Volume
8: No. 4, July 2011
Zhen Zhang, PhD; Lei Zhang, PhD, MBA; Alan Penman, MD, PhD; Warren May, PhD
Suggested citation for this article: Zhang Z, Zhang L, Penman A, May W. Using small-area estimation method to calculate county-level prevalence of obesity in Mississippi, 2007-2009. Prev Chronic Dis 2011;8(4):A85.
http://www.cdc.gov/pcd/issues/2011/jul/10_0159.htm. Accessed [date].
PEER REVIEWED
Abstract
Introduction
Obesity is one of Mississippi’s pressing public health problems.
Since 2005, the state
has ranked first in the nation in adult obesity prevalence. For authorities to
take targeted
action against the obesity epidemic, counties, regions, and subpopulations that
are most affected by obesity need to be identified. The
objective of this study was to assess the scope, socioeconomic and geographic characteristics, and temporal trends of the obesity epidemic in Mississippi.
Methods
Using 2007-2009 Mississippi Behavioral Risk Factor Surveillance System data and auxiliary data, we applied a small-area estimation method to estimate county-level obesity prevalence in 2007
through 2009, to assess the association between obesity and socioeconomic factors and to evaluate temporal trends. We determined geographic patterns by mapping
obesity prevalence. We appraised the precision of estimates by the width of 95%
confidence intervals, and we validated our small-area estimates by comparing them
with direct estimates.
Results
In 2009, the county prevalence of obesity ranged from 30.5% to 44.2%. Counties with the highest prevalence of obesity
were in the Delta region and along the Mississippi River. The obesity prevalence increased from 2007 through 2009. Age, sex, race, education, and employment status
were associated with obesity.
Conclusion
The 2009 obesity prevalence in all Mississippi counties was substantially higher than the national average and
differed by geography and race. Although urgent intervention measures are needed in the entire state, policies and programs giving higher priority to higher-risk areas and subpopulations identified by this study may be better strategies.
Back to top
Introduction
In the past 25 years, the prevalence of obesity, defined as a body mass index (BMI)
of at least 30 kg/m2, has increased dramatically in the United States; more than one-third of adults are now obese (1-4). Mississippi has ranked first in the nation in obesity prevalence
since 2005. Between 1995 and 2009, the prevalence of obesity in Mississippi
increased substantially, from 19.5% to 35.4% (5), and there is no
indication that this upward trend will level off soon. Obesity is associated with heart disease, diabetes, cancer, asthma, arthritis, stroke, and premature death (6,7). Consequently, obesity and its associated health problems have a substantial social and economic
effect (6,8). According to the Mississippi State Department of Health (9), obesity is one of the state’s most pressing public health problems.
The high and increasing rate of diabetes in the state is highly correlated with the increasing rate of obesity (9,10).
The highest obesity rates should be identified for priority intervention both
because of limited resources and because obesity control programs may be
more effective when tailored according to specific community needs (11,12).
Socioeconomic
characteristics, such as age, sex, race, income, and education, and community
factors such as average per capita income and percentage of labor-intensive workers
are associated with obesity (3,13). In an effort to establish the association of
diabetes with obesity, Centers for Disease Control and Prevention (CDC)
produced 2007 county-level obesity prevalence estimates for 3,141 US counties by
using Bayesian multilevel modeling (10) but did not analyze geographic and socioeconomic
characteristics of
the obesity epidemic for the states. To our knowledge, no studies have focused on providing up-to-date small-area health statistics and related information in Mississippi for prevention and intervention purposes. In this study, we sought to produce reliable county-level
estimates of obesity prevalence for all Mississippi counties, identify geographic heterogeneity and temporal trends, and evaluate associations between obesity and socioeconomic factors.
This information would enable the development of appropriate obesity prevention policies and community interventions.
Back to top
Methods
Data sources
Established by CDC, the Behavioral Risk Factor Surveillance System (BRFSS) is
an ongoing state-based surveillance system tracking health conditions and risk
behaviors among noninstitutionalized adults aged 18 years or older in the United States. The design of BRFSS aims at generating reliable prevalence estimates at
the state level or for large metropolitan statistical areas. Sample size for counties are usually too small for making direct inferences with satisfactory precision. CDC
suggests that a sample size of at least 300 is necessary for direct estimation (14,15). To overcome the limitation of small sample sizes, we developed a
2-step estimation method. This method belongs to a family of small-area
estimation techniques that includes varied approaches for making inferences about geographic or social subdomains of the survey domain. The power of the
small-area estimation method resides on its ability to borrow strength from multiple sources of data
— data collected at other times, or in related areas, or both to increase the effective sample size and thus achieve adequate precision. Among current
small-area estimation methods,
the Hierarchical Bayes approach and generalized linear mixed models have been primary choices
(16-18). We used a generalized linear mixed model in this study. We incorporated
a generalized linear mixed model and traditional synthetic methods to meet the
small-area estimation needs in this study.
We acquired individual-level BRFSS data for Mississippi for 2007 through 2009. Variables included in the analytical dataset
were self-reported height and weight and demographic and socioeconomic variables, including age, race, sex, education level, employment status,
annual household income, and marital status. We used
the Federal Information Processing Standard code as the location variable for county. We categorized BMI as
a binary
variable, obesity (obesity = 0 if BMI <30 kg/m2, obesity = 1 if BMI ≥30 kg/m2). In the original Mississippi BRFSS data, age is a continuous variable. Through initial exploratory data analysis, we found a quadratic relationship between BMI and age. According to the shape of the quadratic regression line, we categorized age into 4 groups: 18
to 29, 30 to 44, 45 to 64, and 65 years or older. We categorized education as less
than a bachelor’s degree and
bachelor’s degree or higher. For employment status, we grouped employed for wages and self-employed as “employed,” and
grouped unemployed temporarily, those unable to work, students, retired people, and homemakers as “unemployed.”
The exclusion criteria were 1) missing Federal Information Processing Standard code information
(n = 39); 2) missing BMI values or biologically unlikely BMI values (BMI <12
kg/m2 or BMI >70 kg/m2)
(n = 1,013); 3) pregnant (n = 138); 4) races other than black and white (n = 383). Taking into consideration that in Mississippi 98.5% of the population belongs to 1 of 2 categories, black alone or combined and white alone or combined
(19), we excluded the small portion (1.5%) of respondents of other races to facilitate small-area estimation.
Respondents who chose black alone or black and
other race(s) were categorized as black alone or combined; respondents who chose white
alone or white with race(s) other than black were categorized as being in the white alone or combined
category. The final analytical dataset of 2007-2009 BRFSS had 25,046 observations.
The data sources for auxiliary information were the 2000 US Census (19) and the US Department of Agriculture Economic Research Service (20). We used the auxiliary information to construct predictor variables for statistical modeling. Auxiliary covariates included county-specific sociodemographic factors such as county population composition of age, sex, race, educational achievement, county unemployment rate, rural-urban continuum characteristics,
economic dependence indicators, and poverty indicator. Corresponding to the 4 age categories at the individual level, the auxiliary dataset included 4 age variables, which are the percentages of each age group
18 years or older in the county population.
Estimation method
Modified on the basis of the multilevel logistic regression model of Li and colleagues (13), our
2-step small-area estimation method is a combination of hierarchical modeling and synthetic estimation techniques. This mixed model produces a set of fixed-effect parameter estimates, which are general to all counties, and a set of random-effect parameter estimates, which are county-specific values. First, we identified the independent variables
that were significantly associated
with obesity by fitting a generalized linear mixed model with the relevant variables, both individual-level and county-level. We used backward elimination to prune the model. To further improve predictability, we set the selection criterion for retaining a variable or interaction term in the model at α = 0.1 (21). In the final model, fixed effects included the following variables:
age, sex, race, education level, employment status, survey year, and county-level
average per capita annual household income. Random effects included individual-level variables age, sex, race, education level, and survey year. We also
calculated odds ratios for associated socioeconomic factors in this step.
In the second step of the estimation, we applied a synthetic technique to
link the model-generated parameter estimates to the county-specific
characteristics to produce county-level estimates. This way, the strength
borrowed through the model is realized for each county. Because random effects were not significant, we used only the fixed-effect values in the calculation. However, following the recommendation of Binder
(22),
Jiang (23), and Jia et al (24), we kept the random-effects
component in the model to improve estimation for fixed effects and to enhance
the proper selection of variables (Appendix). We conducted all analyses by using SAS version 9.2 (SAS Institute
Inc, Cary, North
Carolina) to account for the complex sampling design. We grouped the county-level obesity prevalence estimates into quartiles to examine geographic patterns. We produced the obesity map by using ArcGIS 9.2 (ESRI, Redlands, California).
We assessed the precision of our estimates by using the width of 95% confidence intervals (CIs). Following the example of another study (25), we examined correlations and mean absolute differences between model estimates and internal
standards: direct estimates of the state-level obesity rate for 2007 through 2009, and direct estimates for age, sex, and race subgroups. The sample sizes for the 4 age subgroups, 2
sex subgroups, and 2 race subgroups were large enough for reliable direct estimation (range, 663-7,305). Taking into consideration the complex sampling design of BRFSS,
we used SAS PROC SURVEYLOGISTIC procedure (SAS Institute,
Inc, Cary, North Carolina) for direct estimations to account for the weight of each respondent.
Back to top
Results
The state obesity prevalence increased significantly, from 32.5% in 2007 to 33.4% in 2008 and 35.4% in 2009. The prevalence estimates of all 82 counties were
higher in 2009 than in 2007 (Tables
1 and 2). In 2009, all counties had prevalence of obesity greater than 30%. In 49 counties, the prevalence of obesity
was at 35% or higher, and in 12 counties, was at least 40% or higher. Compared with the Healthy
People 2010 goal and with the 2009 national average, all of the county estimates
were substantially higher (Figure
1).
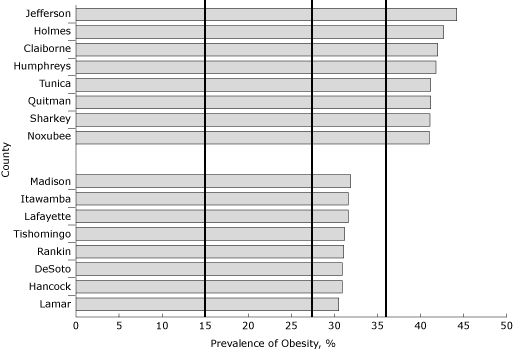
Figure 1. 2009 Mississippi County prevalence of obesity,
Behavioral Risk Factor Surveillance System (BRFSS)
data. Ten percent of the counties with the lowest and highest obesity rates are
shown. The vertical line at 15% indicates the
Healthy People 2010 goal for obesity; vertical lines at 27.1%, and 35.4%
indicate the 2009 national and state averages, respectively. Obesity is defined
as a BMI ≥30.0 kg/m2 based on 2009 BRFSS
self-reported data. [A
tabular version of this figure is also available.]
There was considerable geographic variation in obesity prevalence among Mississippi counties. The difference between Jefferson County (highest) and Lamar County (lowest)
was 13.7% (Figure 2). Counties with higher obesity rates were clustered in the Mississippi Delta region and along the Mississippi River
(Figure 2). Counties along the coastline and in the northeast region (Appalachian foothills) had lower obesity rates,
as did counties with higher socioeconomic
status, such as Madison and Rankin counties.
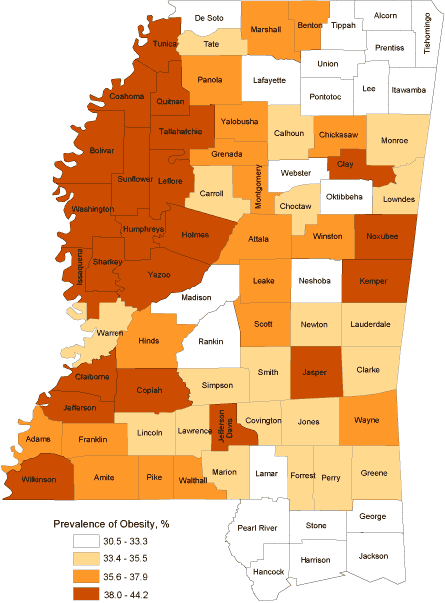
Figure 2. 2009 Mississippi county prevalence of obesity
map
(in quartiles), Behavioral Risk Factor Surveillance System (BRFSS) data. Lighter colors represent lower obesity rate, and
darker colors represent higher obesity rate. Obesity is defined as BMI ≥30.0
kg/m2 based on 2009 BRFSS self-reported data. [A tabular
version of this figure is also available.]
Respondents aged 30 to 44 years had the highest odds of being obese
(Table 3). Compared with college graduates,
respondents
with an education level less than a bachelor’s degree were more likely to be obese. Women had slightly higher odds
than men, and blacks had much higher odds than whites.
The interaction between sex and race was significant (P <.001);
compared with white men, the odds of obesity were 2.2 (95% CI, 2.0-2.5) for black women, 1.4 (95% CI, 1.2-1.6)
for black men, and 0.8 (95% CI, 0.7-0.9) for white women.
Evaluation of county-level estimates
The width of 95% CIs for all county estimates was less than 5 percentage
points (range 2.5-4.7 percentage points). This precision was comparable to that of the design-based direct estimates for the state and is considered reliable (25,26). To assess accuracy, we aggregated small-area county-level estimates to the state level for 2007 through 2009 and compared them with their respective state-level direct estimates; we also compared state-level model estimates with state-level
direct estimates for 2007 through 2009. We further compared model estimates of age, sex, and race subgroups with their respective direct estimates. Pearson’s correlation coefficients between the 2 sets of estimates for the comparisons were 0.95, 0.95, and 0.96, respectively, and the mean absolute differences were 0.5%, 0.5%, and 1.5%, respectively.
Back to top
Discussion
Using 2007-2009 BRFSS data, we obtained stable estimates for county-level prevalence of obesity. The 2009 obesity prevalence in all Mississippi counties is high: it shows the size and scope of the problem facing the state. This finding may help raise the awareness of the obesity crisis for state policy makers, health agency officials, journalists, and the general public. The county estimates also show that obesity prevalence among Mississippi counties
varies considerably, which reveals the heterogeneous nature of the obesity epidemic in the state and requires targeted prevention measures to curb the trend. Furthermore, the
escalating trend observed in Mississippi necessitates aggressive action. Mississippi has taken firm steps in confronting the child obesity crisis (27); parallel measures should be taken for adults.
Similar to observations reported by Li and colleagues (13), we found that in general, socioeconomic status was inversely related to the county prevalence of obesity among adults aged 18 years or older in Mississippi, after adjusting for age, sex, and race. This information may be helpful in guiding the direction of obesity prevention campaigns.
Confirming the troubling racial and socioeconomic disparities in obesity rates observed in other studies (2,3,28), our study shows that the
risk of obesity for blacks nearly doubled that of whites, and black women had the highest odds
of obesity. The 2000 Census indicates that Mississippi’s population consists of 33.7% blacks, the highest in the nation (19). This means that compared with the rest of the nation, a larger
proportion of Mississippi’s population is in a higher risk category. Therefore, racial disparity in obesity
affects Mississippi more than other states. The racial disparity, along with socioeconomic disparities, may
influence public health efforts to plan and implement tailored prevention policies and programs
because the effectiveness of health-promoting strategies varies among racial and
socioeconomic groups. For instance, walking trails may be more effective in a
community where a certain ethnic group clusters, and a farmer’s market may be more
effective in another community of different racial combinations. Consequently,
prevention polices and programs would be most effective if designed accordingly.
This study has potential biases and limitations. First, because the weight and height values in BRFSS were self-reported, bias may have occurred (29,30). Compared with other surveys that generate estimates of obesity prevalence (eg, the National Health and Nutrition Examination Survey,
for which trained professionals measure the height and weight of participants), BRFSS
data tend to underestimate obesity prevalence. Some similar studies, attempting to minimize self-reporting bias, developed a correction method by using auxiliary data (13). However, since self-reporting bias affects all the county-level estimates similarly, it is not expected that relative distribution of obesity would vary. When estimates are biased, concerns arise
about the magnitude of the bias. In the absence of an external standard against which to compare
our data, our assessment of accuracy in this study is limited. Second, because
of software limitations in handling standard error estimation when using mixed models for complex sample survey data, the 95% CI produced was a reasonable approximation, not exact. Further investigation in this direction may be needed.
Back to top
Acknowledgments
We thank Ron McAnally and Dick Johnson of the Mississippi State Department of Health for providing Mississippi BRFSS data.
We also thank Nimish Valvi of the Mississippi State Department of Health for mapping the county obesity rates.
Back to top
Author Information
Corresponding Author: Zhen Zhang, PhD, Center of Biostatistics and
Bioinformatics, University of Mississippi Medical Center, 2500 N State St, Jackson, MS 39216. Telephone: 601-715-2125. E-mail:
zqin2@umc.edu.
Author Affiliations: Lei Zhang, Mississippi State Department of Health, Jackson, Mississippi; Alan Penman, Warren May, University of Mississippi Medical Center, Jackson, Mississippi.
Back to top
References
- Mokdad AH, Serdula MK, Dietz WH, Bowman BA, Marks JS, Koplan JP.
The spread of the obesity epidemic in the United States, 1991-1998. JAMA 1999;282(16):1519-22.
- Ogden CL, Carroll MD, Curtin LR, McDowell MA, Tabak CJ, Flegal KM.
Prevalence of overweight and obesity in the United States, 1999-2004. JAMA 2006;295(13):1549-55.
- Wang Y, Beydoun MA.
The obesity epidemic in the United States — gender, age, socio-economic, racial/ethnic, and geographic characteristics: a systematic review and meta-regression analysis. Epidemiol Rev 2007;29:6-28.
- Flegal KM, Carroll MD, Ogden CL, Curtin LR.
Prevalence and trends in obesity among US adults, 1999-2008. JAMA 2010;303(3):235-41.
- Behavioral Risk Factor Surveillance System prevalence and trends. Centers for Disease Control and Prevention. http://apps.nccd.cdc.gov/brfss. Accessed November 1, 2009.
- US Department of Health and Human Services, Office of the Surgeon General. The Surgeon General’s call to action to prevent and decrease overweight and obesity. http://www.surgeongeneral.gov/topics/obesity/. Accessed July 10, 2009.
- Flegal KM, Graubard BI, Williamson DF, Gail MH.
Excess deaths associated with underweight, overweight, and obesity. JAMA 2005;293(15):1861-7.
- Finkelstein EA, Fiebelkorn IC, Wang G.
National medical spending attributable to overweight and obesity: how much, and who’s paying? Health Aff
(Millwood) 2003;w3-219-26.
- Mississippi State Department of Health. FY 2009 Mississippi state health plan. http://www.healthyms.com/msdhsite/_static/resources/2945.pdf. Accessed August 3, 2009.
- Centers for Disease Control and Prevention.
Estimated county-level prevalence of diabetes and obesity — United States, 2007.
MMWR Morb Mortal Wkly Rep 2009;58(45):1259-63.
- Yancey AK, Kumanyika SK, Ponce NA, McCarthy WJ, Fielding JE, Leslie JP, et
al. Population-based interventions engaging communities of color in healthy eating and active living: a review. Prev Chronic Dis 2004;1(1).
http://www.cdc.gov/pcd/issues/2004/jan/03_0012.htm.
Accessed April 1, 2011.
- Economos CD, Irish-Hauser S.
Community interventions: a brief overview and their applications to the obesity epidemic. J Law Med Ethics 2007;35(1):131-7.
- Li W, Kelsey JL, Zhang Z, Lemon SC, Mezgebu S, Boddie-Willis C, et al.
Small-area estimation and prioritizing communities for obesity control in Massachusetts. Am J Public Health 2009;99(3):511-9.
- Balluz L, Ahluwalia IB, Murphy W, Mokdad A, Giles W, Harris VB.
Surveillance for certain health behaviors among selected local areas — United States, Behavioral Risk Factor Surveillance System,
2002. MMWR Surveill Summ 2004;53(5):1-100.
- Schumann CL, Remington PL.
Using local data to monitor obesity rates in Wisconsin counties, 1994-2003.
WMJ 2005;104(5):20-5.
- Rao JNK. Small area estimation. New York (NY): Wiley-Interscience; 2003.
- Malec D, Sedransk J, Moriarity CL, Leclere FB. Small-area inference for binary variables in the national health interview survey. Journal of American Statistical Association 1997;92(439):815-26.
- Moura FAS, Migon HS. Bayesian spatial models for small-area estimation of proportions. Statistical Modeling 2002;2(3):183-201.
- US Census Bureau, Census 2000 gateway. http://www.census.gov/census2000/sumfile3.html. Accessed October 12, 2009.
- Measuring rurality: 2004 county typology codes. US Department of Agriculture Economic Research Service. http://www.ers.usda.gov/briefing/rurality/typology/. Accessed September 8, 2009.
- Knutson K, Zhang W, Tabnak F. Applying the small-area estimation method to estimate a population eligible for breast cancer detection services. Prev Chronic Dis 2008;5(1).
http://www.cdc.gov/pcd/issues/2008/jan/06_0144.htm.
Accessed September 9, 2009.
- Binder DA. On the variances of asymptotically normal estimators from complex surveys. Int Stat Rev 1983;51(3):279-92.
- Jiang J. Consistent estimates in generalized linear mixed models. Journal of American Statistical Association 1998;93:720-9.
- Jia H, Muennig P, Borawski E.
Comparison of small-area analysis techniques for estimating county-level outcomes. Am J Prev Med 2004;26(5):453-60.
- Schneider KL, Lapane KL, Clark MA, Rakowski W. Using small-area estimation to describe county-level disparities in mammography. Prev Chronic Dis
2009;6(4).
http://www.cdc.gov/pcd/issues/2009/oct/08_0210.htm.
Accessed April 8, 2010.
- Mississippi Behavioral Risk Factor Surveillance System. Mississippi State
Department of Health. http://www.msdh.state.ms.us/brfss/overview.htm. Accessed June 2, 2009.
- Evaluating the impact of the Mississippi Healthy Students Act on childhood
obesity. Mississippi State Department of Health. http://www.mshealthpolicy.com/documents/RWJF64636ProjectBriefNov08.pdf. Accessed June 6, 2010.
- Wang Y, Zhang Q.
Are American children and adolescents of low socio-economic status at increased risk of obesity? Changes in the association between overweight and family income between 1971 and 2002. Am J Clin Nutr 2006;84(4):707-16.
- Villanueva EV.
The validity of self-reported weight in US adults: a population based cross-sectional study. BMC Public Health 2001;1:11.
- Nyholm M, Gullberg B, Merlo J, Lundqvist-Persson C, Råstam L, Lindblad U.
The validity of obesity based on self-reported weight and height: implications for population studies. Obesity 2007;15(1):197-208.
Back to top
