 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Emergency Department Visits for Concern Regarding Anthrax --- New Jersey, 2001Paul C. Allegra,1 D.
Cochrane,1,2 E. Dunn,1 P. Milano,1 J.
Rothman,2 J. Allegra1,2
Corresponding author: Dennis George Cochrane, 241 Brook Valley Rd., Kinnelon, NJ 07405. Telephone: 973-331-0069; Fax: 973-331-0228; E-mail: cochraned@verizon.net. Disclosure of relationship: The contributors of this report have disclosed that they have no financial interest, relationship, affiliation, or other association with any organization that might represent a conflict of interest. In addition, this report does not contain any discussion of unlabeled use of commercial products or products for investigational use. AbstractIntroduction: In October of 2001, after letters processed in Trenton, New Jersey, resulted in multiple cases of anthrax, emergency departments (EDs) in New Jersey experienced an increase in visits from patients concerned about possible exposure to agents of biologic terrorism. Information about the effect of an actual biologic terrorism attack on the emergency department population might be useful in the design of biosurveillance systems, particularly with regard to their performance during the mitigation phase that occurs after an attack. In addition, such information might help identify issues that arise regarding the public health response in the ED setting. Objectives: The objectives of this report were to identify and characterize ED visits, by patients concerned with exposure to biologic terrorism agents, in selected New Jersey hospitals after the anthrax attack in fall 2001. Methods: A retrospective cohort design was used in this study. The setting was 15 New Jersey EDs within a 55mile radius of Trenton. Participants were consecutive patients evaluated by ED physicians for the following four periods in 2001: 1 month before September 11; 1 month after September 11; 1 month after October 11; and for the second month after October 11. Percentages of visits were calculated with a concern for exposure (CE) visits by using International Classification of Diseases, Ninth Revision (ICD-9) descriptors: Feared Complaint--No Diagnosis (ICD-9 code v65.6) and Screening for Infectious Disease (ICD-9 code v75.9) for all hospitals and for Trenton versus nonTrenton hospitals as a percentage of ED visits. Charts were reviewed by using a structured data form. Results: A total of 225,403 ED visits occurred during the 4 months, of which 698 were CE visits. The percentages of CE visits for the four periods were 0.06%, 0.06%, 0.92%, and 0.10%, respectively. For the peak third period, the percentage was increased for the two Trenton hospitals, 1.81%, versus 0.82% for the 13 non-Trenton hospitals. This report is a summary of the 508 visits associated with concern for anthrax exposure during the peak third period: 47% reported exposure to powder, 13% were postal workers, 4% received chest radiographs, 65% had a nasal swab for anthrax, 13% had ED decontamination, and 32% received antibiotics. Conclusion: An increase in CE visits occurred during the 1-month period after October 11, 2001. During the peak month, a higher increase occurred in Trenton EDs. Considering the substantial variation in diagnostic evaluation and treatment, readily available guidelines are needed. IntroductionMedia coverage after the September 11, 2001, attacks included warnings regarding possible biologic terrorism. On October 4, 2001, less than 1 month after the terrorist attacks on the World Trade Center and Pentagon, the condition of a man in Florida was diagnosed as respiratory anthrax; he had no known exposure risk factors (1). On October 12, a case of cutaneous anthrax was reported in New York City. At NBC News, a person was exposed to a letter containing a suspicious powder. The Federal Bureau of Investigation (FBI) reported that four recovered envelopes containing Bacillus anthracis spores were postmarked at the U.S. Postal Service Trenton Processing and Distribution Center in Hamilton Township, New Jersey. The investigation revealed that the Hamilton Township Postal Facility handled two envelopes containing B. anthracis that were mailed to news organizations in NYC on September 18, 2001, and two envelopes mailed to U.S. Senate offices in Washington, DC, on October 9, 2001. Concerns increased in New Jersey on October 18, when two postal workers from the Trenton facility were confirmed to have cutaneous anthrax. These exposures were presumed to represent contact with letters or cross-contamination from letters containing B. anthracis mailed from this location. A total of 22 confirmed or suspect cases of anthrax infection occurred; 11 were inhalation cases, and 11 were cutaneous cases. Five persons died (2). Multiple patients sought medical treatment at New Jersey emergency departments (EDs) with concerns of possible exposure (CE visits) after the media reports of October 12, 2001. Records of these visits, including physician notes, were documented in an electronic format. Syndromic surveillance techniques have been previously reported by using a large existing computerized database of ED visits (3). Techniques included using International Classification of Diseases, Ninth Revision (ICD-9) groups to identify a subgroup of patient visits, examining time-series volume data for these groups, and using electronic chart reviews, to examine characteristics of the subpopulation identified. Limited information has been written regarding the use of such techniques in the aftermath (mitigation phase) of an actual biologic terrorist attack. The objectives of this report were 1) to use these techniques to determine the temporal and geographic aspects of CE visits at 15 New Jersey EDs during the period surrounding the anthrax attacks of 2001 and 2) to characterize the clinical presentations, diagnostic evaluations, and treatments provided, based on a chart review of the electronic medical record. MethodsA retrospective analysis of a computerized database was performed of ED visits from one emergency physician group staffing 15 New Jersey EDs within a 55-mile radius of Trenton. The annual ED volume was 20,000--65,000 patients. These hospitals included urban and suburban teaching and nonteaching hospitals and two hospitals in Trenton. These hospitals comprise approximately 30% of all northern New Jersey hospitals and receive an estimated 35%-40% of all ED visits in northern New Jersey. Consecutive patients evaluated by ED physicians August 11--December 11, 2001, were included. The ED physicians evaluate 85%--95% of the patients at these EDs. Private physicians evaluate the remainder of the patients. The physicians' billing department coded the physicians' charts according to the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) codes. All coders were located at one central facility and trained and supervised similarly. Patients were included as concern for exposure (CE) visits if the primary ICD diagnosis included the following ICD-9 descriptors: Feared Complaint--No Diagnosis (ICD code v65.6) and Screening for Infectious Disease (ICD-9 code v75.9). Percentages of CE visits were calculated for all hospitals and for Trenton versus nonTrenton hospitals as a percentage of ED visits. The following four periods in 2001 were used in the calculation: 1 month before September 11; 1 month after September 1, 1 month after October 12; and the second month after October 12. These periods were chosen to offer sufficient time to establish a baseline percentage before September 11 and to include a similar period after the anthrax cases decreased to the baseline percentage. The student t test and the Chi-square were used to test for statistical significance with alpha set at 0.05. The Bonferroni correction was used when multiple comparisons were made. A chart review was conducted by using a structured data form. The details were provided of the chart review for the peak third period for those visitors who had a concern for anthrax. The details characterized the mechanisms of exposure, symptoms, diagnostics, and treatments. The Internal Review Board at Morristown Memorial Hospital Residency in Emergency Medicine, Morristown, New Jersey, approved the study. ResultsFor the four periods, 225,403 ED visits occurred, of which 698 (0.3%) were CE visits. The percentage of CE visits versus time has been illustrated (Figure 1). A sharp increase occurred on October 12, and a decrease occurred near the baseline 1 month later. The increase on October 12, coincides with the first media news reports of an anthrax case in NYC. Of the 698 CE visits for the four monthly periods, 561 (80%) occurred during the 1-month period after October 12. The percentages of CE visits for the four periods, compared with total visits were 0.06%, 0.06%, 0.92%, and 0.10%, respectively. When the first period is used as the baseline, only the third period indicated a statistically significant increased percentage of CE visits (0.92%; p<0.001). For the peak third period, the percentage was significantly increased for the two Trenton hospitals, compared with the 13 non-Trenton hospitals (1.81% versus 0.82%; p<0.001). Periods 1 and 2 represent periods before the anthrax attacks occurred and therefore indicate baseline characteristics for the patients seeking medical treatment for CE. The chart review in Periods 1 and 2 indicated that the majority of the visits (89%) involved concern regarding one of the following five categories: 1) fear of foreign bodies without findings; 2) motor-vehicle accidents; 3) falls without injury; 4) concern for sexually transmitted disease; and 5) possible toxic ingestion/exposure with none identified. The first casepatient who sought medical treatment for CE to anthrax occurred on October 9. Of the 57,981 ED visits during the third peak period, 561 visits were identified for CE by the ICD9 codes (CE visits), of which 508 were related to a concern for anthrax (CA) visit. The details of the chart review for the peak third period are summarized (Tables 1--4). These results summarize the 508 patient visits that were related to a concern for anthrax. Demographic information is reported for the CA visits during the peak period, October 12-November 11, 2004 (Table 1). Females comprised 277 (55%) of the 508 CA visits during this period. The mean age in years was 39 ± 16. Employees of the post office accounted for 64 patients, and 32 were hospital employees. Based on information charted by the ED physician, 19% of all patients sought help before going to the ED. Seeking help included contacting their primary physician, police department, FBI, postmaster, or job supervisor. A total of 6% reported their concern to the department of public health. In addition, 17% received assistance before going to ED, which included receiving an antibiotic prescription from their primary physician, having their suspected material sent for analysis, and being decontaminated. The mechanisms of exposure for the CA patients during the peak period are presented (Table 2). Of the 508 cases, 120 had documentation of working in or visiting a post office. A total of 128 (25%) patients did not have a history suspicious for exposure to anthrax or the exposure status was not reported. These visits primarily consisted of complaints of fever, cough, chest pain, rash, insect bites, and myalgias. An additional primary complaint was from persons who worked near or traveled by a possible anthrax site and wanted to be checked for anthrax. Examples of other documentation include 1) a hospital employee who was sent by corporate health but did not think she was exposed, and 2) a person who opened several letters from Iraq over the previous year. Respiratory symptoms were present in 70 (14%) patients, and skin symptoms were present in 52 (10%) patients. GI symptoms were present in eight (2%) case-patients. Chest radiographs were done in 20 (4%) of the CA visits, and nasal swab for anthrax was performed during 330 (65%) CA visits. The percentage of visits where nasal swabs were performed was similar until November 3 when a noticeable decline to 22% occurred for the rest of Period 3 (Figure 2). ED decontamination of the patient occurred during 56 CA visits (13%). Antibiotic treatment was initiated for 161 (32%) CA visits. Of these 161 visits, 114 (71%) received ciprofloxacin, and 35 (22%) received doxycycline. Of the 161 patients who received an antibiotic, only 30 (19%) received a prescription for an antibiotic course >14 days. Although determining whether all calls were documented is difficult, calls made to health or police departments were made by the ED and documented for 90 (18%) of the visits. DiscussionA marked increase in CE visits occurred after anthrax was identified in New York City and New Jersey. The CE visits returned to the baseline after 1 month. Despite initial warnings from the media immediately after September 11, 2001, a substantial increase did not occur in CE visits until the initial anthrax case in New York City and the attendant media coverage starting October 12. The number of visits increased substantially in the immediate vicinity of the contaminated postal facility in Trenton. These findings have implications for the design of biosurveillance systems. Although there were only 22 cases of anthrax, suspected or confirmed, 508 visits to the selected EDs for CE occurred during the peak period. This finding suggests that for detecting and trending of cases after a biologic terrorist attack, using syndromic surveillance might be obscured by patients with a concern rather than patients who are actually victims of the attack. In the chart review of CA patients for the peak third period, a substantial variation occurred in the reasons patients sought treatment with a CE to anthrax. Postal workers in a facility that had known cases of anthrax were at maximum risk. Postal workers in other facilities were at lower risk. Members of the general public who had no history of exposure but still wanted to be evaluated were at the lowest risk. Only 4% of the patients received radiographs. This low rate indicates that the majority of the patients were considered to be at little or no risk for having active pulmonary anthrax. A total of 65% of patients received a nasal swab for anthrax, a fairly routine procedure for these patients. Routine nasal swabs for anthrax detection were not recommended by CDC. Instead, CDC recommendations during that period indicated that culture of nasal swabs might be appropriate in the epidemiologic investigation of a known outbreak but would not rule out exposure to or infection with B. anthracis (4). Given the substantial volume of swabs, the minimal evidence of communication with public health departments, and the lower use of prophylactic antibiotics, these swabs probably were performed primarily for patient reassurance or in the mistaken belief that a culture of a nasal swab would rule out anthrax. There was a drop-off in the percentage of patients receiving nasal swabs for anthrax at the end of the one-month peak period which might represent the time at which physicians began following CDC recommendations. It might also represent a decrease in general concern about anthrax. Because of the substantial percentage of patients who received a nasal swab for anthrax and because the nasal swabs were not recommended, these findings suggest that guidelines (5) were not effectively reaching emergency physicians. These findings also suggest that current systems need to be reinforced and further developed to communicate recommendations immediately to ED physicians to manage the influx of victims of possible biologic terrorism. Additional studies have examined the need for better communication systems (6,7), including the use of the Internet (8,9). The percentage of patients who received antibiotics was 32%. The CDC recommendation at the time was that the basis for initiating antibiotic treatment should be exposure or contact, not laboratory test results (5). Whether the initiation of antibiotics was consistent with the CDC recommendation cannot be determined from the data. The same recommendations also called for 60 days of antibiotic prophylaxis. This report determined that only 19% of patients in the series who received an antibiotic prescription received one for >14 days. Sufficient data was not available to determine the extent that these prescriptions were written as "starter" prescriptions intended to be continued if deemed appropriate by the follow-up physician. No other reports specifically examine the volume or character of ED visits during this period. An epidemiologic study by CDC in October 2002 sought to determine the extent of the anthrax outbreak in New Jersey, assess potential sources of B. anthracis exposure, and prevent additional cases by developing and implementing control measures (10). However, this study did not assess the effects of the outbreak and media exposure on New Jersey EDs. In this study, methods were used that had been previously developed for syndromic surveillance to identify and characterize the effect of the anthrax attacks on EDs in the mitigation phase. The investigation was conducted on a large electronic database in which ICD-9 groups were used to identify patient visits of interest, time-series data to detect volume peaks, and a chart review of the affected patients. The level of detail available yielded information that might be valuable to public health preparations for the mitigation phase of a biologic terrorism attack. The data indicated that syndromic surveillance during the mitigation phase might have been affected by a substantial volume of patients concerned about exposure, although exposure was unlikely. The data also indicates that communication between emergency medicine practitioners and public health officials are vital during the mitigation phase and that communication needs improvement. LimitationsAll patients examined in the EDs were not included in this report, only those examined by ED physicians. However, this report encompassed the majority of these patients. Some variation in coding styles might have led to a variation in how patients were classified. However, this potential source of error was mitigated, because ICD-9 coding is performed centrally by a single group of coders who were trained in a similar manner. This report did not include all ED visits in northern New Jersey. However, because the volume represents approximately 30% of hospitals and 35%-40% of ED visits in northern New Jersey, the sample was representative of the total population of ED visits in northern New Jersey during this period. The chart review is limited by the retrospective nature of the study. Certain characteristics that were present were possibly underestimated, because they were not documented in the chart. ConclusionTechniques originally developed for syndromic surveillance identified an increase in CE visits that occurred during the 1-month period after the identification and media coverage of anthrax cases in New York City and at a Trenton postal facility. During the peak month, a higher increase of CE visits occurred in the Trenton EDs than in other EDs in the state. A substantial variation occurred in the reasons that patients sought medical treatment. Although the suspicion for anthrax in these patients appeared to be low, the majority of patients received a nasal swab for anthrax in excess of the guidelines from CDC. This finding suggests the need for improved communications during a biologic terrorist attack and readily available diagnostic and treatment guidelines. References
Table 1 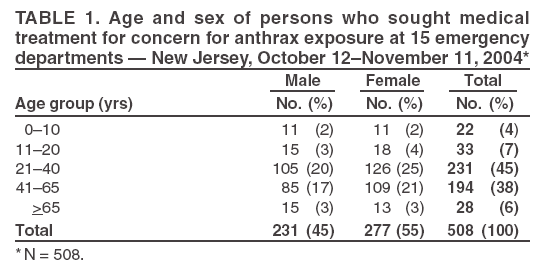 Return to top. Figure 1 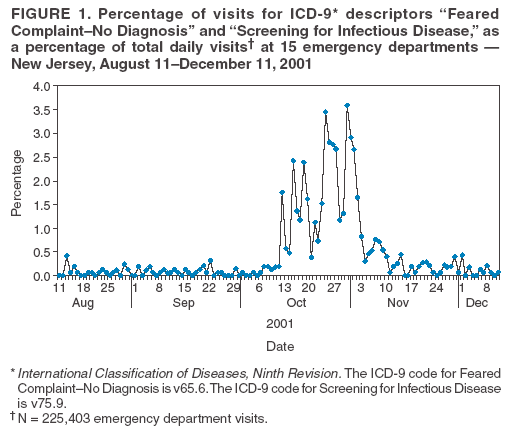 Return to top. Table 2 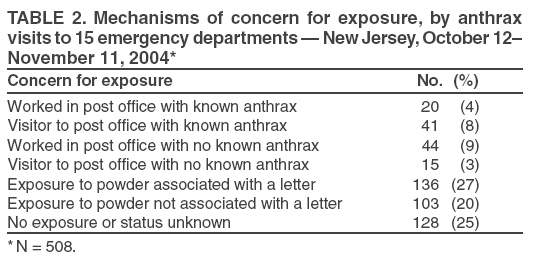 Return to top. Figure 2 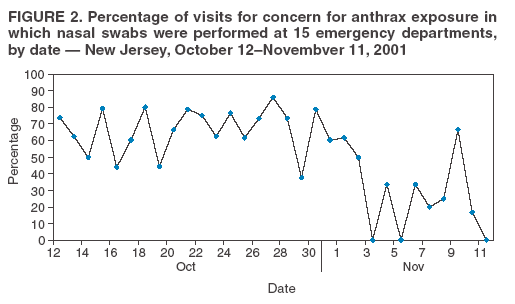 Return to top. Table 3 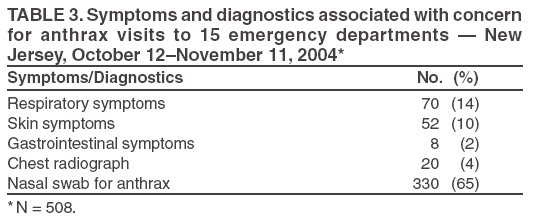 Return to top. Table 4  Return to top.
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Date last reviewed: 8/5/2005 |
|||||||||
|