocompromised, who suffer chronic
or persistent diarrhea, or when the diarrheal illness is unresponsive to
appropriate antimicrobial therapy. Stool examination for parasites is also
indicated for gastrointestinal tract illnesses that appear to have a long
incubation period. Requests for ova and parasite examination of a stool
specimen will often enable identification of Giardia lamblia and
Entamoeba histolytica, but a special request may be needed for
detection of
Cryptosporidium and Cyclospora cayetanensis. Each laboratory may
vary in its routine procedures for detecting parasites, so it is important
to contact your laboratory.
Blood cultures should be obtained when bacteremia or systemic infection
is suspected.
Direct antigen detection tests and molecular biology techniques are
available for rapid identification of certain bacterial, viral, and
parasitic agents in clinical specimens. In some circumstances,
microbiologic and chemical laboratory testing of vomitus or implicated
food items also is warranted. For more information on laboratory
procedures for the detection of foodborne pathogens, consult an
appropriate medical specialist, clinical microbiologist, or state public
health laboratory.
Treating Foodborne Illness
Selection of appropriate treatment depends on identification of the
responsible pathogen (if possible) and determining if specific therapy is
available. Many episodes of acute gastroenteritis are self-limiting and
require fluid replacement and supportive care. Oral rehydration is
indicated for patients who are mildly to moderately dehydrated;
intravenous therapy may be required for more severe dehydration. Routine
use of antidiarrheal agents is not recommended because many of these
agents have potentially serious adverse effects in infants and young
children.
Choice of antimicrobial therapy should be based on
Clinical signs and symptoms;
Organism detected in clinical specimens;
Antimicrobial susceptibility tests; and
Appropriateness of treating with an antibiotic (some enteric bacterial
infections are best not treated).
Knowledge of the infectious agent and its antimicrobial
susceptibility pattern allows the physician to initiate, change, or
discontinue antimicrobial therapy. Such information also can support
public health surveillance of infectious disease and antimicrobial
resistance trends in the community. Antimicrobial resistance has increased
for some enteric pathogens, which dictates judicious use of this therapy.
Suspected cases of botulism are treated with botulinum antitoxin. Equine
botulinum antitoxin for types A, B, and E can prevent the progression of
neurologic dysfunction if administered early in the course of illness.
Physicians and other health care professionals should notify their local
and state health departments regarding suspected cases of botulism. CDC
maintains a 24-hour consultation service to assist health care
professionals with the diagnosis and management of this rare disease.
Surveillance and Reporting of Foodborne Illness
Reporting of foodborne illnesses in the United States began more than
50 years ago when state health officers, concerned about the high
morbidity and mortality caused by typhoid fever and infantile diarrhea,
recommended that cases of "enteric fever" be investigated and reported.
The intent of investigating and reporting these cases was to obtain
information about the role of food, milk, and water in outbreaks of
gastrointestinal tract illness as the basis for public health actions.
These early reporting efforts led to the enactment of important public
health measures (eg, the Pasteurized Milk Ordinance) that profoundly
decreased the incidence of foodborne illnesses.
Often health care professionals may suspect foodborne illness either
because of the organism involved or because of other available
information, such as several ill patients who have eaten the same food.
Health care professionals can serve as the eyes and ears for the health
department by providing such information to local or state public health
authorities. Foodborne disease reporting is not only important for disease
prevention and control, but more accurate assessments of the burden of
foodborne illness in the community occur when physicians and other health
care professionals report foodborne illnesses to the local and state
health department. In addition, reporting of cases of foodborne illness by
practicing physicians to the local health department may help the health
officer identify a foodborne disease outbreak in the community. This may
lead to early identification and removal of contaminated products from the
commercial market. If a restaurant or other food service establishment is
identified as the source of the outbreak, health officers will work to
correct inadequate food preparation practices, if necessary. If the home
is the likely source of the contamination, health officers can institute
public education about proper food handling practices. Occasionally,
reporting may lead to the identification of a previously unrecognized
agent of foodborne illness. Reporting also may lead to identification and
appropriate management of human carriers of known foodborne pathogens,
especially those with high-risk occupations for disease transmission such
as foodworkers.
Table 2 lists current reporting requirements for
foodborne diseases and conditions in the United States. National reporting
requirements are determined collaboratively by the Council of State and
Territorial Epidemiologists and CDC. Additional reporting requirements may also
be mandated by state and territorial laws and regulations. Details on specific
state reporting requirements are available from state health departments and
from the Council of State and Territorial Epidemiologists and CDC.
Typically, the appropriate procedure for health care professionals to
follow in reporting foodborne illnesses is to contact the local or state
health department whenever they identify a specific notifiable foodborne
disease. However, it is often unclear if a patient has a foodborne illness
prior to diagnostic tests, so health care professionals should also report
potential foodborne illnesses, such as when 2 or more patients present
with a similar illness that may have resulted from the ingestion of a
common food. Local health departments then report the illnesses to the
state health departments and determine if further investigation is
warranted.
Each state health department reports foodborne illnesses to CDC. CDC
compiles these data nationally and disseminates information via the weekly
Morbidity and Mortality Weekly Report and annual summary reports. CDC
assists state and local public health authorities with epidemiologic
investigations and the design of interventions to prevent and control
food-related outbreaks. CDC also coordinates a national network of public
health laboratories, called PulseNet, which performs "molecular
fingerprinting" of bacteria (by pulsed-field gel electrophoresis) to
support epidemiologic investigations.
Thus, in addition to
reporting cases of potential foodborne illnesses, it is important for
physicians to report noticeable increases in unusual illnesses, symptom
complexes, or disease patterns (even without definitive diagnosis) to
public health authorities. Prompt reporting of unusual patterns of
diarrheal/gastrointestinal tract illness, for example, can allow public
health officials to initiate an epidemiologic investigation earlier than
would be possible if the report awaited definitive etiologic diagnosis.
Finally, new information on food safety is constantly emerging.
Recommendations and precautions for people at high risk are updated
whenever new data about preventing foodborne illness become available.
Physicians and other health care professionals need to be aware of and
follow the most current information on food safety.
Patient Scenarios
The learning scenarios in this section can be used to reinforce
medical management information pertaining to foodborne illnesses, such as
that provided from the previous sections of this primer. The case studies
provide questions that need to be considered when dealing with a potential
case of foodborne illness. Answers are provided immediately following the
questions to enhance the learning process.
Similar learning scenarios are also available for other foodborne
pathogens.
Congenital Toxoplasmosis, A Patient Scenario
Susan, a 6-month-old infant, is brought to your office for evaluation
of apparent blindness. Her mother reports that she had been well during
the pregnancy and the delivery was uncomplicated. The baby appeared
healthy until age 4 months, when the parents became concerned about her
vision.
Physical examination was normal except for bilateral macular scars,
microphthalmos, and unresponsiveness to visual stimuli. There were no
other neurologic abnormalities, and her growth and development were
appropriate for her age. A computed tomography (CT) scan of the head was
obtained.
Congenital infection with which of the following should be included in the
differential diagnosis?
What additional information would assist with the diagnosis?
More history from the mother, including travel to foreign
country
Vaccination record, including during pregnancy
History of exposure to cats and raw meat
History of multiple sex partners and sexually transmitted disease (STD)
History of herpes
Evaluation of CT scan
The CT scan of the child's head showed periventricular
calcifications and asymmetric dilation of the lateral ventricles. The
mother is 35 years old and reiterated that she does not recall being ill
during the pregnancy; however, she also indicated that she would not
necessarily remember every little symptom. She also denied having a
history of STDs. She had received the mumps-measles-rubella (MMR) vaccine
as a child but no vaccines during pregnancy. The mother recalled eating
insufficiently cooked meat while traveling in France during the first
trimester of pregnancy. The family does not own a cat, and she does not
recall having been exposed to cats during her pregnancy.
What diagnostic tests are needed?
Serologic
evaluation of both mother and child focusing on potential congenital
infection (ie, a ToRCH profile) based on the history of the mother ingesting
raw meat while traveling in a foreign country during first trimester of
pregnancy and the clinical findings (blindness, cerebral calcifications, and
hydrocephalus).
Results of serologic testing detected both IgG and IgM antibodies to
Toxoplasma gondii in both the baby's and mother's serum. The mother's IgM
titer was 1:6400 and IgG titer was 1:6400, while those of the baby were
IgM titer of 1:160 and IgG titer of 1:6400.
How does this information assist with the diagnosis?
Diagnosis of
toxoplasmosis is usually confirmed by serologic tests. Occasionally, organisms
are identified in tissue or body fluids or isolated by culture or animal
inoculation. Polymerase chain reaction (PCR)-based assays are available from
some laboratories for diagnosis of fetal infection and infection in compromised
hosts. For immunocompetent persons, seroconversion or a 4-fold rise of specific
IgG antibodies or demonstration of specific IgM antibodies indicate recent
infection. High titers of IgG antibodies in the absence of IgM antibodies are
consistent with chronic latent infection acquired in the past. The IgM-capture
enzyme-linked immunosorbent assay (ELISA) is more sensitive than the IgM-indirect
fluorescent-antibody assay (IFA) test. However, IgM tests may be false-positive,
and true-positive IgM tests may persist for a year or more. Therefore, to
determine if infection occurred during pregnancy, additional tests, such as an
anti-Toxoplasma avidity test, may be required at a reference laboratory.
Immunodeficient persons usually do not have measurable IgM antibodies, even in
the presence of active disease. The diagnosis of central nervous system (CNS)
toxoplasmosis in such persons is therefore based on clinical picture, typical CT
scan or magnetic resonance imaging (MRI) showing multiple ring-enhancing
hypodense nodules, and a positive IgG test. Brain biopsy is reserved for cases
that fail to respond to an empiric trial of anti-Toxoplasma drugs.
The baby was diagnosed with congenital toxoplasmosis.
How is toxoplasmosis best treated?
Toxoplasmosis
in immunocompetent persons rarely requires treatment, whereas infection in
immunodeficient persons or in infants with congenital infections usually
requires treatment. The combination of pyrimethamine and sulfadiazine is the
treatment of choice. Folinic acid (leucovorin) is given to prevent bone
marrow suppression. Treatment must be continued for the duration of
immunosuppression and for life in AIDS patients whose immunity is not
reconstituted by highly aggressive antiretroviral therapy (HAART).
For persons unable to tolerate the pyrimethamine and sulfadiazine
combination, high doses of pyrimethamine (and leucovorin) and clindamycin
are effective.
The management of toxoplasmosis acquired during pregnancy is
controversial. Testing of newly pregnant women for
T. gondii infection is not routinely done, and routine testing is not
recommended by CDC or by the American College of Obstetricians and
Gynecologists. To prevent fetal infection, one approach is to administer
spiramycin (a macrolide antibiotic, which is concentrated in the placenta
and is not harmful to the fetus). At the same time, amniotic fluid is
submitted for PCR-based testing to determine whether fetal infection has
occurred. If so, options may include pyrimethamine and sulfadiazine given
after the 16th week of pregnancy (since pyrimethamine is potentially
teratogenic) or consideration of terminating the pregnancy. If the fetus is
shown to be uninfected, spiramycin is continued throughout pregnancy.
Different protocols exist for treatment of infants born with congenital
infection. The most commonly recommended treatment is pyrimethamine and
sulfadiazine plus leucovorin during the first year of life. In the present
case, the child was treated for 6 months with pyrimethamine and sulfadiazine
plus leucovorin.
Human infection with the intracellular protozoan parasite
Toxoplasma gondii occurs globally. Infection is usually subclinical or
produces a mild illness, except in immunodeficient persons and fetuses
infected in utero. Most infants with congenital toxoplasmosis appear
healthy at birth but have a high incidence of developing serious
ophthalmologic and neurologic sequelae during the next 20 years of life.
Severe congenital toxoplasmosis may be apparent at birth or become
apparent during the first 6 months of life. Chorioretinitis, intracerebral
calcifications, and hydrocephalus, as in the present case, are typical
features
The child was treated with pyrimethamine, sulfadiazine,
and folinic acid for 6 months. She remains blind, and has developed
moderate psychomotor retardation.
How could Toxoplasma infection have been prevented in this child?
Toxoplasma gondii may be transmitted transplacentally to the fetus if the
mother acquired toxoplasmosis during pregnancy. There is almost no risk of
transplacental transmission if the mother was infected prior to conception;
accordingly, women with positive IgG antibody tests for toxoplasmosis at the
onset of pregnancy are not at risk for developing acute toxoplasmosis. Women
with negative IgG antibody tests during pregnancy should avoid eating
insufficiently cooked or uncooked meat and should avoid ingestion of soil and
water or food that may be contaminated with cat feces.
Transmission occurs by a) ingestion of tissue cysts in raw or
insufficiently cooked meat, especially lamb, pork, and wild game; b) accidental
ingestion of food, water, or soil contaminated with cat feces that contain
infective oocysts; c) transplacental passage of infective tachyzoites; d)
transfusion of infected white blood cells or transplantation of an infected
organ; and e) laboratory accidents.
Prevention of toxoplasmosis is particularly important for uninfected (ie,
seronegative) pregnant mothers, HIV-infected persons, and other
immunocompromised patients:
Avoid ingestion of raw or insufficiently cooked meat and poultry; cook meat to
160°F (71°C) or freeze to -4°F (-20°C). For more details on preventing
toxoplasmosis, please see the Suggested Resources and Suggested Reading List.
Avoid ingestion of environmental oocysts by avoiding contact with cat litter,
soil, water, and vegetables potentially contaminated with cat feces.
Infection acquired by healthy persons is usually asymptomatic or may
lead to painless lymphadenopathy or a mononucleosis syndrome. Maternal
infection is usually unrecognized.
Disease in persons with depressed cellular immunity (eg, persons with
AIDS, transplant recipients, persons receiving immunosuppressants) usually
is due to reactivation of latent infection but can result from acute
infection. Toxoplasmosis in these persons leads to lethal
meningoencephalitis, focal lesions of the CNS, and less commonly,
myocarditis or pneumonitis. The clinical picture may include headache,
seizures, mental status changes, focal neurologic signs, and aseptic
meningitis. Thirty to forty percent of AIDS patients with IgG antibodies
to
T. gondii (indicating chronic latent infection) develop active
toxoplasmosis unless they take preventive medication.
Congenital infection occurs when a previously uninfected mother develops
infection during pregnancy. Infection prior to conception, demonstrated by
specific IgG antibodies, in nearly all cases guarantees against infection
of the fetus. However, transplacental transmission occurs from mothers
whose prior infections reactivate when they receive immunosuppressant
medications or develop AIDS. Congenital toxoplasmosis may result in
abortion, stillbirth, mental retardation, and retinal damage. Recurrent
toxoplasmic chorioretinitis in children and young adults is frequently the
result of congenital infection that was asymptomatic at birth.
Acute Hepatitis A: A Patient Scenario
While working in an emergency room, you are asked to see a
31-year-old Asian-American woman who has had fever, nausea, and fatigue
for the past 24 hours. She also reports dark urine and has had 3 light
colored stools since yesterday. She has previously been healthy and has no
previous history of jaundice. Her physical examination shows a low-grade
fever of 100.6°F/38.1°C, faint scleral icterus, and hepatomegaly. Her
blood pressure and neurologic exam are normal and there is no rash.
Initial laboratory studies show an alanine aminotransferase (ALT) result
of 877 IU/L, aspartate amino transferase (AST) enzyme levels of 650 IU/L,
an alkaline phosphatase of 58 IU/L and a total bilirubin of 3.4 mg/dL.
White blood cell count is 4.6, with a normal differential; electrolytes
are normal; the blood urea nitrogen level is 18 mg/dL; and serum
creatinine level is 0.6 mg/dL. Pregnancy test is negative.
What should be included in the differential diagnosis of acute hepatitis?
Viral infections:
--- hepatitis A, B, C, D, and E
--- varicella
--- cytomegalovirus
--- herpes virus
--- Epstein-Barr virus
What additional information would assist with the diagnosis?
Has she traveled outside the United States recently?
Does she use illicit drugs?
Is anyone else in the household ill?
How many sex partners has she had in the past 6 months?
Does she have regular contact with animals?
What medications is she taking?
Has she ever had a transfusion?
Does she drink alcohol?
Does she take care of children?
Has she ever received hepatitis B vaccination?
Has she ever received hepatitis A vaccination?
Did she receive immune globulin within the past 3 months?
What is her occupation?
She has no children, and her boyfriend is not ill. She has been in a
monogamous relationship with her boyfriend for 2 years. She was born in
the United States; her parents immigrated to the United States from Taiwan
in the 1950s. She works as a food preparer for a catering business. She
returned 4 weeks ago from a 1-week vacation in Mexico (Mexico City and
nearby areas), where she stayed with her boyfriend in several hotels. She
drank only bottled water but ate both cooked and uncooked food at numerous
restaurants while in Mexico, and she visited a family friend and her 3
young children in a Mexico City suburb.
She did not receive hepatitis A vaccine or immune globulin before going
on vacation. She is not sure if she has received hepatitis B vaccine. She
has not gone camping or hiking and had no recent tick exposures. She has
never used illicit drugs, drinks alcohol rarely, and has never received a
transfusion. She is taking oral contraceptives but no other prescription
medication, and took 500 milligrams of Tylenol® once after
onset of her current symptoms. She has a pet cat but no other animal
exposures. She had chickenpox and mononucleosis during childhood.
How does this information assist with the diagnosis?
Lack of
animal or tick exposures makes leptospirosis and Rocky Mountain spotted fever
unlikely, and Q fever less likely. Yellow fever and typhoid fever are very
unlikely with no history of travel to rural endemic areas, and assuming exposure
occurred in Mexico, inconsistent with the long incubation period. Hepatitis A
virus (HAV), hepatitis B virus (HBV), hepatitis C virus (HCV), and hepatitis E
virus (HEV) infection are all possible diagnoses. A drug reaction to the oral
contraceptive is a possible cause of hepatitis. The history of travel to an
endemic area makes hepatitis A the most likely diagnosis.
What diagnostic tests are needed?
Specific diagnostic serologic
studies are necessary to distinguish one form of viral hepatitis from another.
Testing for total (IgG+ IgM) anti-HAV does not distinguish between a past
history of hepatitis A virus infection and current infection and is not useful
in diagnosing acute hepatitis A. Hepatitis A can be easily confirmed with an
anti-IgM anti-HAV test. This test is widely available and results are usually
available within 24 hours. A hepatitis panel is ordered, and results from such a
panel are shown here.
You obtain the following results from the serologic testing:
Total anti-HAV: positive
IgM anti-HAV: positive
Total anti-HBc: positive
IgM anti-hepatitis B core antigen: negative
HBsAg: negative
anti-HBs: positive
anti-HCV: negative
What is the diagnosis?
The diagnosis is hepatitis A. The
hepatitis B serologic tests indicate past, resolved infection with no chronic
infection. Acute hepatitis C is also possible; the appearance of anti-HCV may be
delayed for as long as 9 months after exposure. However, with a confirmed
diagnosis of hepatitis A, further testing for HCV RNA is not indicated at this
point. Finally, note that hepatitis E is rarely reported in travelers, and
results of serologic tests for hepatitis E virus (HEV) are difficult to
interpret. Tests for HEV should only be performed if other more common causes of
hepatitis have been excluded.
The incubation period for hepatitis A is 15--50 days, with an average
of 28 days. The most common signs and symptoms associated with acute
hepatitis A include jaundice, fever, malaise, anorexia, and abdominal
discomfort. The illness can be severe and approximately 10% to 20% of
reported cases require hospitalization. The likelihood of having symptoms
with HAV infection is related to the person's age. In children <6 years of
age, most (70%) infection is asymptomatic; if illness does occur it is not
usually accompanied by jaundice. Older children and adults are more likely
to have symptomatic disease, although jaundice may be absent in as many as
one third of adults with HAV infection. In many developing countries in
Asia, Africa, and Central and South America, infection is nearly universal
during early childhood and is often asymptomatic.
What treatment is indicated?
There is no specific treatment
for hepatitis A. Bed rest does not hasten recovery. Hepatitis A is never a
chronic infection, although 10% to 15% of symptomatic persons have prolonged or
relapsing disease lasting up to 6 months. While rarely fatal in younger persons,
the case-fatality rate is nearly 2% among reported patients who are more than 50
years old. Following is a depiction of a typical course, including times of peak
fecal excretion of HAV, liver function test abnormalities, and clinical
symptoms.
How is hepatitis A virus transmitted, and who is at risk for this disease?
HAV is an RNA virus that only infects primates. HAV has a
fecal-oral route of transmission and is easily transmitted person to person. HAV
is also transmitted through contaminated food or water. Because HAV is present
in the blood during acute infection, bloodborne transmission is also possible,
but rare. The highest levels of HAV are found in the stool, and peak levels
occur in the 2 weeks before onset of illness.
Groups at increased risk for hepatitis A include travelers to developing
countries, men who have sex with men, and injecting and noninjecting drug users.
In the United States, 4% to 6% of reported cases occur among international
travelers, many of whom presumably acquired HAV infection from contaminated food
or water. Approximately 50% of persons with hepatitis A do not report any known
risk factors, and some of these infections may be from unrecognized transmission
via HAV-contaminated food.
How might this illness have been prevented?
Persons planning to travel to
an endemic region should receive hepatitis A vaccine or immune globulin before
departure. Hepatitis A vaccination can be given to anyone 2 years of age and
older, and has the advantage of providing long-term protection (at least 20
years). Hepatitis A vaccine is an inactivated HAV preparation; the first dose of
vaccine provides protective anti-HAV levels within 30 days for >90% of vaccine
recipients. Licensed hepatitis A vaccines available in the United States are
considered to be equivalent in effectiveness, and include Havrix®
(manufactured by Glaxo SmithKline), VAQTA® (Merck & Co.), and Twinrix®
(combined hepatitis A and hepatitis B vaccine, Glaxo SmithKline). Vaccination is
administered in a 2-dose schedule (0, 6 months) for Havrix® and VAQTA®,
and a 3-dose schedule (0, 1, 6 months) for Twinrix®. The second (or
third) dose is provided to ensure protection in those who did not respond to the
first dose of vaccine. Ninety-nine percent of vaccinees will be protected after
2 doses of vaccine.
For persons who present for hepatitis A immunoprophylaxis <30 days before
departure to an endemic region and for children <2 years old, immune globulin (IG)
is an effective means of preventing hepatitis A. IG is the appropriate
immunoprophylaxis for children <2 years old. IG is a sterile preparation of
concentrated antibodies (immunoglobulins) made from pooled human plasma. IG
provides protection against hepatitis A for 3--5 months, depending on dosage,
through passive transfer of antibody. Vaccine and IG may be given
simultaneously.
Hepatitis A is the most common vaccine-preventable disease among
travelers. The risk varies according to region visited and the length of
stay, and is increased even among travelers who report observing measures
to protect themselves against enteric infection or stay only in urban
areas. In the United States, children account for approximately one third
of reported travel-related cases.
What else needs to be done?
Cases of hepatitis A should be
reported to the local health department immediately. The patient's boyfriend and
any other household or sexual contacts whose last exposure to the patient was
<14 days ago should be given IG. Screening for immunity before administering IG
is not recommended in this situation because it is more costly than IG and would
delay its administration. IG is not indicated for family members or friends not
living in the household.
Prompt reporting of hepatitis A cases allows time to decide on a
course of action and provide timely immunoprophylaxis when appropriate.
Because this patient works as a food preparer, the health department will
need to visit the establishment to assess the likelihood that her duties
and hygiene practices pose a significant risk of food contamination. IG is
often recommended for co-workers of commercial food handlers with
hepatitis A. In addition, if she worked at any time during the 2 weeks
before onset of jaundice to 1 week after onset, persons who ate food
prepared or handled by this patient may be candidates for IG prophylaxis.
Determinations of the need for IG prophylaxis are made on a case-by-case
basis by experienced health department personnel. Again, immediate
reporting of hepatitis A cases allows time to decide on a course of action
and provide timely treatment and intervention when appropriate.
Norovirus Infection: A Patient Scenario
Nancy is a 25-year-old previously well graduate student who presents
to the emergency department with a 12-hour history of nausea, diarrhea,
abdominal cramping, and vomiting (about 6 episodes), malaise, and a
low-grade fever. She describes her onset of symptoms as sudden.
Physical examination shows that Nancy is afebrile with a supine blood
pressure of 123/74 mm Hg. She has a diffusely tender abdomen and is
dehydrated. Stool examination is negative for occult blood.
What is the possible differential diagnosis for her chief complaint?
Infectious gastroenteritis
Food intoxication (noninfectious gastroenteritis)
Inflammatory bowel disease
Appendicitis
Pelvic inflammatory disease
What additional information would assist with the diagnosis?
Did anyone in her household experience similar illness within
the week prior to onset of symptoms?
Has she been in contact with anyone outside her household
with similar symptoms within the previous week?
Has she had such symptoms before?
Does she know if anyone else became ill?
Has she traveled outside the United States within the last
month?
Has she previously had a sexually transmitted diseases or
does she have multiple sex partners?
Nancy reports that she rarely has diarrhea or vomiting. She also
reports no contact with anyone who was ill in the past week, nor has she
been out of the country in the past month. Her boyfriend, who does not
live with her, has similar symptoms with an almost identical onset time.
Both attended a wedding 2 days ago. The meal at the wedding reception,
which was held at a local reception hall, was the only meal they shared in
the past several days. Nancy does not know if anyone else who attended the
wedding became ill. Nancy reports that she has no history of a sexually
transmitted disease and that she and her boyfriend have a monogamous
sexual relationship.
How does this information assist with the diagnosis?
Based on
the rapid onset of symptoms, Nancy's reported past history of good health, and
the fact that her boyfriend has an almost identical history, inflammatory bowel
disease, appendicitis, and pelvic inflammatory disease are the least likely
diagnoses.
Food intoxication is also not very likely. Assuming that the wedding
reception was the source of the toxin, and this was their most recent common
meal, the time from exposure to onset of symptoms is too long. Toxins usually
cause illness within minutes to hours after ingestion.
The most likely diagnosis is infectious gastroenteritis. There is a
possibility that Nancy's and her boyfriend's illness may be associated with an
outbreak of gastroenteritis.
What additional information would assist with the identification of the
etiologic agent?
What sorts of foods were served at the wedding reception?
When did the couple last share a meal prior to the wedding
reception?
Has an outbreak of gastroenteritis associated with this
reception has been reported to the local health department?. The
health department may be able to aid in determining what the
etiologic agent was if it is currently investigating the outbreak.
At the wedding, the couple had a choice of meal. Nancy had lobster tail and
filet mignon. Her boyfriend had chicken. They both consumed stuffed mushrooms,
salad, and hors d'oeuvres preceding the main meal. For dessert they both had
wedding cake and fresh fruit. Both drank wine or beer during the reception.
The couple attended a barbecue the previous week. This outing was a
function sponsored by Nancy's employer. Nancy tells you that none of her
co-workers have been ill with vomiting and diarrhea.
You place an inquiry with the local health department about the possible
outbreak. The health department notifies you that an investigation is
currently under way. Illness has also been reported among 75% of attendees
at a wedding the day before the one Nancy attended, at the same reception
hall. The only common food between the 2 weddings is the salad, and the
health department currently suspects a food handler who worked during both
weddings who was experiencing diarrhea. Most patients have reported
nausea, vomiting (about 90%), and diarrhea (70%), with some fever,
malaise, headache, chills, and abdominal pain. The mean incubation period
for those who have reported illness is 28.6 hours, with a mean duration of
31.8 hours.
The health department suspects viral gastroenteritis caused by a
norovirus. A norovirus is suspected because of the rapid onset of
symptoms, the short 36-hour incubation period and relatively short
duration of illness, the absence of bloody diarrhea, and the high
percentage of vomiting. Bacterial cultures are negative for enteric
pathogens on stool samples collected thus far.
What are the complications of norovirus infection?
Noroviruses are common causes of self-limiting acute gastroenteritis, with
illness frequently lasting no longer than 60 hours. They commonly cause
outbreaks in such settings as restaurants, catered events, cruise ships,
schools, and nursing homes. The viruses can be spread person to person through
the fecal-oral route, through contaminated food or water, or by raw or
undercooked shellfish.
How should norovirus infections be managed?
There is no
antiviral agent that can be used to treat norovirus infections. Supportive care
such as oral or intravenous fluids for rehydration should be provided.
To reduce the spread of illness, patients should be educated to use good
hand washing practices, particularly after using the bathroom and before
preparing and handling food.
The health department requests that a stool sample be collected. The
sample should be collected in a sterile container without transport media,
and kept at 4°C (40°F) until shipped. The sample should be shipped on ice
packs to the local health department laboratory for testing. The health
department also asks you to encourage Nancy's boyfriend to submit a stool
sample.
How could this norovirus infection have been prevented?
The
food handler with diarrhea should not have returned to work for at least 24--48
hours after symptoms subsided.
Proper hand washing procedures can prevent the spread of the virus
between persons. Hands should be washed under warm water with soap for
approximately 15 seconds to prevent fecal-oral transmission.
Antibiotic-Resistant Salmonellosis: A Patient Scenario
Andrea brings her 3-year-old son, Marcus, to your office with a 2-day
history of low-grade fever, nausea, and 6--8 watery stools per day. Marcus
has also been complaining of abdominal pain and feeling tired. He has been
eating and drinking less than usual. His medical history is remarkable for
recurrent otitis media, for which he was prescribed oral antibiotics 10
days prior to this visit.
Physical examination reveals a well-developed boy who appears fatigued.
Vital signs are remarkable for low-grade fever (99.5°F/37.5°C). He does
not have signs of dehydration. His otitis appears resolved and he has a
normal cardiopulmonary exam. The abdominal exam reveals hyperactive bowel
sounds, mild diffuse tenderness, and stool negative for occult blood.
What is the differential diagnosis for Marcus' chief complaint?
Infectious gastroenteritis
Appendicitis
Celiac disease
Inflammatory bowel disease
Antibiotic-associated colitis
What additional information would assist with the diagnosis?
Has he had similar symptoms before?
Does he attend child care? If yes, have other children
attending the same care facility been ill with similar
symptoms?
Has the child recently consumed a meal outside his home;
eg, at a birthday party or restaurant?
Do other members of the household or close acquaintances
have diarrhea or bloody diarrhea?
Has he traveled in the month prior to the onset of
illness? If yes, where?
Has he had contact with pet reptiles or farm animals or
visited petting zoos in the week prior to his symptom onset?
Marcus has not had similar episodes of diarrhea in
the past. He attends preschool and is cared for by his grandmother after
school in her home. He last visited a petting farm 3 months prior to this
illness. Their family returned the previous day from a 5-day Caribbean
cruise. Marcus was diagnosed with otitis media 4 days prior to their
departure and was prescribed a 1-week course of oral antibiotics. Andrea
has had nausea and 3--4 loose stools per day for the previous 2 days. She
has not had any fever, abdominal pain, or vomiting. Marcus' father and two
sisters also traveled on the cruise and are asymptomatic. None of the
family members took prophylactic antibiotics for travelers' diarrhea
during the cruise.
How does this information assist with the diagnosis?
The additional history suggests that Marcus' and Andrea's illness may
be an infectious gastroenteritis related to their recent travel.
Antibiotic-associated colitis caused by
Clostridium difficile infection must be considered since the child was
prescribed antibiotics for otitis 8 days prior to this illness. Given the
recent onset, travel history, and his mother's symptoms, it is unlikely
that appendicitis, celiac disease, or inflammatory bowel disease are the
etiologies of Marcus' illness.
The most likely diagnosis is infectious gastroenteritis.
What additional historical information will assist in the
identification of the etiologic organism?
What foods did Marcus and Andrea consume in the previous week?
In particular, which foods/ beverages did they consume that the other family
members did not?
Did either Marcus or Andrea consume undercooked meats, runny
eggs, unpasteurized milk, raw shellfish, or untreated water?
Is there a reptile in the home?
Marcus was prescribed antibiotics for otitis media 1 week prior
to the onset of his gastrointestinal symptoms. Has Andrea been
prescribed antibiotics during the month prior to the onset of her
diarrheal illness?
Have there been other cases of diarrhea recognized in the cruise
ship travelers, in their community, or at Marcus' school?
An open-ended food history reveals multiple common meals
eaten by Andrea and Marcus. Andrea denies the consumption of
unpasteurized milk, raw shellfish, and undercooked meats. She does
report that, unlike the rest of the family, she and Marcus used to
wake up early enough to enjoy the breakfasts served on board the
cruise. Breakfast served on the cruise consisted of a choice of French
toast or pancakes with fruit compote, scrambled eggs or omelets made
to order, potatoes, and fresh fruit along with a choice of beverages,
including milk, coffee, and tea. Andrea complained that the eggs were
occasionally runny. Several fellow passengers told Andrea at breakfast
that they were experiencing vomiting and diarrhea. Andrea and Marcus
ate the remainder of their meals with the entire family. They did not
drink any untreated water or eat items purchased from street vendors
at ports of call. In response to your other questions, Marcus does not
have a reptile at home. Andrea has not been prescribed antibiotics for
more than 1 year. The family lives in a city and has access to
municipal water.
Based on the additional historical details, it
appears that many people on board the cruise were experiencing
symptoms of vomiting and diarrhea. This suggests an outbreak of
infectious gastroenteritis that may be related to a common food or
water source on the ship. The etiologic agent may be bacterial, viral,
or parasitic. The most likely bacterial organisms causing this
diarrheal illness are Campylobacter jejuni,Escherichia
coli,Shigella species, and Salmonella.
C. jejuni is the most common bacterial cause of diarrheal illness in the
United States. Outbreaks of
C. jejuni have been linked to raw milk, poultry, eggs, and water.
Enterotoxigenic E. coli (ETEC) is recognized as the most common
cause of "travelers' diarrhea" and can be transmitted via food or
water. Salmonella is an important bacterial cause of foodborne
illness, ranking just behind
C. jejuni in its frequency. Vehicles most commonly implicated in
foodborne outbreaks of salmonellosis include beef, poultry, produce,
eggs, pork, and dairy products. Large waterborne outbreaks of
salmonellosis have occurred rarely.
Why is identification of the cause of the diarrhea important?
Identification of the cause of diarrhea in these two cases is
important because of the impact on treatment, identification of
related cases, and detection of an outbreak and identification of
the responsible vehicle. Stool cultures should be performed to
detect common bacterial pathogens such as
Campylobacter, Salmonella,
Shigella, or E. coli O157:H7. Antimicrobial susceptibility results
can guide antibiotic therapy if a resistant organism is detected.
Additional testing may be conducted to detect nonbacterial
organisms. Stool examination for ova and parasites (O&P) will
reveal parasitic causes of foodborne and waterborne illness such
as
Cyclospora cayetanensis. Rotavirus infection, one of the most common
etiologies of pediatric diarrhea, may be diagnosed with enzyme
immunoassay (EIA). The presence of fecal leukocytes suggests
bacterial infection but may be found in other infectious or
inflammatory states. Testing for the presence of Shiga toxin to
detect infection with enterohemorrhagic
E. coli (EHEC) would be appropriate if Marcus or Andrea had bloody
diarrhea.
What approaches would you take to treating Marcus' and Andrea's illness? Are
antibiotics indicated for both Marcus and Andrea? What other therapeutic measures are useful for
the management of diarrheal illness?
Because Andrea's symptoms are mild, she does not wish to receive antibiotics. For Marcus, you prescribe trimethoprim-sulfamethoxazole at appropriate doses. You encourage Andrea to monitor for worsening fever, diarrhea, vomiting, and dehydration. You obtain stool specimens for culture and O&P from both Marcus and Andrea to confirm the
etiologic agent.
The primary goal of therapy for Marcus and Andrea is the maintenance of adequate hydration and electrolyte
balance. A commercial oral rehydration solution (ORS) may be used, particularly for Marcus, to provide glucose and salts.
You encourage Andrea to give Marcus ORS to prevent dehydration. Bismuth subsalicylate or loperamide may be used
to decrease the number of unformed stools and shorten the duration of diarrhea, although neither is available over
the counter for children of Marcus' age. Loperamide should not be used in those patients who develop fever or dysentery.
Finally, empiric antibiotic therapy can be used to treat "travelers' diarrhea," which is most commonly caused by ETEC, after obtaining the stool samples but prior to
obtaining results of stool cultures.
Three days after the initial visit, Andrea feels better with fewer stools per day, but Marcus has had worsening vomiting and diarrhea. He has had several episodes of high fever and has not been drinking ORS adequately. In the office, Marcus is
febrile (102°F/38.8°C) and appears dehydrated with dry mucous membranes and decreased skin turgor. No significant change is noted in the abdominal examination. You admit Marcus for intravenous hydration and encouragement of oral
rehydration and consider a change in antibiotic therapy. Because of the progressive systemic nature of his illness, you also obtain blood cultures at this time.
What information will guide your therapy at this time?
The use of intravenous fluids to improve volume status is reasonable given Marcus' inability to maintain hydration
with ORS. However, during hospitalization, he should be encouraged to resume drinking ORS as early as possible.
The decision to change from oral to intravenous antibiotics may be based on Marcus' increased vomiting and on his clinical decline. The choice of antibiotics should reflect the results of stool culture and antimicrobial sensitivities.
The laboratory reports the growth of
Salmonella Typhimurium from Marcus' stool cultures. Susceptibility testing reveals
an organism resistant to multiple antibiotics, including
ampicillin and sulfamethoxazole. Multidrug-resistant
S. Typhimurium has been on the rise in the United States since the early 1990s and now accounts for at least 25% of these isolates. Definitive
type 104 (DT 104), the most common phage type of multidrug-resistant
S. Typhimurium, may be responsible for more
invasive disease than other phage types. In an outbreak, resistant organisms appear to cause more cases than do sensitive
strains. Marcus' recent exposure to antibiotics for otitis media likely increased his susceptibility to
Salmonella infection, perhaps by decreasing the usual protection offered by normal bowel flora, and thus decreasing the infectious dose necessary to cause illness. In addition, he was placed at increased risk for infection with a resistant strain of
S. Typhimurium if he was exposed while still taking the antibiotic.
Treatment of Salmonella gastroenteritis with antibiotic therapy is controversial because of the resulting increase
in asymptomatic carriage, particularly among children less than 5 years of age. However, given the systemic nature of his
illness, you choose to treat Marcus with several days of an intravenous third-generation cephalosporin. This is a reasonable choice in light of the antimicrobial resistance and the reluctance to use fluoroquinolones in the pediatric population.
Should these cases be reported to the local health department? What are the public
health implications of these two cases of salmonellosis?
Salmonellosis is a nationally notifiable disease, and most states require clinicians to report cases to local or state
public health agencies. The health department and its public health partners can conduct studies to determine whether these cases indicated an outbreak of salmonellosis aboard the cruise ship. If an outbreak is confirmed, additional
investigation is necessary to identify the contaminated food or the ill food worker infected with
Salmonella, and whether there were
correctable food-handling errors. If a food vehicle
is identified, traceback and recall may be necessary to remove it from
the market and prevent the occurrence of other cases. Given the increasing prevalence of drug-resistant strains of
S. Typhimurium, public health laboratories may perform bacteriophage typing or pulsed-field gel electrophoresis (PFGE) to further characterize the drug-resistance patterns of these organisms. Reporting of these cases will contribute to essential nationwide surveillance of salmonellosis, foodborne outbreaks, and antimicrobial
resistance.
What prevention measures will you recommend to Marcus and Andrea? Are repeat
stool cultures necessary?
To prevent Salmonella infections, all meat and egg dishes should be fully cooked. Andrea can purchase eggs that
are pasteurized in the shell, and irradiated ground beef and poultry to reduce the risk of contamination. Basic food
safety practices in the kitchen can also help prevent such infections, such as refrigerating leftovers promptly, washing hands and utensils after contact with raw meat and poultry, and keeping raw meat and poultry separate from ready-to-eat
foods. Marcus and Andrea should be reminded to wash their hands with warm running water and soap after using the
bathroom and before and after meals to avoid transmitting the infection to others. Marcus is likely to have prolonged carriage of Salmonella in the intestines. While he may return to preschool as soon as he is feeling well enough to do so because direct spread from one child to another is rare, clinicians should defer to their local health departments regarding their clearance policies for convalescing children attending preschool.
With adequate hydration and your chosen antimicrobial therapy, Marcus will likely recover fully from this diarrheal
illness without residual complications.
Unexplained Illness: A Patient Scenario
You have been a primary care practitioner in Manhattan, New York, for several years. Jack, a 29-year-old otherwise
healthy male, has been your patient for the past year. At 8:00 a.m. he calls your triage nurse complaining of a very sudden onset of nausea, cramps, coughing, and sweating. The nurse is concerned about the suddenness of onset and wants to know what
you would like to do.
Should you have him call again later if he does not improve? Should you have him make
an acute-visit appointment, or should you send him to the emergency room?
You are concerned about the suddenness of the onset of symptoms but not the severity, so you decide to have him
come to the office immediately.
Jack presents in your office 30 minutes later. In addition to nausea, cramps, coughing, and sweating, his eyes have begun to tear uncontrollably and he complains of having had difficulty breathing while en route to the office. Upon arrival,
he immediately asks to use the bathroom.
Jack reports that he started his morning routine as usual with a run. Upon returning home, he finished drinking the bottle of water he had purchased earlier from the local deli and began to get ready for work. By the time he had finished
showering and dressing, he began to feel sick to his stomach. He then developed cramping but no diarrhea. Shortly thereafter, he began to have bouts of coughing uncontrollably. He does not know when the sweating started. He states that he had
difficulty breathing while en route to the office, and that the tearing just started. He denies vomiting, hemoptysis, hematuria, bright red blood per rectum (BRBPR), chills,
fever, headache, myalgia, arthralgia, or diarrhea. Jack also denies the use of any
medication, other drugs or alcohol. "That stuff rots your gut."
Jack reports that he finished his run at about 7:00 a.m. It is now 9:00 a.m..
Despite having just urinated, he states that he must go again and immediately. However, Jack experiences incontinence
on his way to the bathroom. Upon his return to the exam room, you notice a slight tremor in his left arm. He states that this has only just begun.
What preliminary diagnosis can you make at this point?
An anxiety attack
A viral syndrome
A potential foodborne illness
Anticholinergic poisoning
You are not ready to reach a conclusion at this point, so you move to a physical exam and observe the following:
You note that Jack is anxious but oriented to time, place, and person. His head, ears, eyes, nose, throat (HEENT)
examination shows bilateral miosis and decreased reactivity. There are no signs of trauma or bleeding. His heart has regular rate and rhythm, no murmur, and good perfusion. Radial and dorsal pulses are 2+. His lung examination reveals scattered
wheezing. His abdomen is soft, nontender, not distended, with
increased bowel sounds, and no mass. Extremities appear within
normal limits. The neurologic exam reveals the slight tremor in his left arm, slightly slurred speech, excessive salivation, and transient fasciculations in both upper extremities. You note negative Babinski and his cranial nerves (CN) 2-11 appear intact, while CN 12 appears slightly abnormal.
What other information would assist with the diagnosis?
More history from Jack, including most recent activity and diet.
You now seek additional history. Jack lives alone and does not believe that he has been in contact with anyone who is ill.
He works in an office as a lawyer. His run takes him up 5th Avenue and then over to 3rd Avenue, then back home. He does
not run through Central Park. He does not have plants and does not garden as a hobby. His most recent meal was the
night before, about 10 hours prior to the onset of his symptoms. It consisted of boiled pasta, steamed broccoli, and olive oil. He prepared the meal himself. He states that he carefully washed the broccoli, the oil was from a bottle he opened last week, and the pasta was from a box he had already used 2 days before. All he had to drink was tap water with dinner last evening and the bottled water from this morning.
Jack's presentation appears to involve which of the following systems?
Autonomic nervous system
Lymphatic system
Central nervous system
The signs and symptoms in Jack's presentation predominantly involve increased autonomic responses, and are
perhaps progressing to include the central nervous system as well. You decide that immediate treatment is called for and order oxygen, atropine, and pralidoxime (2-PAM). Given that Jack does not appear to have been exposed dermally, the most likely
route appears to have been oral. Therefore, you also appropriately begin an IV with normal saline
What is the initial diagnosis?
This presentation is not consistent with bacterial, viral, or parasitic food poisoning. While the signs and
symptoms indicate acute organophosphate poisoning, the history provides no indication, and indeed seemingly contradicts this theory because of the lack of exposure. There has been no exposure to places where organophosphates are typically used, such as on lawns, house plants, and parks. Nevertheless, Jack has presented with a fairly classic case of organophosphate
poisoning. Therefore, ingestion must be considered. Since you have no suggestion of deliberate ingestion on Jack's part, it must be assumed that he has consumed it unintentionally.
Organophosphate poisoning has an onset of 30 minutes to 2 hours. Jack has actually made it easy to identify the most
likely source: the only thing he has consumed in 10 hours is water. The broccoli could have had pesticides on it that may not have been removed when Jack washed it, but then he would have developed his symptoms during the night. Taking into
account the temporal relationship between his ingestion of the bottled water and the onset of his symptoms, the bottled water seems the most likely candidate.
Given this information, what are key questions you should consider?
Is the water truly contaminated?
If it is, how did it become contaminated?
Who else may have ingested it?
Who else is at risk?
What action should be taken?
You realize that if your diagnosis and conclusions are correct then a public health hazard may exist. Two things need
to be done. First, the health department must be contacted, and second, tests need to be done that will confirm
your diagnosis. While the usual work-up for organophosphate
poisoning is clinical diagnosis, there are assays available
to measure cholinesterase activity in plasma and red blood cells. It is also possible to detect some pesticides in urine. You decide to order both tests as this will provide the greatest insight into what the possible exposure is for other people in Jack's building, neighborhood, or even his city.
When communicating with the local public health department, whom should you ask
to speak to concerning this situation?
The medical epidemiologist?
The medical director?
The infectious disease officer?
You ask to speak with the medical director. You present Jack's case, making careful note of the time course, and
also inform the medical director of your suspicions of the source. The medical director takes this information and agrees with your concerns. She then asks you to speak with the chief epidemiologist so that an investigation can begin.
In many large cities, there is a city health department; in smaller cities or towns, it will usually be necessary to contact the local or state health department. Try to match the level with the greatest number of people who may become affected. Other persons who may be of immediate help if you cannot reach the medical officer are the epidemiologist or even an environmental health officer. These people will most likely know what to do with the information you have.
Most health departments across the country have been working to increase their knowledge or at least their awareness
of the possibility of intentional contamination. Many have also created positions solely devoted to this task. Therefore, it is possible that you will be directed to such an individual.
The health department initiates an investigation that
includes testing the water; looking for other cases of organophosphate poisoning; interviewing the patient;
notifying other parts of the public health system, including law enforcement, CDC,
and the state health department. They may even issue a public notice.
There is another possible cause for the case you have just seen: sarin gas can cause a similar presentation. If sarin gas had been sprayed into the air, it is possible that Jack could have respiratory exposure to the nerve gas.
If this were true, how would it change what you did?
Persons exposed to sarin, and possibly other nerve agents, will have a clinical presenation similar to those
with organophosphate poisoning. Hence, medical management will likely be similar.
Finally, you are gratified to have helped detect a possible act of contamination that could potentially harm or even kill a great many people. Afterward, while making rounds in the hospital that day you are told by a colleague that a number
of runners from a 5K race in Central Park this morning and tourists visiting the Empire State Building were brought to
the emergency room complaining of sudden onset of nausea, cramps, and coughing. It was reported that all had been
drinking bottled water.
Clinical Vignettes: What's Your Call?
The following clinical vignettes are provided for your self-evaluation. All are possible situations that may present at
your practice. The "Diagnostic Considerations" section and the tables of etiologic agents that are also part of this primer will provide the information necessary for you to adequately
address these clinical situations. Note that these
vignettes include both infectious and noninfectious forms of foodborne illness.
For the following clinical vignettes, choose the best answer from the choices listed at the end of the vignettes:
A --- likely diagnosis; choose the best possible answer listed on "answer selections" page under
A selections.
B --- most appropriate choice to confirm the diagnosis (there may be more than one correct answer --- list all of them). Choose from the possible answers listed on "answer selections" page under the
B section.
Finally, decide whether the situation warrants reporting to the local or state health department.
Clinical Vignettes
You receive a long-distance call from a patient who is an outdoorsman. He is with a group that collected and ate
some wild mushrooms less than 2 hours ago. Several members of the group have since developed vomiting, diarrhea,
and some mental confusion.
A --- likely diagnosis: _____________________________________
B --- most appropriate test to confirm etiology/follow-up action:
_________________________________
Report to the health department? ___Yes ___No
A newborn child has symptoms of sepsis. Cerebrospinal fluid
studies are consistent with meningitis. The mother had a flu-like
syndrome prior to delivery.
A --- likely diagnosis: _____________________________________
B --- most appropriate test to confirm etiology/follow-up action:
_____________________________________
Report to the health department? ___Yes ___No
This patient has just returned today from Latin America following a 2-day business trip. He reports having
eaten several meals of fish that he bought from street vendors around his hotel. He feels very ill with profuse,
watery diarrhea, and vomiting.
A --- likely diagnosis: _____________________________________
B --- most appropriate test to confirm etiology/follow-up action:
_____________________________________
Report to the health department? ___Yes ___No
An 18-month-old child is brought to your office with fever, bloody diarrhea, and some vomiting. She has
been drinking unpasteurized milk in the last 48 hours. No other family members are ill.
A --- likely diagnosis: _____________________________________
B --- most appropriate test to confirm etiology/follow-up action:
_____________________________________
Report to the health department? ___Yes ___No
A patient calls and states that he and several family members are ill with severe vomiting. They ate at a church picnic
4 hours earlier.
A --- likely diagnosis: _____________________________________
B --- most appropriate test to confirm etiology/follow-up action:
_____________________________________
Report to the health department? ___Yes ___No
A patient calls and states that most family members have developed severe vomiting, about 1 hour after eating at
a picnic. They ate barbecued beef, chips, potato salad, and homemade root beer. Some are complaining of a
metallic taste.
A --- likely diagnosis: _____________________________________
B --- most appropriate test to confirm etiology/follow-up action:
_____________________________________
Report to the health department? ___Yes ___No
VII. A patient has had chronic intermittent diarrhea for about 3 weeks. There is no fever or vomiting and no blood in
the stool. The patient travels to Latin America and Eastern Europe frequently, most recently 2 weeks ago.
A --- likely diagnosis: _____________________________________
B --- most appropriate test to confirm etiology/follow-up action:
_____________________________________
Report to the health department? ___Yes ___No
The parents of a 6-month-old infant are concerned because she is listless and weak. The infant is feeding poorly,
has poor head control, and is constipated. There is no fever or vomiting.
A --- likely diagnosis: _____________________________________
B --- most appropriate test to confirm etiology/follow-up action:
_____________________________________
Report to the health department? ___Yes ___No
A businessman who travels frequently is ill with
fatigue, jaundice, abdominal pain, and diarrhea. About 1 month
ago, he returned from an international trip during which he consumed raw oysters.
A --- likely diagnosis: _____________________________________
B --- most appropriate test to confirm etiology/follow-up action:
_____________________________________
Report to the health department? ___Yes ___No
Several members of a single family are ill with abdominal cramps and watery diarrhea. They just returned from
visiting friends on the East Coast of the United States, where they consumed raw oysters 48 hours ago.
A --- likely diagnosis: _____________________________________
B --- most appropriate test to confirm etiology/follow-up action:
_____________________________________
Report to the health department? ___Yes ___No
A minister at a local church calls to report that many members began experiencing watery diarrhea on the
morning after the annual turkey dinner fundraiser. Some people also reported nausea and abdominal cramps, but no one
has fever or bloody stools.
A --- likely diagnosis: _____________________________________
B --- most appropriate test to confirm etiology/follow-up action:
_____________________________________
Report to the health department? ___Yes ___No
You receive a long-distance call from a patient on a fishing vacation off the coast of Belize. Her family has been
eating a variety of local fish and shellfish that they caught. She reports that several family members developed
abdominal pain, severe diarrhea, and weakness the morning after they consumed the seafood for dinner. One family member began having difficulty speaking later on that same night.
A --- likely diagnosis: _____________________________________
B --- most appropriate test to confirm etiology/follow-up action:
_____________________________________
Report to the health department? ___Yes ___No
A family in a rural community is worried that their father may be having a stroke. He is complaining of double
vision and is having trouble swallowing. They have a large garden and eat home-canned vegetables.
A --- likely diagnosis:
B --- most appropriate test to confirm etiology/follow-up action:
Report to the health department? ___Yes ___No
A 2-year-old child who attends day care presents with abdominal cramps and severe bloody diarrhea, which has
been present for 2 days. He has no fever.
A --- likely diagnosis: _____________________________________
B --- most appropriate test to confirm etiology/follow-up action:
_____________________________________
Report to the health department? ___Yes ___No
Susan tells you that she has had diarrhea, nausea, and abdominal cramping for almost 12 hours now. She also
presents with malaise and a low-grade fever and informs you that as far as she can tell, the symptoms developed very
suddenly. Stool examination is negative for occult blood. Susan informs you that her good friend is also sick and they
both attended a company picnic less than 2 days ago.
A --- likely diagnosis: _____________________________________
B --- most appropriate test to confirm etiology/follow-up
action: _____________________________________
Report to the health department? ___Yes ___No
Sally arrives at your office with acute gastrointestinal illness characterized by diarrhea, abdominal cramps, chills,
fever, and body aches. She also informs you that about 3 days before she started getting sick, she had consumed raw
ground beef that was seasoned with onions and an herb mix.
A --- likely diagnosis: _____________________________________
B --- most appropriate test to confirm etiology/follow-up action:
_____________________________________
Report to the health department? ___Yes ___No
James presents to the emergency room with a low-grade fever and complaining of fatigue and nausea for the past
24 hours. He also describes his urine as being dark and states that he has had 4 bowel movements in the past 24 hours,
all of which were light colored. Upon further questioning, James says that he has no history of jaundice and that
he returned from a business trip to the Philippines a month ago.
A --- likely diagnosis: _____________________________________
B --- most appropriate test to confirm etiology/follow-up action:
_____________________________________
Report to the health department? ___Yes ___No
You are halfway through your shift in the ER. There are four patients, two adults and two children, with a history of nausea, vomiting, abdominal pain, and profuse (especially in the children) watery diarrhea in the absence of
fever. They each report that these symptoms began 5 days ago and resolved after 1 day. They had all been symptom free
for 3 days, but now the symptoms have returned. There is also a new onset of jaundice and bloody diarrhea. Lab
results indicate elevated LFTs. The patients do not know each other, but all report eating hamburgers several hours before the initial onset of symptoms.
A --- likely diagnosis: _____________________________________
B --- most appropriate test to confirm etiology/follow-up action:
_____________________________________
Report to the health department? ___Yes ___No
A mother has brought in a 5-month-old child with apparent blindness. She reports that the child had been healthy until the past month when the vision problems appeared. The mother states that she had been well during the pregnancy,
but further questioning reveals that the mother had two young cats at home for which she was the sole care provider. The cats were given away just before the birth of the child because of concerns about the child being smothered by the cats.
A --- likely diagnosis: _____________________________________
B --- most appropriate test to confirm etiology/follow-up action:
_____________________________________
Report to the health department? ___Yes ___No
Answer Choices
A: Choose from any of these possible etiologies:
Intoxication from preformed toxins of
Staphylococcus aureus or Bacillus cereus
Intoxication from toxins produced in vivo
by Clostridium perfringens
Salmonella or Campylobacter
are possible.
E. coli O157:H7
Noroviruses, Vibrio
parahaemolyticus, and other Vibrio infections
Vibrio cholerae infection
Botulism must be ruled out
Listeria monocytogenes sepsis
Cryptosporidium parvum
Cyclospora cayetanensis
A form of metal poisoning
A form of mushroom poisoning
Likely fish/shellfish toxin
Giardia lamblia
Trichinella spiralis
Hepatitis A virus
Congenital toxoplasmosis
Intentional amanitin poisoning
B: Choose from any of these following tests/actions
Clinical diagnosis; laboratory tests may not always be indicated.
Generally detected on routine stool cultures.
Generally, a reference laboratory is needed to identify the toxin from food, stool, or vomitus.
Important to identify causative organism for public health reasons.
Send stool samples to health department
(Vibrio cholerae, other vibrios, E. coli O157:H7, special toxin tests, Clostridium perfringens, Clostridium botulinum).
Not detected by routine stool cultures
(E. coli O157:H7, Vibrio cholerae, other vibrios).
Should test for viral agents.
For cysts, ova, and parasite detection, at least 3 stool samples must be collected. Sometimes the organism may still
be missed.
Test for appropriate metal.
Special test needed to identify a fish toxin.
Consult a mycologist to identify the mushroom.
Blood culture is the best source for diagnosis.
Blood test helpful to identify the agent.
May need acute and convalescent serum or viral cultures.
Isolation of T. gondii from infant blood. PCR of white blood cells or CSF, or IgM and IgA serology, performed by a reference laboratory.
Rapid and aggressive antitoxin therapy. There is no single effective antidote at this time, but silibinin (with penicillin G) and N acetyl cysteine are showing promise. Plan for hepatic and renal failure.
Guerrant RL, Van Gilder T, Steiner TS, et al. Practice guidelines for the management of infectious diarrhea. Clin Infect Dis. 2001:32:331--351.
Mead PS, Slutsker L, Dietz V, et al. Food-related illness and death in the United States. Emerg Infect Dis [serial online]; 1999;5 (5):607--625. Available from: URL:
http://www.cdc.gov/ncidod/eid/vol5no5/mead.htm.
Swerdlow DL, Altekruse SF. Foodborne diseases in the global village: what's on the plate for the 21st century. In: Scheld WM, Craig WA, Hughes JM, eds. Emerging Infections 2. Washington, DC: ASM Press; 1998:273--293.
Tauxe RV, Swerdlow DL, Hughes JM. Foodborne disease. In: Mandell GL, Bennett JE, Dolin R, eds. Principles and Practice of Infectious Diseases, Fifth Edition. New York: Churchill Livingstone; 2000:1150--1165.
Tauxe RV. Emerging foodborne diseases: an evolving public health challenge. Emerg Infect Dis. [serial online] 1997;3:425--434. Available from URL
http://www.cdc.gov/ncidod/eid/vol3no4/tauxe.htm
Turnbull PCB. Guidelines for the surveillance and control of anthrax in humans and animals. Geneva: World Health Organization, 1998.
Publication #WHO/EMC/ZDf/98.6.
Inglesby TV, Henderson DA, Bartlett JG, et al. Anthrax as a biological weapon: medical and public health management. Working Group on
Civilian Biodefense. JAMA. 1999;281:1735--1745.
Botulism
Arnon SS, Schechter R, Inglesby TV, et al. Botulinum toxin as a biological weapon: medical and public health management. JAMA. 2001; 285:1059--1070.
Shapiro RL, Hatheway C, Becher J, Swerdlow DL. Botulism surveillance and emergency response: a public health strategy for a global challenge. JAMA. 1997;278:433--435.
Angulo FJ, Getz J, Taylor JP, et al. A large outbreak of botulism: the hazardous baked potato. J Infect Dis. 1998;178:172--177.
Angulo FJ, St. Louis ME. Botulism. In: Evans AS, Brachman PS, eds. Bacterial Infections of Humans. New York: Plenum; 1998:131--53.
Brainerd Diarrhea
Mintz ED, Weber JT, Tauxe RV, et al. An outbreak of Brainerd diarrhea among travelers to the Galapagos Islands. J Infect Dis. 1998; 177:1041--1045.
Osterholm MT, MacDonald KL, White KE, et al. An outbreak of newly recognized chronic diarrhea syndrome associated with raw milk
consumption. JAMA. 1986;256:484--490.
Brucellosis
Sauret JM, Vilissova N. Human brucellosis. J Am Board Fam Pract. 2002;15:401--406.
Baldi PC, Miguel SE, Fossati, CA, Wallach JC. Serological follow up of human brucellosis by measuring IgG antibodies to lipopolysaccharide
and cytoplasmic proteins of Brucella species. Clin Infect Dis. 1996;22:446--455.
Martin Mazuelos E, Nogales MC, Florez C, Gomez Mateos M, Lozano F, Sanchez A. Outbreak of
Brucella melitensis among microbiology
laboratory workers. J Clin Microbiol. 1994;32:2035--2036.
Khuri-bulos NA, Doud AH, Azab SM. Treatment of childhood brucellosis: results of a prospective trial on 113 children. Pediatr Infect Dis J. 1993;12:377--381.
Chomel BB, DeBess EE, Mangiamele DM, et al. Changing trends in the epidemiology of human brucellosis in California from 1973 to 1992: a shift toward foodborne transmission. J Infect Dis. 1994;170:1216--1223.
Campylobacter
Allos BM. Campylobacter jejuni infections: update on emerging issues and trends. 2001. Clin Infect Dis. 2001;32:1201--1206.
Roels TH, Wickus HH, Bostrum JJ, et al. A foodborne outbreak of
Campylobacter jejuni infection associated with tuna salad: a rare strain in an
unusual vehicle. Epidemol Infect. 1998;121:281--287.
Smith KE, Besser JM, Hedberg CW, et al. Quinolone-resistant
Campylobacter jejuni infections in Minnesota, 1992--1998. N Engl J
Med. 1999;340:1525--1532.
Allos BM, Taylor DN. Campylobacter infections. In: Evans AS, Brachman PS, eds. Bacterial Infections of Humans. New York: Plenum
Medical; 1998:169--190.
Cholera
Guerrant RL, Carneiro-Filho BA, Dillingham RA. Cholera, diarrhea, and oral rehydration therapy: triumph and indictment. Clin Infect
Dis. 2003;37:398--405.
Mahon BE, Mintz ED, Greene KD, et al. Reported cholera in the United States, 1992--1994: a reflection of global changes in cholera epidemiology. JAMA. 1996;276:307--312.
Wachsmuth IK, Blake PA, Olsvik O, eds. Vibrio
cholerae and cholera: molecular to global perspectives. Washington, DC: American Society
for Microbiology; 1994.
Shears P. Recent developments in cholera. Curr Opin Infect Dis. 2001;14:553--558.
Clostridium
Kalinowski RM, Tompkin RB, Bodnaruk PW, Pruett WP Jr. Impact of cooking, cooling, and subsequent refrigeration on the growth or survival of Clostridium perfringens in cooked meat and poultry products.
J Food Prot. 2003;66:1227--1232.
Hogenauer C, Hammer HF, Krejs GJ, Reisinger EC. Mechanisms and management of antibiotic-associated diarrhea. Clin Infect Dis. 1998;27:702--710.
Brynestad S, Granum PE. Clostridium
perfringens and foodborne infections. Int J Food Microbiol. 2002;74:195--202.
Simor AE, Bradley SF, Strausbaugh LJ, Crossley K, Nicolle LE; SHEA Long-Term-Care Committee.
Clostridium difficile in long-term-care facilities for
the elderly. Infect Control Hosp Epidemiol. 2002;23:696--703.
Moyenuddin M, Williamson JC, Ohl CA. Clostridium
difficile-associated diarrhea: current strategies for diagnosis and therapy. Curr Gastroenterol Rep. 2002;4:279--286.
Herwaldt BL. Cyclospora cayetanensis: A review focusing on the outbreaks of cyclosporiasis in the 1990s. Clin Infect Dis. 2000;31:1040--1057.
Herwaldt BL, Ackers ML. An outbreak in 1996 of cyclosporiasis associated with imported raspberries. N Engl J Med. 1997;336:1548--1556.
Herwaldt BL, Beach MJ. The return of Cyclospora in 1997: another outbreak of cyclosporiasis in North America associated with imported raspberries. Ann Intern Med. 1999;130:210--220.
Soave R, Herwaldt BL, Relman DA. Cyclospora. Infect Dis Clin North Am. 1998;12:1--12.
Diarrheogenic E. coli
Dalton CB, Mintz ED, Wells JG, et al. Outbreaks of enterotoxigenic
Escherichia coli infection in American adults: a clinical and epidemiologic profile. Epidemiol Infect 1999; 123:9--16.
Moyenuddin M, Wachsmuth IK, Moseley SL, et al. Serotype, antimicrobial resistance, and adherence properties of
Escherichia coli strains associated with outbreaks of diarrheal illness in children in the United States. J Clin Microbiol. 1989; 27:2234--2239.
MacDonald KL, Eidson M, Strohmeyer C, et al. A multistate outbreak of gastrointestinal illness caused by enterotoxigenic
Escherichia coli in imported semisoft cheese. J Infect Dis. 1985;151:716--720.
Scott E. Relationship between cross-contamination and the transmission of foodborne pathogens in the home. Pediatr Infect Dis J.
2000;19(10 Suppl):S111--113.
Kohl KS, Rietberg K, Wilson S, Farley TA. Relationship between home food-handling practices and sporadic salmonellosis in adults in
Louisiana, United States. Epidemiol Infect. 2002;129:267--276.
Altekruse SF, Street DA, Fein SB, Levy AS. Consumer knowledge of foodborne microbial hazards and food-handling practices. J Food
Prot. 1996;59:287--294.
Reid DS, Harris LJ. Microorganisms and microbial toxins. Adv Exp Med Biol. 1999;459:9--21.
Blaha T. Epidemiology and quality assurance application to food safety. Prev Vet Med. 1999;39(2):81--92.
Escherichia coli O157:H7
Park S, Worobo RW, Durst RA. Escherichia
coli O157:H7 as an emerging foodborne pathogen: a literature review. Crit Rev Biotechnol. 2001;21:27--48.
Peacock E, Jacob VW, Fallone SM. Escherichia
coli O157:H7: etiology, clinical features, complications, and treatment. Nephrol Nurs J.
2001;28:547--557.
Bender JB, Hedberg CW, Besser JM, et al. Surveillance for
Escherichia coli O157:H7 infections in Minnesota by molecular subtyping. N Engl J.
Med. 1997;337:388--394.
Mahon BE, Griffin PM, Mead PS, Tauxe RV. Hemolytic uremic syndrome surveillance to monitor trends in infection with
Escherichia coli O157:H7 and other Shiga toxin-producing
E. coli. Emerg Infect Dis [serial online]. 1997;3:409--412. Available at URL
http://www.cdc.gov/ncidod/eid/vol3no3/letters.htm#mahon
Slutsker L, Ries AA, Greene KD, et al. Escherichia
coli O157:H7 diarrhea in the United States: clinical and epidemiologic features. Ann Intern
Med. 1997; 126:505--513.
Gardner TB, Hill DR. Treatment of giardiasis. Clin Microbiol Rev. 2001;14:114--128.
Nash TE. Treatment of Giardia lamblia infections. Pediatr Infect Dis J. 2001;20:193--195.
Mintz ED, Hudson-Wragg M, Mshar P, et al. Foodborne giardiasis in a corporate office setting. J Infect Dis. 1993;167:250--253.
Osterholm MT, Forfang JC, Ristinen TL, et al. An outbreak of foodborne giardiasis. N Eng J Med. 1981;304:24--28.
Petersen LR, Cartter ML, Hadler JL. A foodborne outbreak of
Giardia lamblia. J Infect Dis. 1988;157:846--848.
Hepatitis A
CDC. Prevention of hepatitis A through active or passive immunization: recommendations of the Advisory Committee on Immunization
Practices (ACIP). MMWR. 1999:48( No. RR-12).
Cuthbert JA. Hepatitis A: old and new. Clin Microbiol Rev. 2001;14: 38--58.
CDC. Public health dispatch: multistate outbreak of hepatitis A among young adult concert attendees---United States, 2003. MMWR.
2003;52:844--845.
Listeriosis
Mylonakis E, Paliou M, Hohmann EL, Calderwood SB, Wing EJ. Listeriosis during pregnancy: a case series and review of 222 cases.
Medicine (Baltimore). 2002;81:260--269.
Taege AJ. Listeriosis: recognizing it, treating it, preventing it. Cleve Clin J Med. 1999;66:375--380.
Salamina G, Donne ED, Niccolini A, et al. A foodborne outbreak of gastroenteritis involving
Listeria monocytogenes. Epidemiol Infect.
1996;117:429--436.
Schuchat A. Listeriosis and pregnancy: food for thought. Obstet Gynecol Surv. 1997;52:721--722.
Slutsker L, Schuchat A. Listeriosis in humans. In: Ryser ET, Marth EH, eds. Listeria, Listeriosis, and Food Safety. New York: Marcel Dekker; 1999;75--95.
Noroviruses
Matson DO, Szucs G. Calicivirus infections in children. Curr Opin Infect Dis. 2003;16:241--246.
Fankhauser RL, Noel JS, Monroe SS, Ando TA, Glass RI. Molecular epidemiology of "Norwalk-like viruses" in outbreaks of gastroenteritis in the United States. J Infect Dis. 1998;178:1571--1578.
Hedberg CW, Osterholm MT. Outbreaks of foodborne and waterborne viral gastroenteritis. Clin Microbiol Rev. 1993;6:199--210.
Parashar UD, Dow L, Fankhauser RL, et al. An outbreak of viral gastroenteritis associated with consumption of sandwiches: implications for the
control of transmission by food handlers. Epidemiol Infect. 1998;121: 615--621.
CDC. "Norwalk-like viruses:" public health consequences and outbreak management. MMWR 2001;50(No. RR-9).
Salmonellosis
Parry CM. Antimicrobial drug resistance in Salmonella
enterica. Curr Opin Infect Dis. 2003;16:467--472.
Zaidi E, Bachur R, Harper M. Non-typhi
Salmonella bacteremia in children. Pediatr Infect Dis J. 1999;18:1073--1077.
Mahon BE, Ponka A, Hall WN, et al. An international outbreak of
Salmonella infections caused by alfalfa sprouts grown from contaminated seeds.
J Infect Dis. 1997;175:876--882.
Mermin J, Hoar B, Angulo FJ. Iguanas and
Salmonella Marina infection in children: a reflection of the incidence of reptile-associated salmonellosis
in the United States. Pediatrics. 1997;99:399--402.
Shane AL, Tucker NA, Crump JA, et al. Sharing Shigella: risk factors for a multicommunity outbreak of shigellosis. Arch Pediatr Adolesc
Med. 2003;157:601--603.
Khan WA, Dhar U, Salam MA, et al. Central nervous system manifestations of childhood shigellosis: prevalence, risk factors, and outcome. Pediatrics. 1999;103:E18.
Sobel J, Cameron DN, Ismail J, et al. A prolonged outbreak of
Shigella sonnei infections in traditionally observant Jewish communities in
North America caused by a molecularly distinct bacterial subtype. J Infect Dis. 1998;177:1405--1408.
Mohle-Boetani JC, Stapleton M, Finger R, et al. Community-wide shigellosis: control of an outbreak and risk factors in child day-care centers. Am J Public Health. 1995;85:812--816.
Ries AA, Wells JG, Olivola D, et al. Epidemic
Shigella dysenteriae type 1 in Burundi: panresistance and implications for prevention. J Infect
Dis. 1994;169:1035--1041.
Lee LA, Shapiro CN, Hargrett-Bean N, Tauxe RV. Hyperedemic shigellosis in the United States: a review of surveillance data for
1967--1988. J Infect Dis. 1991;164:894--900.
Toxoplasmosis
Jones J, Lopez A, Wilson M. Congenital toxoplasmosis. Am Fam Physician. 2003;67:2131--2138.
Masur H, Kaplan JE, Holmes KK, U.S. Public Health Service; Infectious Diseases Society of America. Guidelines for preventing
opportunistic infections among HIV-infected persons---2002. Recommendations of the U.S. Public Health Service and the Infectious Diseases Society of America. Ann Intern Med. 2002;137:435--478.
Schellenberg RS, Tan BJ, Irvine JD, et al. An outbreak of trichinellosis due to consumption of bear meat infected with
Trichinella nativa, in 2 northern Saskatchewan communities. J Infect Dis. 2003;188:835--843.
Bruschi F, Murrell KD. New aspects of human trichinellosis: the impact of new
Trichinella species. Postgrad Med J. 2002;78:15--22.
Capo V, Dickson DD. Clinical aspects of infections with Trichinella spp. Clin Microbiol. 1996;9:47--54.
Laurichesse H, Cambon M, Perre D, et al. Outbreak of trichinellosis in France associated with eating horse meat. Com Dis Rep. 1997;7(5):R69-73.
MacLean JD, Viallet J, Law C, Staudt M: Trichinosis in the Canadian Arctic: report of five outbreaks and a new clinical syndrome. J Infect Dis. 1989;160:513.
Typhoid Fever
Olsen SJ, Bleasdale SC, Magnano AR, et al. Outbreaks of typhoid fever in the United States, 1960--99. Epidemiol Infect. 2003;130:13--21.
Stephens I, Levine MM. Management of typhoid fever in children. Pediatr Infect Dis J. 2002;21:157--58.
Mermin JH, Townes JM, Gerber M, et al. Typhoid fever in the United States, 1985--1994: changing risks of international travel and
increasing antimicrobial resistance. Arch Intern Med. 1998;158:633--638.
Ackers ML, Puhr ND, Tauxe RV, et al. Laboratory-based surveillance of
Salmonella serotype Typhi infections in the United States: antimicrobial resistance on the rise. JAMA 2000; 283:2668--2673
References Used To Compile Etiology Tables
Askew GL, Finelli L, Genese CA, Sorhage FE, Sosin DM, Spitalny KC. Boilerbasse: an outbreak of methemoglobinemia in New Jersey in
1992. Pediatrics. 1994;94:381.
Bhat RV, Beedu SR, Ramakrishna Y, Munshi KL. Outbreak of trichothecene mycotoxicosis associated with consumption of mould-damaged
wheat products in Kashmir Valley, India. Lancet. 1989;1:35.
Cartwright CP. Utility of multiple-stool-specimen ova and parasite examinations in a high-prevalence setting.
J Clin Microbiol. 1999; 37:2408--2411.
DuPont HL. The Practice Parameters Committee of the American College of Gastroenterology. Guidelines on acute infectious diarrhea in adults. Am J Gastroenterol. 1997;92:1962.
Eliason BC, Lewan RB. Gastroenteritis in children: principles of diagnosis and treatment. Am Fam Physician. 1998;58:1769.
Fleming CA, Caron D, Gunn JE, Barry MA. A food borne outbreak of
Cyclospora cayetanensis at a wedding: clinical features and risk factors for
illness. Arch Intern Med. 1998;158:1121.
Morgan MRA, Fenwick GR. Foodborne illness: natural foodborne toxicants. Lancet. 1990;336:1492.
Neill MA, Osterholm MT, Swerdlow DL. New threats from food borne infections. Patient Care. July 15, 1994;47--71.
Rodrigue DC, Etzel RA, de Porras E, et al. Lethal paralytic shellfish poisoning in Guatemala. Am J Trop Med Hyg. 1990;42:267.
Schlech WF, III. Listeria gastroenteritis: old syndrome, new pathogen.
N Engl J Med. 1997; 336:130--132.
Seamens CM, Schwartz G. Food-borne illnesses: differential diagnosis and targeted management. Emerg Med Ref. 1998;19:120.
Tangermann RH, Etzel RA, Mortimer L, Renner GD, Paschal DC. An outbreak of a food-related illness resembling boric acid poisoning. Arch Environ Contam Toxicol. 1992;90:228.
Tauxe RV, Hughes JM. Foodborne disease. In: Mandel GF, Bennett JE, Dohr R, eds. Principles and Practices of Infectious Diseases 5th ed. Churchill Livingstone: New York; 2000;1150.
Wong CS, Jelacic S, Habeed RL, Watkins SL, Tarr PI. The risk of the hemolytic-uremic syndrome after antibiotic treatment of Escherichia coli O157:H7 infections. N Engl J Med. 2000; 342:1930--1936.
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services.References to non-CDC sites on the Internet are
provided as a service to MMWR readers and do not constitute or imply
endorsement of these organizations or their programs by CDC or the U.S.
Department of Health and Human Services. CDC is not responsible for the content
of pages found at these sites. URL addresses listed in MMWR were current as of
the date of publication.
All MMWR HTML versions of articles are electronic conversions from ASCII text
into HTML. This conversion may have resulted in character translation or format errors in the HTML version.
Users should not rely on this HTML document, but are referred to the electronic PDF version and/or
the original MMWR paper copy for the official text, figures, and tables.
An original paper copy of this issue can be obtained from the Superintendent of Documents,
U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800.
Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to
mmwrq@cdc.gov.