
Volume 5: No.
2, April 2008
SPECIAL TOPIC
Prehospital and Emergency Department Capacity for
Acute Stroke Care in Minnesota
Albert Wu Tsai, PhD, MPH
Suggested citation for this article: Tsai AW. Prehospital and emergency department capacity for
acute stroke care in Minnesota. Prev Chronic Dis 2008;5(2).
http://www.cdc.gov/pcd/issues/2008/
apr/07_0212.htm. Accessed [date].
PEER REVIEWED
Abstract
Introduction
Stroke is the third leading cause of death in Minnesota. One strategy to reduce the burden of stroke is to implement systems-level improvements in the prehospital and acute care settings. Two surveys conducted in 2006 obtained information about current practices and capacities of emergency medical services and emergency departments in Minnesota.
Methods
In 2006, the Minnesota Department of Health and the Minnesota Stroke Partnership (the statewide stroke collaborative group) conducted two surveys. The survey for emergency medical services organizations, mailed to every licensed ambulance service in Minnesota, asked about transportation policies and training needs. The survey for hospitals, mailed to every hospital in the state, asked about capacity to treat
acute stroke. Results were calculated using simple frequency analyses.
Results
Of 257 surveys mailed to ambulance services, 199 (77%) were returned. Ambulance services generally considered stroke an emergency. Training on stroke
was reported most effective in person annually or semiannually. Of 133 surveys mailed to hospitals, 120 (90%) were returned. Stroke capacity differed markedly between hospitals in rural areas and hospitals in the large Minneapolis–St. Paul metropolitan area. Many hospitals, particularly small hospitals,
reported lacking stroke protocols. Training for stroke is needed overall but particularly in small hospitals.
Conclusion
Transport and treatment of people with acute stroke in Minnesota vary by hospital size and location. Standardization of transport and protocols for acute treatment may increase efficiency and overall care for stroke patients. In addition, the need
to train ambulance personnel and emergency departments about stroke remains high.
Back to top
Introduction
In the United States, an estimated 700,000 strokes occur annually (1). Although Minnesota
is consistently rated one of the healthiest states in the nation (2), stroke is a major cause of death and disability for Minnesotans. In 2005, 2372 people died from stroke, making it the third
leading cause of death in the state (3). In addition, approximately 11,000 hospitalizations for stroke occur annually, with estimated costs exceeding $266 million (Minnesota Department of Health, Minnesota Hospital Discharge Dataset, unpublished data, 2005).
The American Heart Association recently released recommendations for comprehensive systems of stroke care (4). These include establishing processes to provide rapid access to emergency medical services (EMS) for people with
acute stroke and promoting the use of transport and treatment protocols by EMS personnel. In addition, hospital care for
acute stroke should include strategies to ensure appropriate and efficient triage and treatment of stroke patients and use of clinical pathways (i.e., procedures and protocols outlined through a decision tree, usually provided on a paper
document attached to a medical chart). The Minnesota Stroke Partnership (MSP) — a coalition of stroke care professionals, advocates, and others interested in stroke prevention and treatment representing various health care delivery organizations in Minnesota — considers prehospital transport and treatment and emergency care as priority systems. MSP works with the Minnesota Department of Health (MDH) to plan and implement systems-level changes. Because these systems had not been formally assessed to determine gaps or needs, MSP and MDH conducted two surveys to assess the
preparedness and capacity of these systems.
Back to top
Methods
Minnesota Emergency Medical Services Stroke Care Survey
A survey of EMS directors was developed in 2006 with input from MSP members to collect information about prehospital stroke care capacity and practices among Minnesota ambulance services. The survey also provided information to MSP about stroke training needs and effective methods to train and educate EMS personnel.
A sample of ambulance directors beta-tested the 23-question survey. The MDH Institutional Review Board approved the final survey tool in May 2006. The list of recipient ambulance services was obtained from the Minnesota Emergency Medical Services Regulatory Board. EMS agencies providing only air transport or facility-to-facility transport services were excluded because this survey focused on ground transport issues.
In June 2006, the survey tool, along with a cover letter written jointly by the MSP and MDH,
was sent to the 240 directors overseeing all 257 ambulance services in the state. Respondents were given the option to complete the survey online. Two follow-up letters were sent to ambulance services not responding within 6 weeks. A total of 199 (77% response rate) surveys were completed. The survey closed in August 2006. A copy of the survey is available at
http://www.health.state.mn.us/cvh*.
Minnesota Acute Stroke Treatment System Survey
MSP members with expertise in clinical stroke care developed the survey of hospitals. Questions were based on recommendations from the Brain Attack Coalition for stroke centers (5) and from the American Stroke Association Stroke Systems of Care (4) planning committee for Minnesota. The MDH Institutional Review Board approved the final survey of 22 questions in October 2005. The list of recipient hospitals was obtained from the MDH Facility and Provider Compliance Division Web site
(www.health.state.mn.us/divs/fpc/fpc.html*). The survey excluded hospitals that serve primarily children or otherwise are specialty care facilities (e.g., rehabilitation hospitals) because this assessment focused on adults receiving acute care.
Every hospital was contacted by telephone to determine the best recipient of the survey. Recipients were mostly directors of nursing or quality improvement. The survey,
along with a cover letter written jointly by MSP and MDH, was sent to 133 acute care hospitals in January 2006. Respondents were given the option to complete the survey online. Two follow-up letters were sent to hospitals not responding within 6 weeks. Hospitals that did not return the second follow-up survey were contacted by
telephone to conduct the survey. A total of 120 (90%) of 133 hospitals responded. Nineteen hospitals within the seven-county Minneapolis–St. Paul metropolitan area (“Twin
Cities metro area”) responded, compared with 101 rural (non-metro and small metro area) hospitals. Of the 13 hospitals not responding to the survey, 11 reported fewer than 100 beds, and 11 are located outside the Twin Cities metro area. The survey closed in April 2006. A copy of the survey is available at www.health.state.mn.us/cvh*.
Data analysis
Data for both surveys were analyzed by size of hospital (according to number of licensed beds) and location (Twin
Cities metro and rural). Hospitals were grouped into the following categories: small (<50 beds [n = 75]), medium (50–99 beds [n = 17] and 100–249 beds [n = 9]), and large (≥250 beds [n = 19]).
Back to top
Results
Minnesota Emergency Medical Services Stroke Care Survey
Stroke patient transportation and advance notification
Fewer than two-fifths (37%) of respondents reported the existence of a written transportation protocol for stroke patients (Table 1). Most (91%) would not bypass a hospital to send a patient to a destination with greater capacity for stroke care; according to written comments, ambulances take patients to a hospital chosen by the patient or patient’s family. Most ambulances (78%) provide advance notice to hospitals about
stroke patients needing urgent care, with notification on scene (10%), immediately en route (21%), or as soon as possible en route (54%); the questionnaire did not define the difference between “immediately” and “as soon as possible.” Ten percent of ambulance services alert the destination hospital within 5 minutes before reaching it. Air transport is used infrequently; 70% never use a helicopter.
Prehospital care and management
Seventy-six percent of services have a written protocol for prehospital stroke management (Table 2). The Cincinnati Stroke Scale
(5) (or some modification of it) is the most commonly used stroke scale assessment tool. The stroke scale score is reported to hospital staff “sometimes” in 21% of cases, “always” in 34% of cases, and “rarely” or “never” in 36% of cases;
9% of respondents did not know whether the stroke scale score is reported to
hospital staff.
Stroke training for EMS
A majority of respondents reported their personnel are trained on stroke at
least once a year (119 [60%]) (Table 3). Nearly one-third (60 [30%]) reported
their personnel receive stroke training once every 2 or 3 years. Classroom training was the most commonly cited format,
followed by DVDs or videos (Table 3). Other types of training reported include
run reviews and Advanced Cardiac Life Support refresher courses (6). Most
respondents reported offering training opportunities annually (56%) or
semiannually (24%) is most effective.
Forms of training reported most often as most effective include
agency-sponsored conferences and seminars, regional conferences, Internet-based
training, and statewide conferences (Figure). Agency-sponsored conferences or
seminars was the kind of training most commonly reported effective for Emergency
Medical Technician (EMT)-Basic (79%) and, to a lesser degree (32%), for
paramedics. This form of training also was reported as effective for paramedics (32% of responses). Internet-based training was the second most common method for
paramedics (22%), with regional (18%) and statewide (16%) conferences cited about equally. Teleconferences, videoconferences, and national conferences were least frequently cited as effective training vehicles.
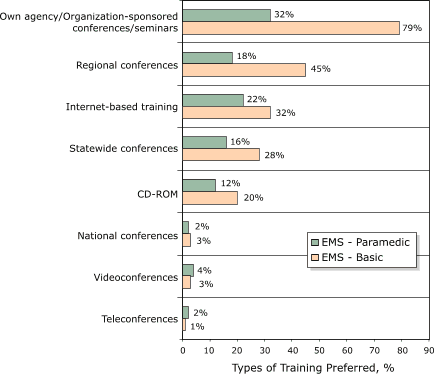
Figure. Percentage of types of training deemed most
effective by
emergency medical services (paramedic and basic) staff, Minnesota Emergency Medical Services Stroke Care Survey, 2006.
Respondents were instructed to indicate (by checking) as many types as they
wished. [A tabular version of this figure is also available.]
Minnesota Acute Stroke Treatment System Survey
Emergency departments
Eighty-four percent of the largest hospitals reported having written emergency department (ED) care protocols for acute stroke diagnosis or treatment, compared with 43% of small hospitals (Table 4). Fifty-two percent of rural hospitals have ED protocols. Of the hospitals with written stroke care protocols, 10 (17%) use telemedicine.
ED staff in approximately 80% of medium and large hospitals receive training for acute stroke diagnosis and treatment, compared with 60%
of small hospitals and 65% of rural hospitals. Most of the hospitals with a stroke team are based in the Twin Cities metro area. One hundred twelve (93%) hospitals reported the ability to provide around-the-clock laboratory services, with expedited results within 45 minutes.
Among the rural hospitals, 16% do not have computerized tomography (CT) scan
or a CT technician available around the clock (Table 4). Of the 17 hospitals that do not have access to a neurologist for consultation on stroke cases, all but one were rural hospitals; four hospitals reported having access to a neurologist for consultation during specific hours of the day.
Inpatient care
Approximately 27% of small, 58% of medium-sized, and 35% of rural hospitals have written inpatient protocols for managing stroke patients (Table 5). Fewer than 20% of small hospitals have a “stroke code” (alert system for hospital staff to respond to an inpatient stroke). Most (56) of the 60 hospitals that do not provide coordinated stroke care have fewer than 100 beds. Nearly every hospital that indicated not providing such coordinated stroke care
reported being prepared to transfer stroke patients to an appropriate hospital for such care. Eight percent of rural hospitals, compared with 68% of
Twin Cities metro hospitals, have a designated ward for stroke patients.
Quality improvement, education, and primary stroke center certification
At the time of the survey (January 2006), the Joint Commission had certified six
Twin Cities metro hospitals as Primary Stroke Centers.
Forty-four (37%) hospitals reported their staff had sufficient opportunity to receive at least 8 hours each year of stroke education and training (Table 6). Staff in 10 (16%) of the 63 smallest hospitals have such an opportunity. About half of hospitals with 100 or more beds provide public education; 7% of small hospitals and 31% of medium-sized hospitals provide public education on stroke at least twice a year. Twenty percent of small hospitals and 42% of medium-sized hospitals have a database
for tracking quality information. One-fourth of hospitals reported having a stroke champion working within the hospital as an advocate for improving stroke care.
Hospitals were asked to name their priorities for stroke, and written responses were grouped (Table 7). Development of protocols, standing orders, or pathways (31% overall) were most commonly reported, followed by early identification or assessment of stroke patients (20%) and staff education on stroke (19%). Other responses included rapid intervention or use of tissue plasminogen activator (tPA) (14%) and rapid transfer of stroke patients (13%) (Table 7).
Stroke hospitalizations and tPA questions
Seventy-two (61%) of 118 hospitals reported administering intravenous tPA for acute stroke treatment. Among
the 74 small hospitals, 35 (49%) administer tPA, compared with 19 (73%) of 26 medium hospitals and 17 (89%) of 19 large hospitals. Among rural hospitals, 56 (56%) of 99 administer tPA, compared with 17 (89%) of 19
Twin Cities metro hospitals.
Back to top
Discussion
The Minnesota Emergency Medical Services Stroke Treatment Survey 2006 provided valuable information about current opinions
on stroke, transport and treatment practices, and training format preferences for Minnesota ambulance service personnel. For example, few services reported using a helicopter to transport stroke patients. Although helicopter transport may not be practical within the
Twin Cities metro area because distance and traffic congestion are not significant barriers, services in rural areas
should consider using air transport to reach a hospital within the window for using thrombolytic therapy.
A minority of EMS have a written policy for where to transport patients with acute stroke. Although most hospitals in Minnesota claim to be prepared to either treat or transfer stroke patients, the current practice of transporting to the nearest hospital highlights the need to increase the capacity of hospitals statewide to treat patients with acute stroke according to current clinical practice guidelines.
Respondents reported CD-ROM- or Internet-based training curricula and conferences or seminars as the most effective vehicles for training ambulance personnel. However, no further details were obtained about how effectiveness was assessed.
The Minnesota Acute Stroke Treatment System Survey 2006 identified many areas of strength in stroke care. These include around-the-clock laboratory services and CT scan services, plans for transferring stroke patients in hospitals without coordinated post-ED care, and ability to administer intravenous tPA for treatment of acute stroke. However, much work remains to build an effective and efficient system of care for stroke patients in Minnesota hospitals.
At the time of the survey, only six hospitals had been certified as Primary Stroke Centers; since then, three additional hospitals have been certified. The Joint Commission is an independent, nonprofit organization that accredits and certifies health care organizations and programs in the United States. The Joint Commission Primary Stroke Center certification program is recognized nationwide as a symbol of quality that reflects an organization’s commitment to meeting certain
performance standards.
Limitations of both surveys should be considered in interpreting results. First, accuracy of responses was limited to respondents’ knowledge about stroke practices and capacity. The extent to which respondents queried more informed colleagues to answer questions for which they were unsure is unknown. In addition, self-reported information has the potential for bias toward positive answers when the opposite may be true. Moreover, none of the responses were confirmed by external review
or formal inquiry. Despite their limitations, these data are valuable for planning changes and developing a coordinated system of stroke care in Minnesota.
Implications
The MSP Steering Committee developed the following recommendations for consideration by ambulance services, hospitals, state agencies, and collaborating partner organizations in making systems-level improvements in stroke care. These suggestions and strategies were based on the results of these surveys and on discussion in quarterly meetings during 2006 after the surveys.
Prehospital care
Prehospital EMS personnel should continue to treat stroke as an emergent event.
Because a large proportion of respondents reported that first responders typically provide only vital sign information to ambulance staff about a patient with a suspected stroke, without indicating they suspect a stroke, MSP
and its partners should consider teaching first responders
to recognize the signs of stroke and to communicate such information to ambulance personnel.
MSP and its partners should encourage all ambulance service organizations to use the Cincinnati Stroke Scale as the standard for assessing patients suspected of having stroke. By having all ambulance organizations voluntarily adopt the Cincinnati Stroke Scale, a common standard can be established for training and educating ambulance personnel.
MSP and its partners should inform hospital ED staff that this stroke scale standard is being encouraged, and prehospital providers should include
instructions in their standard operating procedures to always verbally provide
stroke scale information to hospital ED staff. This communication will potentially aid the efficiency of care provided in the destination hospital.
MSP and its partners should inform prehospital EMS providers about the locations of primary stroke centers and educate
them about recent recommendations for stroke systems of care.
MSP and its partners should provide training for prehospital EMS providers on stroke issues annually or semiannually. This training should be offered, but not mandated, for ambulance personnel.
MSP and its partners should provide classroom education or regional conferences and seminars — probably the most effective methods for education and training. Internet-based training also should be provided as an option for continuing education.
Emergency department
Hospitals that do not currently have standing orders for treating acute stroke in the ED
should develop and share protocols. The state agency (MDH), in collaboration with partners, may be in the position to provide technical assistance to ED staff in all hospitals — but especially small and rural hospitals — to aid implementation of protocols and standing orders.
ED protocols in rural hospitals should consider including telemedicine. Relationships should be fostered between appropriate facilities (e.g., hospitals within the same health systems) to help development of telemedicine to improve acute stroke care.
Inpatient care
MSP and its partners should develop care protocols and pathways for inpatient care of stroke patients and share these tools among hospitals, particularly rural hospitals.
Staff at hospitals that do not have a stroke code for inpatient stroke events should be trained on developing and implementing protocols.
Quality improvement and education
MSP and its partners should provide technical assistance and lessons learned to all hospitals that plan to become certified as Primary Stroke Centers by the Joint Commission.
MSP and its partners should provide ongoing stroke training and continuing education opportunities for hospital staff on the following topics:
- Protocol development and implementation
- Evidence-based use of tPA
- Early and rapid assessment of stroke (National Institutes of Health Stroke Scale training)
- Updates and current practices for stroke care
Partner organizations may collaborate with hospital education and outreach departments to develop community-based stroke education efforts, particularly during May (Stroke Awareness Month).
Partners should collaborate on increasing the number of hospital EDs that administer intravenous tPA in appropriate and eligible stroke patients.
MSP and its partners should develop a voluntary hospital network, where purpose, infrastructure, and initiatives are defined and implemented by multiple partners, including the state quality improvement organization, state hospital association, state office of rural health, and the statewide coalition or task force for stroke.
Conclusions
The results of these surveys will guide MDH and MSP in planning for systems-level intervention and programs to improve acute stroke care in Minnesota. In addition, ambulance services and hospitals can use these results to change their health systems to improve the quality of care for their stroke patients. Finally, these surveys highlight the need to develop a statewide or regional system for transportation and treatment of stroke patients to better facilitate coordination between EMS and
hospital care. This system may involve development of formal or informal agreements to divert patients to appropriate facilities, establishment of a structure for providing continuing education to health care providers, and opportunities for health care organizations to improve their overall stroke care capacities.
Back to top
Acknowledgments
This work was supported by cooperative agreement #U50/CCU519109 from the
Centers for Disease Control and Prevention. No other financial contributions
were given for the collection or analysis of the data.
Back to top
Author Information
Albert W. Tsai, PhD, MPH, Minnesota Department of Health, P.O. Box 64882, St. Paul, MN 55164-0882. Telephone: 651-201-5413. E-mail: Albert.tsai@health.state.mn.us.
Back to top
References
- Rosamond W, Flegal K, Friday G, Furie K, Go A, Greenlund K, et al.
Heart disease and stroke statistics−2007 update: a report from the American
Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation 2007;115:e69-171.
- America’s health rankings. 2006 ed. Minnetonka (MN): United Health Foundation;
2006. http://www.unitedhealthfoundation.com/ahr2006/2006ahr.pdf.*
- MN vital statistics interactive queries database: death statistics. St.
Paul (MN): Minnesota Department of Health, Center for Health Statistics; 2005.
https://pqc.health.state.mn.us/mhsq/birth/queryFrontPage.jsp?goTo=deathInterfaceSas.jsp&queryPage= deathInterfaceSas.jsp&startQuery=true.*
- Schwamm LH, Pancioli A, Acker JE 3rd, Goldstein LB, Zorowitz RD, Shephard
TJ, et al.
Recommendations for the establishment of stroke systems of care:
recommendations from the American Stroke Association’s Task Force on the
Development of Stroke Systems. Stroke 2005;36(3):690-703
- The Internet Stroke Center. Stroke scales and clinical assessment tools:
Cincinnati Stroke Scale. http://www.strokecenter.org/trials/scales/cincinnati.html*.
- Advanced Cardiac Life Support. http://www.heart.org/presenter.jhtml?identifier=3011972*.
Back to top
|
