 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Poison Control Center--Based Syndromic Surveillance for Foodborne IllnessMary P. Derby,1 J.
McNally,1 J. Ranger-Moore,1 L.
Hulette,2 R. Villar,1 T. Hysong,1 E. MacNeill,2 M. Lebowitz,1 J. Burgess1
Corresponding author: Mary P. Derby, Environmental and Community Health, Mel and Enid Zuckerman College of Public Health, The University of Arizona, 1435 North Fremont, Tucson, AZ 85719. Telephone: 520-620-6936; Fax: 520-882-5014; Email: mpderby@email.arizona.edu. Disclosure of relationship: The contributors of this report have disclosed that they have no financial interest, relationship, affiliation, or other association with any organization that might represent a conflict of interest. In addition, this report does not contain any discussion of unlabeled use of commercial products or products for investigational use. AbstractObjectives: This retrospective study evaluated the usefulness of a poison control center (PCC) data collection system in Tucson, Arizona for early detection of foodborne disease outbreaks. Methods: A search of a PCC database identified callers with gastrointestinal symptoms attributable to suspected foodborne illnesses whose calls were received during January 1--March 31, 2000. For each foodborne illness-related call, PCC coding was compared with a predefined diarrhea/gastroenteritis syndrome. PCC calls also were evaluated by using ZIP code, age, sex, and date of symptom onset to determine if call classifications matched any laboratory-confirmed cases reported to a county health department. Results: An independent review generally agreed with the PCC's classification of calls. When calls and cases were compared, only one potential match was identified. Conclusion: Although confirmatory diagnostic information was not available, PCC calls were not duplicative of cases evaluated by the county health department, which suggests that they represent two independent data sets. PCC data might provide a useful addition to surveillance data reported to public health agencies for the early detection of foodborne disease outbreaks. These results will now be used to develop collaborative prospective surveillance systems. IntroductionIncreased concern for public safety and the risk of emerging infectious diseases has prompted interest in the development and implementation of syndromic surveillance systems. The aim of these systems is to enhance traditional public health surveillance systems by collecting and analyzing realtime (i.e., instantaneous) or near real-time data on symptoms from nontraditional sources (e.g., pharmaceutical sales or school absentee records) before laboratory confirmation of an illness is received (1--3). By focusing on trends or unexpected patterns in data, syndromic surveillance systems might assist public health authorities in detecting outbreaks more rapidly than can be performed by using traditional public health surveillance systems (4,5). Public health departments are using syndromic surveillance systems to monitor diarrheal disease or influenza-like symptoms (through pharmaceutical sales data) (6,7) and influenza-like illness (through emergency medical services dispatch records) (8) and to detect outbreaks of illnesses that might be infectious or related to a biologic terror attack (through data on emergency department [ED] and urgent care visits) (9,10). Public health departments are responsible for detecting, managing, and preventing foodborne disease outbreaks (FBDOs). Foodborne diseases account annually for an estimated 76 million illnesses, 325,000 hospitalizations, and 5,000 deaths in the United States (11,12). Traditional public health FBDO surveillance systems collect data when ill persons seek medical care. However, only an estimated 8% of persons with gastroenteritis symptoms seek medical care, and only a minority of those who do seek care undergo diagnostic testing necessary to determine an etiology for their illness (13,14). In addition, substantial delays can occur while awaiting laboratory results. Because PCCs operate 24 hours a day, collect real-time symptom data from callers who seek treatment advice, and provide referral assistance before callers seek medical care, forming partnerships with PCCs might enhance public health surveillance systems. A recent Institute of Medicine report underscored the need to integrate PCC networks with the public health system to improve surveillance systems (15). Investigation of foodborne illnesses in Pima County (2000 population: 843,746), Arizona, is primarily the responsibility of the Pima County Health Department (PCHD), which operates a traditional public health FBDO surveillance system. All suspected and laboratory-confirmed cases of foodborne illnesses reported to PCHD by health-care providers and all restaurant complaint calls received by PCHD are investigated. The Arizona Poison and Drug Information Center (APDIC) provides case-specific treatment and referral information to callers who complain of foodborne illness. APDIC evaluates complaints received independently of PCHD. The goals of this study were to evaluate the ability of APDIC's data collection system to provide early detection of FBDOs and to recommend ways to improve FBDO surveillance efforts by integrating the two surveillance systems. MethodsPCC Data CollectionAPDIC is one of two PCCs operating in Arizona, serving approximately 2 million persons statewide (excluding residents of Maricopa County, who call the Banner PCC). Staffed by trained pharmacists and certified by the American Association of Poison Control Centers, APDIC receives 180--250 calls daily. In 2000, of 68,433 calls received, approximately 31,000 involved exposures, of which 783 (2.5%) involved suspected foodborne illness or an illness related to food ingestion. An additional 38,433 information (nonexposure) calls were received, of which 202 (0.5%) were related to questions about foodborne illness or food products. When a call is received, a PCC specialist records the caller's suspected exposure (e.g., food poisoning) and provides consultation on the basis of the caller's suspected exposure, age, underlying medical history, and acuity and duration of reported symptoms. The PCC specialist also enters call data, including an assessment (i.e., exposure reason), into an electronic database (Toxicall,® Computer Automation Systems, Inc., Aurora, Colorado). For all exposure-related calls, the PCC specialist enters the date and time the call was received; the caller's sex, age, and ZIP code; type of call (exposure or information); acuity of symptoms; reason for exposure (as assessed by the PCC specialist); exposure site, time, and route; clinical effects, therapies, and medical outcome; and any multiple contacts. Because a caller might report more than one ill person within a household, the PCC specialist also assigns a case-record number and completes a medical history and disposition for each contact identified. To identify multiple contacts, the PCC specialist cross-references all case-record numbers in each caller's and contact's case record. If the call is anticipated to require PCC follow-up, the caller's name and telephone number are also recorded. The PCC specialist may elect to record additional call information in the narrative section of the database. To ensure quality control, every tenth record received daily is reviewed for accuracy of data entry. Call Confirmation and Comparison to Syndrome DefinitionAll calls to APDIC concerning human exposure received during January 1--March 31, 2000, were reviewed retrospectively. Three factors were considered in constructing the syndrome definition: 1) APDIC lacks a uniform process for coding suspected foodborne illnesses; 2) the PCC specialist codes calls according to how callers report exposure history (i.e., chief complaint); and 3) multiple syndromic definitions exist for diarrhea/gastroenteritis. The syndrome definition used was modified from that used by the Arizona Department of Health Services for drop-in syndromic surveillance conducted during the 2001 World Series in Arizona (i.e., vomiting, abdominal pain, or any other gastrointestinal [GI] distress) (16). Foodborne illness was defined broadly as a syndrome or associated symptoms recognized by a caller who reported ingestion of suspected contaminated food and any of the following GI complaints: abdominal pain, nausea, vomiting, or diarrhea. The selected syndrome definition used in this study included symptoms associated with, but not limited to, foodborne illnesses. Callers with GI symptoms associated with an underlying medical condition (e.g., irritable bowel syndrome, reaction to medication, or chemical exposure not related to ingestion of contaminated food) were excluded. A nurse reviewed call data records from APDIC's electronic database by following a protocol that identified all possible calls with suspected foodborne illness, reviewed each identified caller's record, and abstracted preselected variables from each record. Within the protocol used, the search process (Figure) involved a review of all Pima County calls by a nurse to determine if coding of calls by PCC specialists conformed to the syndrome definition. Standardized variables were collected and entered into a database for analysis. Information collected included each caller's age, sex, and ZIP code; symptoms; presumed exposure history; exposure site, time, and route; multiple contact(s); referral recommendation(s); and APDIC coding of the caller's suspected diagnosis. Sensitivity, specificity, and positive predictive value (PPV) were calculated on the basis of APDIC coding of callers' suspected foodborne illness compared with the nurse reviewer's assessment of APDIC call data, using the syndrome definition. Call Confirmation and Comparison to Laboratory-Confirmed CasesPCHD provided data on cases of laboratory-confirmed illnesses during January 1--March 31, 2000. Variables collected on laboratory-confirmed illnesses included the caller's sex, age, and ZIP code; the date a laboratory confirmed the results; the date of onset of symptoms; and the date PCHD was notified of the confirmed report. To determine whether APDIC foodborne illness complaint calls also were reported to and evaluated by PCHD, an attempt was made to match calls to PCHD laboratory-confirmed cases by using date of onset of symptoms, ZIP code, age, and sex. Onset of symptoms was considered a critical variable because it most likely represented the date a person would have called APDIC. However, for 49% of PCHD cases, the onset of symptoms date was unavailable. The unavailability rate varied (range: 25%--62%) for each microorganism identified through laboratory confirmation (Table 1). For those laboratoryconfirmed PCHD cases for which the date of the patient's onset of symptoms was unavailable, an onset date was estimated for each type of foodborne illness (i.e., campylobacter, giardiasis, hepatitis A, shigellosis, and salmonellosis) by using the average interval from date of onset of symptoms to the laboratory-confirmed date for cases for which the patient's symptom onset date was known. The average interval, ±3 days, was used to look for matches to APDIC calls by ZIP code, age, and sex. Differences in age, sex, and incubation period were evaluated by using chi-square analyses. Data were analyzed by using SPSS (Chicago, Illinois) and Stata 8.0 (College Station, Texas). The study analysis focused on Pima County callers to APDIC and laboratory-confirmed PCHD cases. This study was conducted in accordance with the Health Insurance Portability and Accountability Act, which requires that a minimum of identifiable data be used to ensure patient privacy, and data that would identify callers and cases were not collected. This study underwent human subjects review and was approved by The University of Arizona Institutional Review Board. ResultsAPDIC Call DescriptionDuring January 1--March 31, 2000, APDIC received 6,768 calls reporting human exposure; 2,922 (43.2%) were from Pima County residents. The database search process and outcome were limited to Pima County callers (Figure). Of 370 calls reporting human exposure with recorded GI symptoms, 307 (83%) were ingestion related; 51 (14%) calls were recorded as unintentional food poisoning, of which 50 were consistent with the syndrome definition. Twenty-nine (58%) persons whose reported symptoms were consistent with the syndrome definition called APDIC <24 hours of suspected reported exposure, and seven (14%) persons called >24 hours after suspected reported exposure. For 14 (28%) callers, exposure history was undetermined. Sixteen (32%) callers reported an exposure outside the home, and 19 (38%) involved more than one person. Only two (4%) callers were referred to a health-care facility or ED for immediate medical evaluation. Adults accounted for the highest number of symptomatic calls, with 18 (36%) known to be aged >25--64 years. Six (12%) calls were received from adults reporting illness among persons aged 15--24 years, six (12%) reporting illness among children aged 5-14 years, and three (6%) reporting illness among children aged <5 years (Table 2). Sensitivity, Specificity, and PPVSensitivity, specificity, and PPV were calculated for APDIC's coding of each call, and compared with the nurse reviewer's assessment of the call data (Table 3). Of the 256 calls involving GI symptoms and ingestion but coded by APDIC as nonfood-related, eight (3%) likely represented potential cases of foodborne illness. Including these eight calls, sensitivity of the search strategy and APDIC coding for foodborne illness was 86% (50/58). Only one false-positive call was identified, which yielded a specificity of 99.6% (248/249). The symptoms and exposure reported from this caller were more consistent with a probable food allergy. Of 51 calls identified by the search strategy, 50 (98%) were consistent with the syndrome definition, providing a PPV of 98% (50/51). APDIC Calls Compared to PCHD-Confirmed CasesA total of 77 laboratory-confirmed cases were reported to PCHD. Only one of the APDIC calls was a potential match to a confirmed PCHD case. For this potential match, both the APDIC call and PCHD case had the same date of symptom onset, date of call, ZIP code, and sex; however, the caller's age was different by 1 year. No significant differences in age or sex were noted between callers and cases in the APDIC and PCHD databases. However, the incubation period for the 77 laboratory-confirmed cases (>2 days for 47 [61%] and <24 hours for 30 [39%] cases) was statistically different (p<0.001) from the incubation period for the APDIC calls (<24 hours for 29 [58%] calls). DiscussionPCCs provide a new source of real-time data that might help improve surveillance for FBDOs, which are characterized by illness attributable to a common food or water source among two or more persons (12). During the 3-month study period, APDIC received 51 calls regarding foodborne illness, of which 50 were consistent with the diarrhea/gastroenteritis syndrome definition used. Although the majority of calls represented single occurrences of illness, 19 (38%) calls involved more than one person and thus might have been representative of outbreaks. Only one potential match was identified as a PCHD laboratory-confirmed illness, indicating that the APDIC data collection system is not duplicative of cases reported to and evaluated by PCHD during the same period. Although clinical validation studies are needed to determine the exact etiology of these illnesses, APDIC might help PCHD identify FBDOs earlier through detection of new cases of foodborne illness. Although APDIC has multiple coding categories that PCC specialists can use to code suspected cases of foodborne illnesses, the defined search strategy identified calls regarding potential foodborne illness reported to and classified by APDIC with high specificity and reasonable sensitivity. If only callers with GI symptoms and a history of ingestion were considered, a high degree of agreement existed between the syndrome definition and coding by the PCC specialist for those calls classified as unintentional food poisoning. The entire database was searched for GI symptoms and ingestion, and all cases of potential foodborne illness were reviewed, thus ensuring that all cases of misclassification were identified. Because PCCs report data regarding symptoms, not diagnoses, the syndrome definition used to evaluate calls for foodborne illness was critical. Studies have not compared the accuracy of callers' chief complaints compared with that of PCC specialists' assessment for foodborne illness. However, a recent study that evaluated the accuracy of using ED patients' chief complaints classified ED visits into syndromes and identified agreement for GI syndrome (17). Other research on ED visits has determined that International Classification of Diseases (ICD) codes are more accurate than a patient's chief complaint, possibly because they are based on a physician's diagnosis (18). In constructing the GI syndrome definition, consideration was given to multiple definitions discussed in the literature. The syndrome definition used was consistent with that used by ADHS for drop-in surveillance; however, other definitions have been used (9). A limitation of the syndrome definition used is that it included symptoms associated with, but not limited to, foodborne illness. For outbreak detection to be improved, a standard syndrome-based definition should be developed for APDIC to collect and code call data consistent with an established syndrome-based definition. ConclusionComparing the incubation period noted for the majority of APDIC callers (<24 hours) with that for persons whose cases were identified by PCHD suggests that the two data sets are identifying persons from different populations. Preformed toxins are typically associated with gastroenteritis after a short incubation period (usually 2--4 hours) (19). Chemical contaminants also produce similar symptoms <30 minutes after ingestion (12). In contrast, bacterial pathogens, including Shigella and Salmonella, might be associated with longer incubation periods (range: 12--36 hours for Salmonella and 12--96 hours for Shigella) (19). Another possibility is that callers inaccurately identified their previous meal as the source of their illness. Because the etiologic source of the callers' reported illnesses could not be validated, this matter remains unresolved, underscoring the necessity for external validation of sources. This study is subject to multiple limitations. Demographic and clinical data are missing from both the APDIC and PCHD databases. Not all suspected exposures could be confirmed through laboratory testing, and the study period was brief. Symptom onset dates were not available for 49% of PCHD laboratory-confirmed cases. In an attempt to compensate, onset dates were calculated on the basis of the average interval from the date of symptom onset to the laboratory confirmation date. This was done separately by type of PCHD case (e.g., campylobacter and hepatitis A). One reason why APDIC calls could not be matched to PCHD cases might be that natural variation was lost because of use of a group mean, underscoring the need for more complete data in future studies. Consistent with other foodborne surveillance studies, the illness reported might have been acquired not through what the caller identified as previously consumed contaminated food but instead through an earlier contaminated food source, contaminated water, person-to-person contact, or direct contact with animals (20). Despite these limitations, this study demonstrates a potential role for PCC foodborne illness call data and public health agencies' foodborne illness surveillance systems. The two systems detect GI syndromes and could potentially overlap if both the PCC and the public health department used a well-designed, specific syndromic screen and maintained data regarding the frequency and severity of foodborne illnesses (i.e., for detection of FBDOs). PCCs provide 24-hour coverage with trained PCC specialists who might enhance health department surveillance, particularly during the evenings and on weekends. However, successful integration of these systems requires external clinical validation of PCC foodborne illness calls. On the basis of this analysis, prospective surveillance of APDIC's real-time foodborne illness complaint calls will be implemented. Callers to APDIC whose illnesses are consistent with the syndrome definition and who pose the highest transmission risk (e.g., food handlers, child-care providers or attendees, and callers with an increase in severity of symptoms) will, upon informed consent, be referred to PCHD for evaluation of their symptoms. Similarly, an independent nurse reviewer will conduct follow-up regarding consenting callers whose symptoms are consistent with the syndrome definition but who are not referred to PCHD to determine the extent of their illness and any medical treatment received. This prospective surveillance will allow for a clinical validation of callers' illnesses by determining sensitivity, specificity, and PPV by using a laboratory test as a standard on those calls referred to PCHD. Additional studies are needed to assess the effectiveness of a prospective, integrated approach to foodborne illness surveillance. Fundamental to success of these efforts is public awareness of what types of illnesses should be reported and where they should be reported, the development of standardized definitions of syndromic illnesses, and consistent coding of calls by PCC specialists. Studies are needed to determine whether a temporal relationship exists between APDIC calls and PCHD cases; if such a relation is demonstrated, prospective monitoring of increases in APDIC calls might be predictive of increases in the number of foodborne illness cases. PCCs might improve public health syndromic surveillance for foodborne illnesses because they capture early, real-time symptom data from the broadest possible range of sources (i.e., callers with mild to severe illness). Once clinical evaluation has confirmed callers' foodborne illnesses, then computerized PCC databases could be linked and programmed with detection algorithms to alert public health officials of increases in cases or geographic clustering of cases. The PCHD surveillance system is limited in its ability to capture real-time foodborne illness symptom data. APDIC might provide a useful addition to the PCHD's syndromic surveillance system and might assist in early detection of FBDOs. AcknowledgmentThis research was supported in part through a National Institute of Health Predoctoral Training Fellowship, NIH grant number 5F31NR00824-03. References
Table 1  Return to top. Table 2 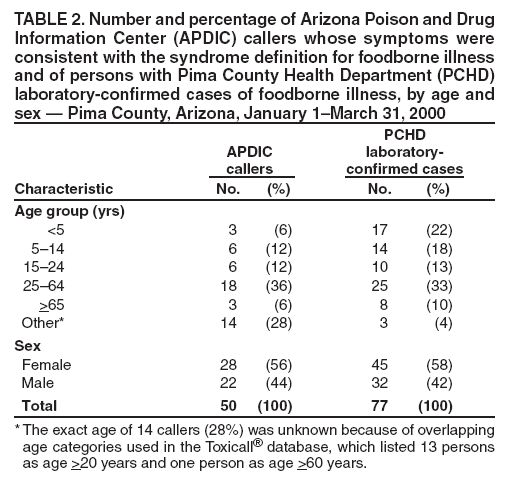 Return to top. Table 3 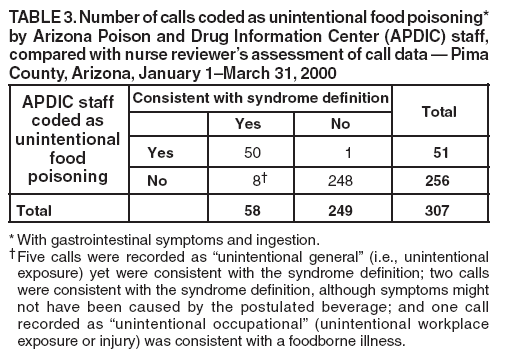 Return to top. Figure 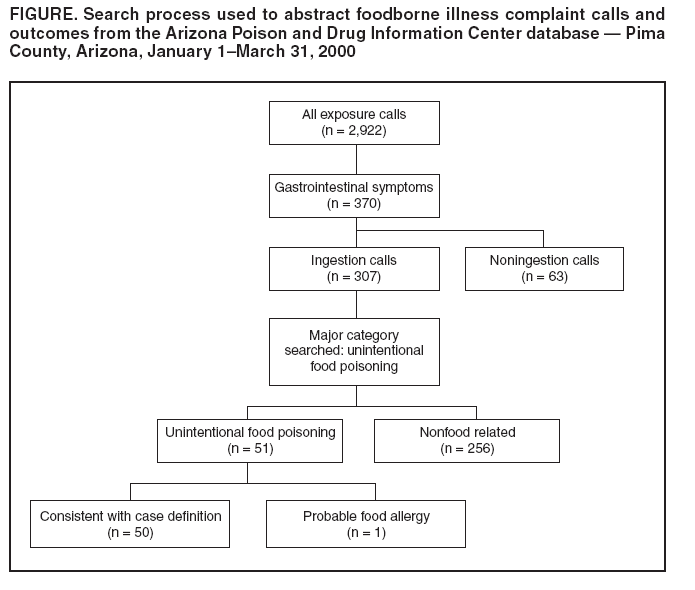 Return to top.
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Date last reviewed: 8/5/2005 |
|||||||||
|