
|
|
Volume 5: No.
1, January 2008
COMMUNITY CASE STUDY
Expanding the Delivery of Clinical Preventive Services Through Community Collaboration: The SPARC Model
Douglas Shenson, MD, MPH, William Benson, Andree C. Harris
Suggested citation for this article: Shenson D, Benson W, Harris AC. Expanding the delivery of clinical preventive services through community collaboration: the SPARC model. Prev Chronic Dis 2008;5(1).
http://www.cdc.gov/pcd/issues/2008/
jan/07_0139.htm. Accessed [date].
PEER REVIEWED
Abstract
Background
Population-based rates of adult vaccinations and cancer screenings are low, with less than 40% of older adults up to date with routinely recommended prevention services. Delivery rates are lower still in poor and minority communities.
Context
During the past 10 years, Sickness Prevention Achieved through Regional Collaboration (SPARC), a New England–based nonprofit agency, has developed a promising model for increasing community-wide delivery of prevention services. However, the SPARC
model has not been tested in communities elsewhere. In 2006, the Centers for
Disease Control and Prevention facilitated a partnership
between SPARC and the Aging Services division of the Atlanta Regional Commission to evaluate the program’s replicability.
Methods
SPARC coalitions involving local public health agencies, hospitals, social service organizations, and advocacy groups were established in two counties of the region, with
the Atlanta Regional Commission providing regional coordination. Using the SPARC model, the coalitions planned, marketed, and implemented community-based activities to deliver adult screenings and vaccinations.
Consequences
During a 3-week pilot phase, SPARC clinics were held in central Atlanta at three senior housing facilities, a local fire station, and a charter middle school, delivering 353 prevention services to
314 residents. In Fayette County, 634 people received influenza vaccinations on Election Day at SPARC clinics
located near 10 polling places.
Interpretation
The
SPARC model provides a practical framework for improving the community-wide delivery of disease prevention services. The model can galvanize local health services providers to develop successful locally tailored interventions, and the approach is applicable in communities outside of SPARC’s home region.
Back to top
Background
Despite rigorous documentation of the benefits of vaccinations and screening
for chronic diseases, coverage rates remain low. The U.S. Preventive Services Task Force
(USPSTF), an independent national panel of private-sector experts in prevention and primary care, has been reviewing and updating guidelines for preventive service delivery for 23
years (1). The task force does so for a good reason: clinical preventive services hold the promise of preventing or mitigating the impact of many major causes of death in the United States.
Some measures are more effective than others. Vaccinations against influenza and pneumococcal disease and screening for cancers of the breast, cervix, and colon, as well as
identifying people at risk for cardiovascular disease through screening for
hypertension and hypercholesterolemia, all receive a “priority” score from the task force.
Adults aged 65 or older have a higher risk of morbidity and mortality from
influenza. For older persons not living in nursing homes or chronic-care
facilities, influenza vaccine is 30% to 70% effective in preventing
hospitalization for pneumonia and influenza (2,3). Biannual mammography
significantly decreases breast cancer mortality through early detection and
treatment (4). Screening can reduce the risk of death from colorectal cancer by
59% (5). These services form a group of interventions that are recommended on
the basis of a person’s age and sex, and may benefit the entire population of older Americans. Moreover, each of the services is covered by Medicare and most other health insurance plans.
The effectiveness and availability of routine prevention makes the low coverage rate of routine prevention measures all the more striking. Recent analysis showed that in 2004 no more than 25% of adults between the ages of 50 and 64 had received the set of vaccinations and cancer screenings
given a "priority" score by the USPSTF and that less than 40% of those aged 65
or older were up to date
with these measures (6). The
up-to-date rates are lower still for elderly black and Hispanic populations, including, for example, uninsured or low-income Hispanic or Latino populations in Atlanta, Georgia (7).
Back to top
Context
Policy makers have for a long time looked to the doctor’s office as the critical venue for delivery of preventive services. Important initiatives have been developed to reduce barriers to their delivery,
such as shortcomings in physician training, conflicting preventive care recommendations, inadequate office management systems, and lack of knowledge or motivation among patients. These
initiatives have
had mixed success (8,9). Because a large part of the target population for preventive services is either healthy or uninsured
and therefore less likely to visit health care facilities, what has been missing in the U.S. approach is a public health delivery strategy that extends beyond the clinical setting. During the past 10 years, a New England–based agency has developed a promising model for achieving greater community-wide delivery of
preventive services.
Sickness Prevention Achieved through Regional Collaboration (SPARC) is a nonprofit organization devoted to overcoming critical roadblocks to higher delivery rates
of preventive services. The health care system relies almost entirely on doctors — that is, the “sick care” system — to vaccinate and screen entire communities. SPARC’s goal is to
make use of untapped opportunities to deliver
preventive measures across the community. The program has been active in a four-county region at the junction of Connecticut, Massachusetts, and New York (Berkshire, Columbia, Dutchess, and Litchfield counties). The area is primarily rural, but includes two small cities, Poughkeepsie, New York, and Pittsfield, Massachusetts.
SPARC’s approach is to enlist collaboration among providers, local government agencies, community groups, and others to use existing community resources for delivery of preventive care. SPARC does not itself deliver clinical preventive services but creates, coordinates, facilitates, and monitors community-wide strategies to increase the use of immunizations and disease screening. Rather
than view the physician-patient encounter as the beginning and end of a delivery system, SPARC’s approach regards the physician practice as only one element in a community-wide network of activities. Figure 1
describes the current model for delivery of preventive services and Figure 2,
the SPARC model. Because the organization’s collaborators include local and regional preventive care providers, services are not duplicated — activities are created,
consolidated, and coordinated by providers already at work in the area.
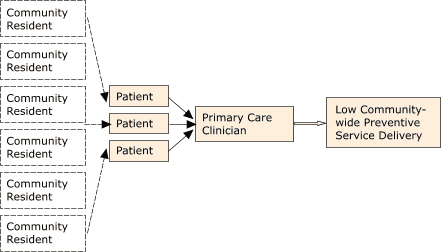
Figure 1. Current model for delivery of preventive services. [A text description of this flowchart is also available.]
Figure 2: SPARC model for delivery of preventive services. [A text description of this flowchart is also available.]
SPARC’s initiatives have successfully increased the use of influenza vaccinations, pneumococcal vaccinations, hepatitis B vaccinations, tetanus boosters, colorectal cancer screening, and mammography in its home communities. In 1997, SPARC led a broad program to ensure the delivery of pneumococcal vaccinations (PPV) at all community
influenza vaccination clinics in two of its counties. Using
Medicare reimbursement data, SPARC doubled the annual prevalence of PPVs delivered in both counties (10).
An innovative SPARC initiative delivered hepatitis B vaccinations at public high schools.
Another
surveyed homebound seniors receiving home-delivered meals to facilitate delivery
of prevention services. In 1995, SPARC piloted a “Vote and Vax” program for Litchfield County to evaluate the feasibility of
delivering influenza vaccinations near polling places (11). With the support of the Robert Wood Johnson Foundation, SPARC built on this work by leading multistate Vote and Vax programs in 2004 and 2006 (12).
SPARC also offered mammography appointments at influenza vaccination clinics
to women who were behind schedule for breast cancer screening. The idea was to bundle these
two services. This simple innovation doubled mammography rates among women attending the
influenza
vaccination clinics (13). Uninsured women received financial assistance to pay
for mammograms from a statewide health program for low-income women. The approach has been used across SPARC’s region (14). In 2001, SPARC developed a mechanism to redistribute influenza vaccine
among mass immunizers (e.g., public health clinics, drug stores, and grocery stores that administer vaccines to the public) and
physician practices to ensure broader immunization of high-risk patients (15).
SPARC’s successful results were described by the director of the
Centers for Disease Control and Prevention's (CDC’s) National Center for Chronic Disease Prevention and Health Promotion before the Special Committee on Aging of the United States Senate (16) and have been cited by the agency’s Healthy Aging Program as a potential national model (17). In doing so, CDC raised an important question: Is the SPARC model practicable
in communities elsewhere?
To address the question, in 2006 CDC facilitated a partnership between SPARC and the Aging Services division of the Atlanta Regional Commission (ARC). This agency’s organizational profile appeared well-suited to hosting a SPARC initiative. As the Area Agency on Aging (AAA), ARC collaborates with county-based agencies, other government agencies, nonprofit organizations, and businesses to
design and implement an array of programs to serve older adults and caregivers. Through contracts with 10 county-based aging programs and 13 specialized agencies to provide home and community-based services, ARC delivers and coordinates information, resources, and services to older residents in its 10-county area.
The goal of the initiative was to evaluate whether an AAA such as ARC could
serve as an effective platform for launching a successful program based on the SPARC model.
Back to top
Methods
In February 2006, ARC invited SPARC leadership to describe the program to approximately 20 health and social-sector leaders from several counties in the Atlanta region. The discussion emphasized four key elements in the model: 1) the importance of selecting preventive services for which there is strong evidence of effectiveness, 2) the need for population-wide strategies to increase their
delivery, 3) opportunities for delivering or facilitating access to these services outside the traditional clinical setting, and 4) the adaptability of the program to the local health care and social service environments.
During the presentation, SPARC reviewed the percentages of men and women aged 65 or older
in the nation and the state who are up to date with
routine preventive services. In Georgia in 2004, these rates were 38% for men and 32% for women (18).
This initial meeting led to a commitment to launch a pilot SPARC program in the Atlanta area. Representatives from county-level aging services in Fulton and Fayette counties indicated that they would like to participate in the pilot activity and were selected primarily on that basis. Fulton County, which includes downtown Atlanta
and comprises 529 sq miles, has a population of approximately 960,000
(51.6% white, 42.9% black, 7.4% Hispanic) and a median household income of $45,819;
approximately 7.6% of the population is aged 65 or older. Fayette County (197 sq miles), a semirural area south of Fulton County, has a population of approximately 107,000 (78.4% white, 17.0% black, 3.7% Hispanic) and a median household income of $75,679;
approximately 10% of the population is aged 65 or older.
Estimates for the delivery of disease prevention services to older residents in the Atlanta region are not available at the county level. However, a region-wide survey
conducted in 2006 estimated that only 44% of older residents received an
influenza vaccination in the past year, 42% received a pneumococcal vaccination,
25% received screening for colorectal cancer in the past 2 years, and 65% of
older women received a routine mammogram within the past 2 years (19).
Coalitions were established in these two counties with ARC acting as regional coordinator. The
primary goal of the pilot program was not primarily to deliver large numbers of preventive services or to seek improvements in population health but to evaluate whether the SPARC model might be applicable in this urban and semirural setting. The
study populations would be adults aged 55 or older living in
target areas of the two counties who were likely not to have received all routinely recommended clinical preventive services.
Resources
ARC provided no funding to the local coalitions. However, it made several in-kind resources available, including ARC staff members and posters. Technical assistance for planning, implementation, and evaluation was purchased from the New England–based SPARC program through a 12-month contract. The local SPARC coalitions raised modest funds for miscellaneous expenses. All revenues
generated by the delivery of services were retained by the local agency members who provided the care. Two representatives from CDC’s Healthy Aging Program provided guidance for ARC and the county SPARC coalitions, but CDC did not supply funding for the program.
The SPARC coalitions established in Fulton and Fayette counties were to develop and implement local strategies for increasing access to clinical preventive services. The respective county offices on aging were designated by ARC as the coalition facilitators; other coalition members brought local knowledge of their communities and a preexisting network of relationships with potential
collaborators. The local public health departments were the primary providers of essential services; other key stakeholders included local hospitals, social service agencies, visiting-nurse agencies, and advocacy organizations. Participating agencies are listed in Acknowledgments.
Planning
The SPARC coalitions began by tackling a set of operational issues. An initial task was
for the initiative to establish the geographic boundaries of the communities they would serve and identify the populations to be targeted. These decisions helped determine which other partners should be invited to participate. The coalitions also determined which clinical preventive services would be
offered. SPARC guidelines included only measures recommended by the USPSTF.
Finally, the coalitions were asked to select community locations from which preventive services would be offered. The Fulton County coalition recognized that those living in congregate sites
such as low-income senior housing apartments have a potentially ready infrastructure for access to services and
could be drawn to prevention services
offered on the premises by education and enticement. In Fayette County, the coalition concluded that people living in single-family homes that are geographically scattered, or who may have limited mobility, would be attracted by access to the services, such as at polling places.
The Fulton County coalition determined that preventive services would be offered in the lobbies of three Atlanta Housing Authority
(the Authority) senior housing apartment buildings, representing 24% (411) of seniors housed by the Authority. Using a mechanism developed by SPARC, women attending the clinics would be offered the opportunity to receive a scheduling telephone call from a radiology facility of
their choice. The Fayette County coalition adopted SPARC’s Vote and Vax program as the centerpiece of its effort. Fayette County also planned a Senior Services Health Fair, where a variety of vaccinations and disease screening services would be available.
The SPARC coalitions met monthly, refining their approach as new members joined and as obstacles or opportunities emerged. Tactical matters included deciding which of the selected services would be offered at each delivery location, reviewing the scheduling and distribution of SPARC clinic sites so that they would be scheduled evenly through the season, determining transportation needs for
disabled community residents, and ensuring that medical referrals or follow-up would be available for people with positive screening results. The coalitions identified appropriate referral networks for screening follow-up, including options for adults without health insurance.
Communications
|
 |
| Figure 3. Vote and Vax
outreach poster, Fayette County, Georgia, 2006. |
|
Each of the SPARC coalitions developed a communications plan for its work. These plans were designed to help get the word out about program activities and to encourage members of the community to participate. The plans drew on SPARC’s experience in launching successful outreach activities for adult vaccinations in its home region. In addition, the Atlanta coalitions recognized that
offering disease prevention services alone was unlikely to attract large numbers of community participants. Each coalition therefore identified ways to attract people to service locations. In Fulton County, the coalition organized a farmers market offering fresh produce at senior housing sites and also recruited a podiatry program to provide free foot massages to seniors. In addition, the SPARC
coalition decided to make a particular effort to invite men to the program and arranged for the public health department to offer a presentation called “Let’s Talk About Sex,” which provided information about the prevention of sexually transmitted diseases. Print pamphlets, flyers, and posters were distributed. In Fayette County, posters and flyers (Figure 3) were used to
advertise the availability of influenza vaccinations near selected polling places.
Back to top
Consequences
During a 3-week pilot implementation phase (November 14–December 5), clinics were held in central Atlanta at three senior housing facilities, a local fire station, and a middle school. The initiative delivered 189 influenza and 49 pneumococcal vaccinations, as well as 44
tetanus booster shots. Approximately 62% of adults receiving an
influenza vaccination stated they had not received
one in the previous 12 months, and 56% thought it “not very likely” or were “not sure” that they would have received an
influenza vaccination if they had not had one at a SPARC clinic site. Each of the clinics also provided screening for diabetes (43 total), as well as access to mammograms for women older than 40 who had not received screening in the past 12 to 24 months (32
appointments were scheduled). A total of 314 residents were served, 138 (44%) men and 176 (56%) women. Approximately one-third of clients were aged 65 or older, 40% were aged 50 to 64, and 28% were aged 18 to 49.
In Fayette County, 634 influenza vaccinations were delivered at Vote and Vax clinics situated near 10 polling places. Approximately 83% of recipients were in influenza vaccine priority groups (aged 50 or older, or aged 18
to 49 with elevated risk factors); 61% were men,
and 39% were women
(Table). Approximately 27% of the recipients had not received an influenza vaccination in the past 12
months. PPV was also provided at Vote and Vax clinics (Figure 4). Approximately 96% of the vaccine recipients had Medicare, Medicaid, or other health insurance coverage. At the Fayette County Senior Health Fair, held at a local church, several preventive services were offered to attendees, including influenza and pneumococcal vaccinations; referrals for breast cancer and
colorectal cancer screening; and screening for diabetes, hypertension, and osteoporosis.
Figure 4. Receipt of pneumococcal vaccination among
adults aged ≥65 at Fayette County, Georgia, Vote and Vax Clinics, November 2006. [A tabular version of this figure is also available.]
Back to top
Interpretation
The results of this pilot initiative show that SPARC does provide a practical and appealing framework for improving delivery of clinical preventive services and can assist local service providers
in developing community-tailored interventions. New community-based sites for delivering prevention services were established in both counties, and new combinations of disease prevention services were
made available at these sites. The organization’s approach worked effectively with local service providers and helped establish new partnerships
among them. For example, this effort represented the first time that the Atlanta Housing Authority and the county aging offices worked together. SPARC’s work was perceived as being both in the interest of the community and to the advantage
of local agencies because the program increases the number of people who receive care. At
the completion of the pilot implementation phase, SPARC coalitions in both counties decided to continue and expand their work in the coming year.
The leadership of ARC’s Area Agency on Aging was a critical element in the success of the pilot. The effectiveness of the commission not only reflects the skills of ARC’s individual AAA team members but also highlights the importance in the SPARC model of having a central coordinating entity that takes responsibility for managing the program. The work of the county-level SPARC
coalitions demonstrated how a committed group of collaborators can tailor SPARC’s general approach to the needs and opportunities present in their own communities. The SPARC coalitions developed an imaginative and well-received set of social marketing strategies and were able to identify untapped community resources — senior housing and neighborhood polling places — from
which to launch the program.
The results of this initiative represent a beginning; more work remains to be done. In reviewing activities at the completion of the pilot phase, several limitations were noted. SPARC coalition members identified a need for additional funding to allow the development of a more extensive outreach and marketing effort. Coalition members also highlighted the importance of developing local
data-gathering and surveillance systems that can monitor population-wide coverage of clinical preventive services. Some collaborators also saw the importance of developing SPARC initiatives that are more extensively integrated with local medical providers. More systematic collection of qualitative data on various program elements would be useful in future efforts to replicate the program.
The experience of the Atlanta pilot program suggests that AAAs may represent an important vehicle for replication of SPARC elsewhere. There are 655 AAAs nationwide; all but a handful of states with small populations have AAAs covering all areas of the state. Several key attributes of AAAs are essential to the SPARC model. They have an established infrastructure with annual funding under the
Older Americans Act (OAA). As part of the “aging network” of federal, state, and local agencies, AAAs support a diverse array of community-based services within their geographical boundaries. Although AAAs work closely with the health care community, they do not provide clinical preventive services. Having been mandated by OAA to support and promote preventive services (20), AAAs have increased their
support for evidence-based prevention services in recent years, with the encouragement of the federal Administration on Aging.
The lifesaving potential of expanding access to cancer screenings and vaccinations is significant. In 2001, cancer began to surpass heart disease as the leading cause of death for persons younger than 85 years (21). Influenza and pneumonia, for which vaccinations are available, are together the fifth leading cause of death in the population aged 65
or older. Indeed, widespread immunization
and screening with appropriate follow-up has repeatedly been shown to be the most cost-effective strategy for
reducing the death rate of these diseases (22,23). Access to prevention services must be broadened to encompass the whole community. Protecting
the population from preventable disease is a
goal that will require the participation of medical, public health, and advocacy organizations.
Applying the SPARC model in more communities may advance this goal.
Back to top
Acknowledgments
Participating Agencies: American Cancer Society; American Heart Association and American Stroke Association; Atlanta Housing Authority; Atlanta Regional Commission;
Avon Foundation Breast Cancer Awareness Initiative;
Digestive Healthcare of Georgia; East Point Fire Department; East Point Police Department; East Point Community; Fayette Care Clinic; Georgia
Cares; Georgia State University; Fayette County Health Department; Fayette Senior Services; Fulton County Department of Health and Wellness; Grady Hospital; Grady Senior Services; Health First Medical Supplies; Historic District Development Corporation; Maxim Healthcare Services; Piedmont Fayette Hospital; Piedmont Physicians; Project Open Hand; South Fulton Medical Center; South Fulton Senior Services;
Southern Home Care Services; Visiting Nurse/Hospice Service, LLC; West End Medical Centers;
East Point NORC (Naturally Occurring Retirement Community) Project.
Back to top
Author Information
Corresponding Author: Douglas Shenson, MD, MPH, SPARC (Sickness Prevention Achieved through Regional Collaboration), 76 Prince St, Newton, MA 02465.
Telephone: 617-796-7966. E-mail: dshenson@sparc-health.org.
Author Affiliations: William Benson, Health Benefits ABCs, Wheaton, Maryland;
Andree C. Harris, Centers for Disease Control and Prevention (CDC), Atlanta, Georgia.
Back to top
References
- U.S. Preventive Services Task Force. Rockville (MD): Agency for Healthcare Research and Quality.
http://www.ahrq.gov/clinic/uspstfab.htm. Accessed May 9, 2007.
- Mullooly JP, Bennett MD, Hornbrook MC, Barker WH, Williams WW, Patriarca PA, et al.
Influenza vaccination programs for elderly persons: cost-effectiveness in a health maintenance organization. Ann Intern Med 1994;121(12):947-52.
- Nichol KL, Wuorenma J, von Sternberg T.
Benefits of influenza vaccination for low-, intermediate-, and high-risk
senior citizens. Arch Intern Med 1998;158(16):1769-76.
- U.S. Preventive Services Task Force Recommendations. Ann Intern Med 2002;137(Part 1):344-6.
- Selby JV, Friedman GD, Quesenberry CP Jr, Weiss NS.
A case-control study of screening sigmoidoscopy and mortality from colorectal cancer.
N Engl J Med 1992;326(10):653-7.
- Shenson D, Bolen J, Adams M.
Receipt of preventive services by elders based on composite measures, 1997–2004. Am J Prev Med 2007;32(1):11-8.
- Asamoa K, Rodriguez M, Ginés V, Varela R, Dominguez K, Mills CG, et al.
Report from CDC. Use of preventive services by Hispanic/Latino women in two urban communities: Atlanta, Georgia and Miami, Florida, 2000 and 2001. J Women’s Health (Larchmt) 2004;13(6):654-61.
- Yeazel MW, Bunner SH, Kofron PM, Weiss PJ.
Put prevention into practice (PPIP): evaluating PPIP in two family practice residency sites. Fam Med 2002;34(1):17-22.
- Gottlieb NH, Huang PP, Blozis SA, Guo JL, Murphy Smith M.
The impact of Put Prevention into Practice on selected preventive services in five Texas sites. Am J Prev Med 2001;21(1):35-40.
- Centers for Disease Control and Prevention.
Local data for local decision making — selected counties, Connecticut, Massachusetts, and New York, 1997.
MMWR Morb Mortal Wkly Rep 1998;47(38):809-13.
- Shenson D.
Putting prevention in its place: the shift from clinic to community. Health Aff
(Millwood) 2006;25(4):1012-5.
- Vote and vaccinate: grant results. Princeton (NJ): Robert Wood Johnson
Foundation.
http://www.rwjf.org/reports/npreports/vote.htm.* Accessed August 20, 2007.
Updated October 2006.
- Shenson D, Cassarino L, DiMartino D, Marantz P, Bolen J, Good B, et al.
Improving access to mammograms through community-based influenza clinics. A
quasi-experimental study. Am J Prev Med 2001;20(2):97-102.
- Cormier LF, Benfer RW, Shenson D. Expanding access to mammograms for older
rural women: SPARC’s community-wide approach to delivery clinical preventive
services. The 2005 Aetna Susan B. Anthony Award for Excellence in Research
on Older Women in Public Health. 133rd APHA Annual Meeting. Philadelphia,
Pennsylvania. December 2005.
- DiMartino D, Cassarino L, Boy A, Shenson D. Redistribution of influenza vaccine between mass immunizers and physician practices to assure immunization of high-risk patients.
Proceeding of the 35th Annual National Immunization Conference. 2001 May 29−June 1; Atlanta, Georgia.
- Marks J. Director of the CDC's National Center for Chronic Disease
Prevention and Health Promotion, before the Special Committee on Aging of
the United States Senate, Testimony before Congress: May 19, 2003.
http://www.cdc.gov/washington/testimony/ag051903.htm. Accessed September
27, 2007.
- Lang JE, Moore MJ, Harris AC, Anderson LA. Healthy aging: priorities and programs of the Centers for Disease Control and Prevention: public health at the federal level. Generations 2005;29(2):24-9.
- Shenson D, Bolen J, Adams M.
Receipt of preventive services by elders
based on composite measures, 1997-2004. Am J Prev Med 2007;32(1):11-8.
- Older adults in the Atlanta region: preferences, practices and potential of the 55+ population.
Atlanta (GA): Atlanta Regional Commission; 2007.
http://www.atlantaregional.com/cps/rde/xchg/ arc/hs.xsl/470_ENU_HTMLhtm.* Accessed
October 30, 2007.
- Disease Prevention and Health Promotion Services Act, 42 USC §3030.
- Jemal A, Murray T, Ward E, Samuels A, Tiwari RC, Ghafoor A, et al.
Cancer statistics, 2005.
[Published erratum in: CA Cancer J Clin 2005;55(4):259]. CA Cancer J Clin 2005;55(1):10-30.
- Cai L, Uchiyama H, Yanagisawa S, Kamae I.
Cost-effectiveness analysis of
influenza and pneumococcal vaccinations among elderly people in Japan. Kobe J
Med Sci 2006;52(3-4):97-109.
- Weaver M, Krieger J, Castorina J, Walls M, Ciske S.
Cost-effectiveness
of combined outreach for the pneumococcal and influenza vaccines. Arch Intern
Med 2001;161(1):111-20.
Back to top
|
|
