Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail.
Recommended Antimicrobial Agents for the Treatment
and Postexposure Prophylaxis of Pertussis
2005 CDC Guidelines
Prepared by
Tejpratap Tiwari, M.D.
Trudy V. Murphy M. D.
John Moran M.D.
National Immunization Program, CDC
The material in this report originated in the National Immunization Program, Stephen L. Cochi, MD, Acting Director; and the Epidemiology
and Surveillance Division, Alison C. Mawle, PhD, Acting Director.
Corresponding preparer: Tejpratap Tiwari, National Immunization Program, CDC, 1600 Clifton Road NE, MS E-61, Atlanta, GA 30333.
Telephone: 404-639-8765; Fax: 404-639-8257; Email: tit2@cdc.gov.
Summary
The recommendations in this report were developed to broaden the spectrum of antimicrobial agents that are available
for treatment and postexposure prophylaxis of pertussis. They include updated information on macrolide agents other
than erythromycin (azithromycin and clarithromycin) and their dosing schedule by age group.
Introduction
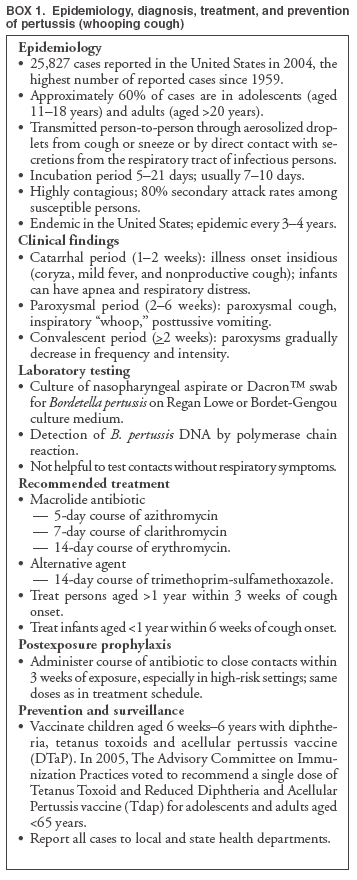
Pertussis is an acute bacterial infection of the respiratory tract that is caused by
Bordetella pertussis, a gram-negative bacterium (Box 1).
B. pertussis is a uniquely human pathogen that is transmitted from an infected person to
susceptible persons, primarily through aerosolized droplets of respiratory secretions or by direct contact with respiratory secretions
from the infected person.
Disease Burden
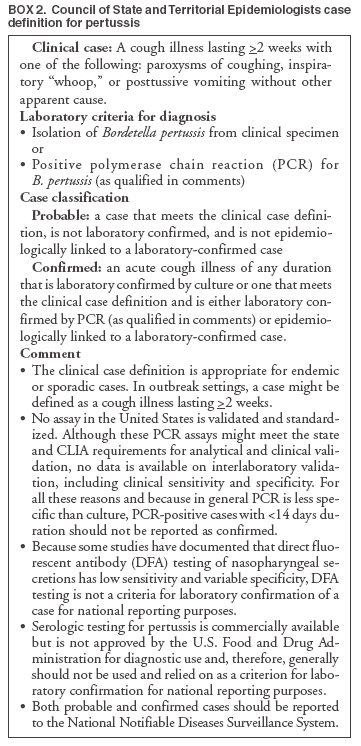
The Council of State and Territorial Epidemiologists (CSTE) reviewed and approved a standard case definition for
pertussis in June 1997(1,2) (Box 2). The national pertussis surveillance system is passive and relies on physicians to report cases
of pertussis to state and local health departments, which then report cases of pertussis weekly to the National Notifiable
Diseases Surveillance System (NNDSS). The reports are transmitted to CDC through the National Electronic
Telecommunications System for Surveillance (NETSS) and contain demographic data and supplemental clinical and epidemiologic information
for each reported pertussis case.
Despite high childhood vaccination coverage levels for pertussis vaccine
(3,4), pertussis remains a cause of
substantial morbidity in the United States. Pertussis is the only disease for which universal childhood vaccination is recommended
that has an increasing trend in reported cases in the United States. The disease is endemic in the United States with epidemic
cycles every 3--4 years. In the early vaccine years during 1922--1940, an average annual rate of 150 per 100,000 population
was reported (5,6). After introduction of universal vaccination during the 1940s, the incidence of reported pertussis
declined dramatically to approximately one case per 100,000 population.
During the preceding 3 decades, reports of pertussis steadily increased again in the United States, from a nadir of
1,010 cases in 1976 (3) to 25,827 in 2004 (2004 rate: 8.5 cases per 100,000 population)
(7); the number of reported pertussis cases in 2004 was the highest since 1959. Increased awareness and improved recognition of pertussis among clinicians, greater
access to and use of laboratory diagnostics (especially extensive polymerase chain reaction [PCR] testing), and increased
surveillance and reporting of pertussis by public health departments could have contributed to the increase in reported cases
(8). Some of the reported increase might constitute a real increase in the incidence of pertussis
(9). Although infants have the highest incidence of pertussis of any age group, adolescents and adults account for the majority of reported cases.
Clinical Manifestations
The incubation period of pertussis averages 7--10 days (range: 5--21 days)
(6,10) and has been reported to be as long as
6 weeks (11,12). Pertussis has an insidious onset with catarrhal symptoms (nasal congestion, runny nose, mild sore-throat,
mild dry cough, and minimal or no fever) that are indistinguishable from those of minor respiratory tract infections. Some
infants can have atypical disease and initially have apneic spells and minimal cough or other respiratory symptoms. The catarrhal
stage last approximately 1--2 weeks. The cough, which is initially intermittent, becomes paroxysmal. A typical paroxysm
is characterized by a succession of coughs that follow each other without inspiration. Paroxysms terminate in typical cases
with inspiratory "whoop" and can be followed by posttussive vomiting. Although children are often exhausted after a
coughing paroxysm, they usually appear relatively well between episodes. Paroxysms of cough usually increase in frequency and
severity as the illness progresses and usually persist for 2--6 weeks. Paroxysms can occur more frequently at night. The illness can
be milder and the characteristic whoop absent in children, adolescents, and adults who were previously vaccinated.
Convalescence is gradual and protracted. The severity of illness wanes, paroxysms subside, and the frequency of
coughing bouts decreases. A nonparoxysmal cough can continue for 2--6 weeks or longer. During the recovery period,
superimposed viral respiratory infections can trigger a recurrence of paroxysms.
Patients with pertussis often have substantial weight loss and sleep disturbance
(13). Conditions resulting from the effects
of the pressure generated by severe coughing include pneumothorax, epistaxis, subconjunctival hemorrhage, subdural
hematoma, hernia, rectal prolapse, urinary incontinence, and rib fracture
(14). Some infections are complicated by primary or
secondary bacterial pneumonia and otitis media. Infrequent neurologic complications include seizures and hypoxic encephalopathy.
Adolescents and adults with unrecognized or untreated pertussis contribute to the reservoir of
B. pertussis in the community. Patients with pertussis are most infectious during the catarrhal stage and during the first 3 weeks after cough onset. Pertussis
is highly infectious; the secondary attack rate exceeds 80% among susceptible persons
(15,16). Unvaccinated or incompletely vaccinated infants aged <12 months have the highest risk for severe and life-threatening complications and death
(5,8,17--25).
Differential Diagnosis
The differential diagnoses of pertussis include infections caused by other etiologic agents, including adenoviruses,
respiratory syncytial virus, Mycoplasma
pneumoniae,Chlamydia pneumoniae, and other
Bordetella species such as B.
parapertussis, and rarely B. bronchoseptica
(26) or B. holmseii (27). Despite increasing awareness and recognition of pertussis as a disease that
affects adolescents and adults, pertussis is overlooked in the differential diagnosis of cough illness in this population
(28).
Prevention
Vaccination of susceptible persons is the most important preventive strategy against pertussis. Universal childhood
pertussis vaccine recommendations have been implemented since the mid-1940s. For protection against pertussis during childhood,
the Advisory Committee on Immunization Practices (ACIP) recommends 5 doses of diphtheria and tetanus toxoid and
acellular pertussis (DTaP) vaccine at ages 2, 4, 6, 15--18 months, and 4--6 years
(29). Childhood vaccination coverage for
pertussis vaccines has been at an all-time high
(4). However, neither vaccination nor natural disease confers complete or
lifelong protective immunity against pertussis or reinfection. Immunity wanes after 5--10 years from the last pertussis vaccine
dose (3,8,30--34). Older children, adolescents, and adults can become susceptible to pertussis after a complete course
of vaccination during childhood.
During spring of 2005, two Tetanus Toxoid and Reduced Diphtheria Toxoid and Acellular Pertussis vaccines
adsorbed (Tdap) formulated for adolescents and adults were licensed in the United States
(BOOSTRIX®, GlaxoSmithKline
Biologicals, Rixensart, Belgium and ADACEL, Sanofi Pasteur, Toronto, Ontario, Canada). ACIP voted to recommend a single dose
of Tdap for adolescents aged 11--18 years in June 2005 and adults aged 19--64 years in October 2005.
Treatment of Pertussis
Maintaining high vaccination coverage rates among preschool children, adolescents, and adults and minimizing exposures
of infants and persons at high risk for pertussis is the most effective way to prevent pertussis. Antibiotic treatment of
pertussis and judicious use of antimicrobial agents for postexposure prophylaxis will eradicate
B. pertussis from the nasopharynx of
infected persons (symptomatic or asymptomatic). A macrolide administered early in the course of illness can reduce
the duration and severity of symptoms and lessen the period of communicability
(35). Approximately 80%--90% of patients
with untreated pertussis will spontaneously clear
B. pertussis from the nasopharynx within 3--4 weeks from onset of cough
(36); however, untreated and unvaccinated infants can remain culture-positive for >6 weeks
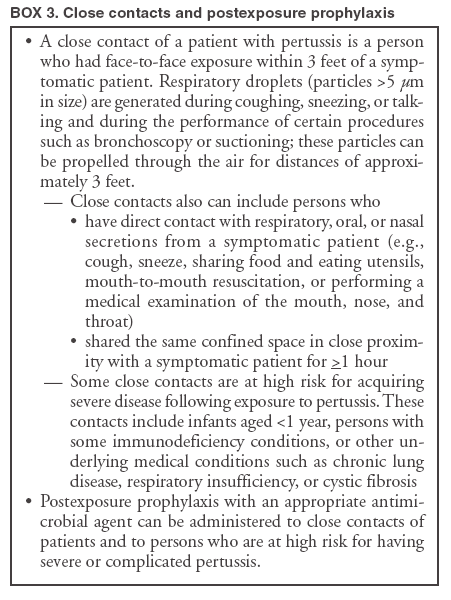
(37). Close asymptomatic contacts
(38) (Box 3) can be administered postexposure chemoprophylaxis to prevent secondary cases; symptomatic contacts should
be treated as cases.
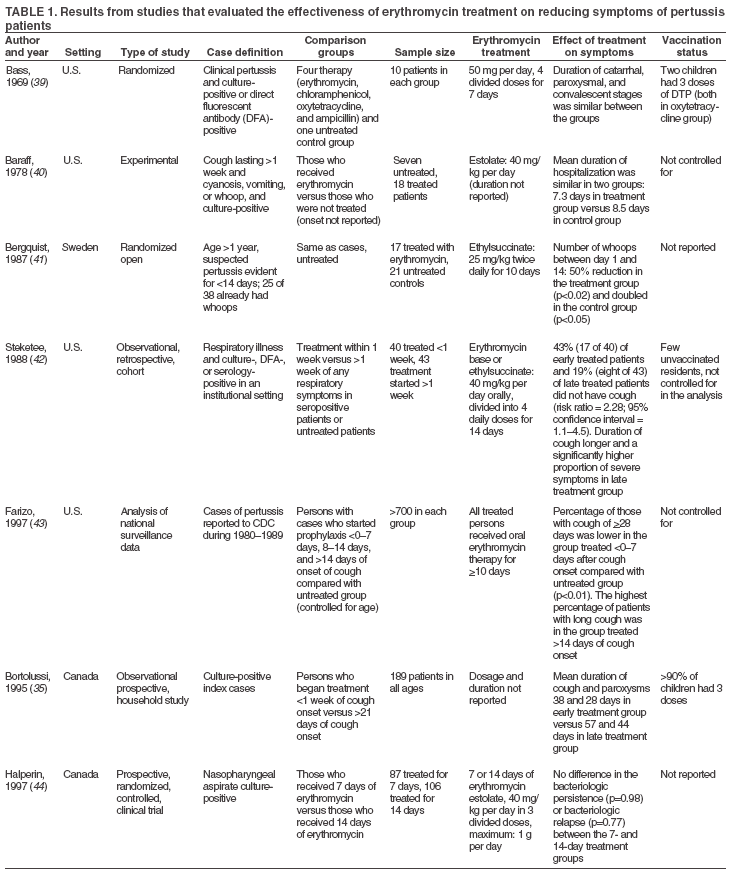
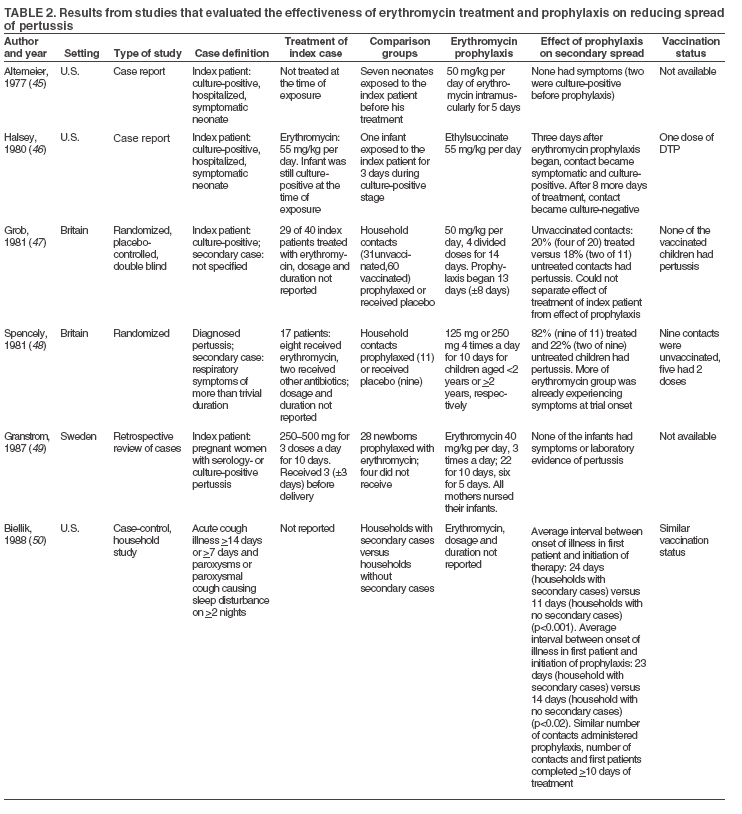
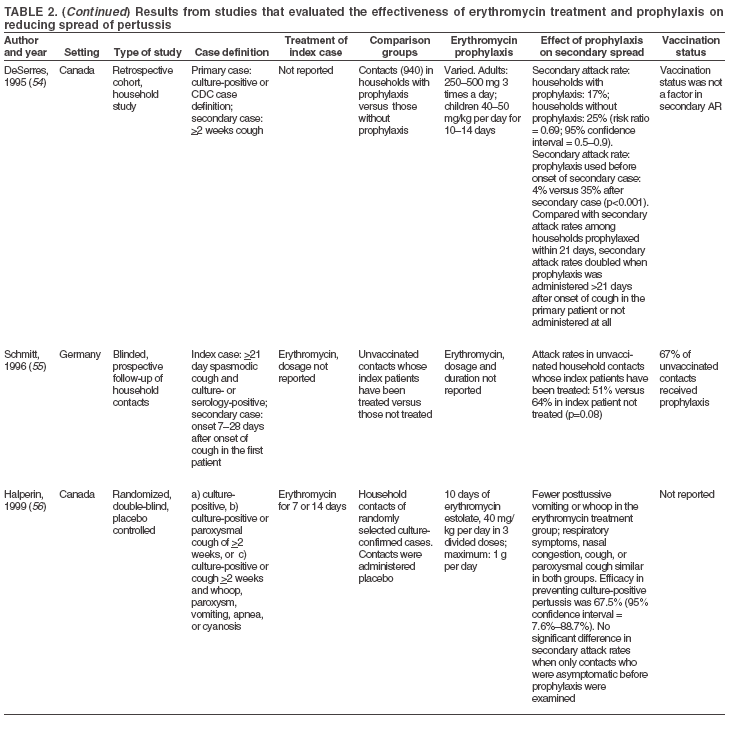
Erythromycin, a macrolide antibiotic, has been the antimicrobial of choice for treatment or postexposure prophylaxis
of pertussis. It is usually administered in 4 divided daily doses for 14 days. Although effective for treatment (Table 1)
and postexposure prophylaxis (Table 2), erythromycin is accompanied by uncomfortable to distressing side effects that result
in poor adherence to the treatment regimen. During the last decade, in vitro studies have demonstrated the effectiveness
against B. pertussis of two other macrolide agents (azithromycin and clarithromycin)
(57--64). Results from in vitro studiesare not always replicated in clinical studies and practice. A literature search and review was conducted for in vivo studies and
clinical trials that were conducted during 1970--2004 and used clarithromycin or azithromycin for the treatment and prophylaxis
of pertussis (Table 3). On the basis of this review, guidelines were developed to broaden the spectrum of macrolide
agents available for pertussis treatment and postexposure prophylaxis and are presented in this report to update previous
CDC recommendations (71). Treatment and postexposure prophylaxis recommendations are made on the basis of existing
scientific evidence and theoretical rationale.
Recommendations
I. General Principles
A. Treatment. The macrolide agents erythromycin, clarithromycin, and azithromycin are preferred for the treatment
of pertussis in persons aged >1 month. For infants aged <1 month, azithromycin is preferred; erythromycin and
clarithromycin are not recommended. For treatment of persons aged
>2 months, an alternative agent to macrolides is
trimethoprim-sulfamethoxazole (TMP--SMZ) (Table 4).
The choice of antimicrobial for treatment or prophylaxis should take into account effectiveness, safety (including
the potential for adverse events and drug interactions), tolerability, ease of adherence to the regimen prescribed, and
cost. Azithromycin and clarithromycin are as effective as erythromycin for treatment of pertussis in persons aged
>6 months, are better tolerated, and are associated with fewer and milder side effects than erythromycin. Erythromycin and
clarithromycin, but not azithromycin, are inhibitors of the cytochrome P450 enzyme system (CYP3A subclass) and can interact with
other drugs that are metabolized by this system. Azithromycin and clarithromycin are more resistant to gastric acid, achieve
higher tissue concentrations, and have a longer half-life than erythromycin, allowing less frequent administration (1--2 doses per
day) and shorter treatment regimens (5--7 days). Erythromycin is available as generic preparations and is considerably less
expensive than azithromycin and clarithromycin.
B. Postexposure prophylaxis. A macrolide can be administered as prophylaxis for close contacts of a person with
pertussis if the person has no contraindication to its use. The decision to administer postexposure chemoprophylaxis is made
after considering the infectiousness of the patient and the intensity of the exposure, the potential consequences of severe pertussis
in the contact, and possibilities for secondary exposure of persons at high risk from the contact (e.g., infants aged <12
months). For postexposure prophylaxis, the benefits of administering an antimicrobial agent to reduce the risk for pertussis and
its complications should be weighed against the potential adverse effects of the drug. Administration of postexposure
prophylaxis to asymptomatic household contacts within 21 days of onset of cough in the index patient can prevent symptomatic
infection. Coughing (symptomatic) household members of a pertussis patient should be treated as if they have pertussis. Because
severe and sometimes fatal pertussis-related complications occur in infants aged <12 months, especially among infants aged
<4 months, postexposure prophylaxis should be administered in exposure settings that include infants aged <12 months
or women in the third trimester of pregnancy. The recommended antimicrobial agents and dosing regimens for
postexposure prophylaxis are the same as those for treatment of pertussis (Table 4).
C. Special considerations for infants aged <6 months when using macrolides for treatment or
postexposure prophylaxis. The U.S. Food and Drug Administration (FDA) has not licensed any macrolide for use in infants aged
<6 months. Data on the safety and efficacy of azithromycin and clarithromycin use among infants aged <6 months are
limited.
Data from subsets of infants aged 1--5 months (enrolled in small clinical studies) suggest similar microbiologic
effectiveness of azithromycin and clarithromycin against pertussis as with older infants and children. If not treated, infants with
pertussis remain culture-positive for longer periods than older children and adults
(36,72). These limited data support the use
of azithromycin and clarithromycin as first-line agents among infants aged 1--5 months, based on their in vitro
effectiveness against B. pertussis, their demonstrated safety and effectiveness in older children and adults, and more convenient
dosing schedule.
For treatment of pertussis among infants aged <1 month (neonates), no data are available on the effectiveness
of azithromycin and clarithromycin. Abstracts and published case series describing use of azithromycin among infants aged
<1 month report fewer adverse events compared with erythromycin
(73); to date, use of azithromycin in infants aged <1
month has not been associated with infantile hypertrophic pyloric stenosis (IHPS). Therefore, for pertussis, azithromycin is
the preferred macrolide for postexposure prophylaxis and treatment of infants aged <1 month. In this age group, the risk
for acquiring severe pertussis and its life-threatening complications outweigh the potential risk for IHPS that has been
associated with erythromycin (74). Infants aged <1 month who receive a macrolide should be monitored for IHPS and other
serious adverse events.
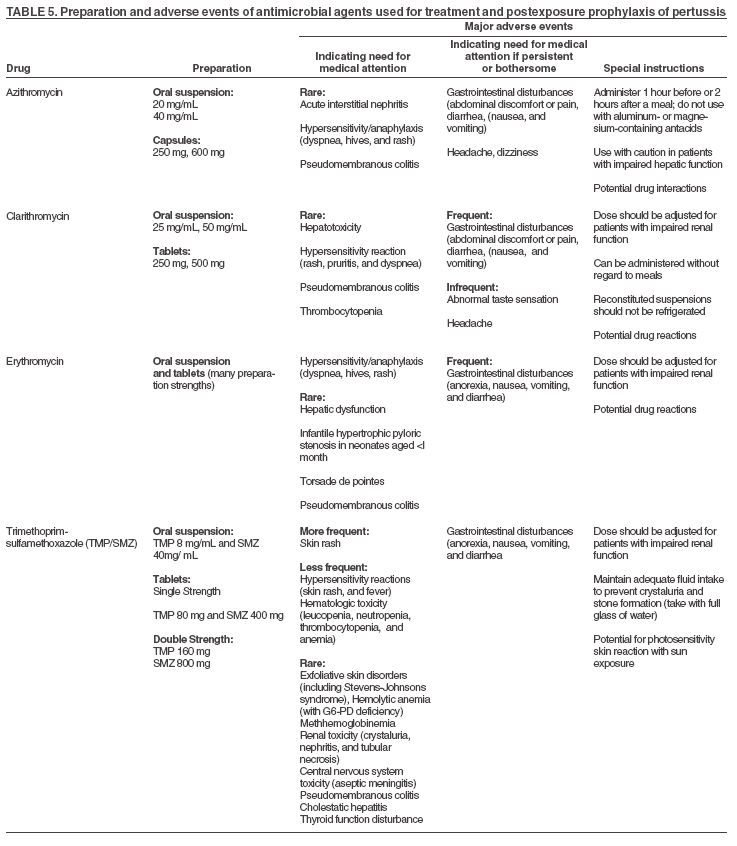
D. Safety. A comprehensive description of the safety of the recommended antimicrobials is available in the package
insert, or in the latest edition of the Red Book: Pharmacy's
Fundamental Reference. A macrolide is contraindicated if there is history
of hypersensitivity to any macrolide agent (Table 5). Neither erythromycin nor clarithromycin should be
administered concomitantly with astemizole, cisapride, pimazole, or terfenadine. The most commonly reported side effects of
oral macrolides are gastrointestinal (e.g., nausea, vomiting, abdominal pain and cramps, diarrhea, and anorexia) and rashes;
side effects are more frequent and severe with erythromycin use.
II. Specific Antimicrobial Agents
1. Azithromycin. Azithromycin is available in the United States for oral administration as azithromycin
dihydrate (suspension, tablets, and capsules). It is administered as a single daily dose.
Recommended regimen:
Infants aged <6 months: 10 mg/kg per day for 5 days.
Infants and children aged
>6 months: 10 mg/kg (maximum: 500 mg) on day 1, followed by 5 mg/kg per day
(maximum: 250 mg) on days 2--5.
Adults: 500 mg on day 1, followed by 250 mg per day on days 2--5.
Side effects include abdominal discomfort or pain, diarrhea, nausea, vomiting, headache, and dizziness. Azithromycin should be prescribed with caution to patients with impaired hepatic function. All patients should be cautioned not to
take azithromycin and aluminum- or magnesium-containing antacids simultaneously because the latter reduces the rate
of absorption of azithromycin. Monitoring of patients is advised when azithromycin is used concomitantly with
agents metabolized by the cytochrome P450 enzyme system and with other drugs for which the pharmacokinetics change
(e.g., digoxin, triazolam, and ergot alkaloids). Drug interactions reactions similar to those observed for erythromycin
and clarithromycin have not been reported. Azithromycin is classified as an FDA Pregnancy Category B drug
(75).
2. Erythromycin. Erythromycin is available in the United States for oral administration as erythromycin base (tablets
and capsules), erythromycin stearate (tablets), and erythromycin ethylsuccinate (tablets, powders, and liquids).
Because relapses have been reported after completion of 7--10 days of treatment with erythromycin, a 14-day course
of erythromycin is recommended for treatment of patients with pertussis or for postexposure prophylaxis of close contacts
of pertussis patients (76).
Recommended regimen:
Infants aged <1 month: not preferred because of risk for IHPS. Azithromycin is the recommended antimicrobial agent.
If azithromycin is unavailable and erythromycin is used, the dose is 40--50 mg/kg per day in 4 divided doses. These
infants should be monitored for IHPS.
Infants aged >1 month and older children: 40--50 mg/kg per day (maximum: 2 g per day) in 4 divided doses for 14 days.
Adults: 2 g per day in 4 divided doses for 14 days
Gastrointestinal irritation, including epigastric distress, abdominal cramps, nausea, vomiting, and diarrhea, are the
most common adverse effects associated with oral administration of erythromycin. Symptoms are dose-related. Some
formulations with enteric-coated tablets and the ester derivatives (e.g., ethylsuccinate) can be taken with food to minimize these side
effects. Hypersensitivity reactions (e.g., skin rashes, drug fever, or eosinophilia), cholestatic hepatitis, and sensorineural hearing
loss have occurred after administration of macrolides; severe reactions such as anaphylaxis are rare.
An increased risk for IHPS has been reported in neonates during the month after erythromycin administration. In one
case, pyloric stenosis occurred in a breastfeeding infant whose mother took erythromycin. In 1999, a cluster of seven cases of
IHPS were reported among neonates (all aged <3 weeks when prophylaxis was started) who had taken erythromycin after
exposure to a pertussis patient. In a cohort study, erythromycin prophylaxis was causally associated with IHPS (seven cases out of
157 erythromycin exposed infants versus zero cases out of 125 infants with no erythromycin exposure (relative risk: infinity
[95% confidence interval = 1.7--infinity]).
The high case-fatality ratio of pertussis in neonates underscores the importance of preventing pertussis among
exposed infants. Health-care providers who prescribe erythromycin rather than azithromycin to newborns should inform parents
about the possible risks for IHPS and counsel them about signs of IHPS.
Erythromycin is contraindicated if there is history of hypersensitivity to any macrolide
agent.Erythromycin should not be administered concomitantly with astemizole, cisapride, pimazole, or terfenadine. Rare cases of serious cardiovascular
adverse events, including electrocardiographic
QT/QTc interval prolongation, cardiac arrest, torsades de pointes, and other
ventricular arrhythmias, have been observed after concomitant use of erythromycin with these drugs.
Erythromycin is an inhibitor of the cytochrome P450 enzyme system (CYP3A subclass). Coadministration of
erythromycin and a drug that is primarily metabolized by CYP3A can result in elevations in drug concentrations that could increase
or prolong both the therapeutic and adverse effects of the concomitant drug. Drugs that are metabolized by CYP3A
include alfentanil, bromocriptine, cyclosporine, carbamazepine, cilostazol, disopyramide, dihydroergotamine, ergotamine,
lovastatin and simvastatin, methylprednisolone, quinidine, rifabutin, vinblastine, tacrolimus, triazolo-benzodiazepines (e.g.,
triazolam and alprazolam) and related benzodiazepines, and sildenafil. In addition, reports exists of drug interactions of
erythromycin with drugs not thought to be metabolized by CYP3A, including zidovudine, hexobarbital, phenytoin, and
valproate, theophylline, digoxin, and oral anticoagulants.
Erythromycin is classified as an FDA Pregnancy Category B drug
(76). Animal reproduction studies have failed
to demonstrate a risk to the fetus, but no adequate or well-controlled studies in humans exist.
3. Clarithromycin. Clarithromycin is available in the United States for oral administration as granules for oral
suspension and tablets.
Recommended regimen:
Infants aged <1 month: not recommended.
Infants and children aged
>1 month: 15 mg/kg per day (maximum: 1 g per day) in 2 divided doses each day for 7 days.
Adults: 1 g per day in two divided doses for 7 days.
The most common adverse effects associated with clarithromycin include epigastric distress, abdominal cramps,
nausea, vomiting, and diarrhea. Hypersensitivity reactions (e.g., skin rashes, drug fever, or eosinophilia), hepatotoxicity, and
severe reactions such as anaphylaxis are rare. Because of its similarity to erythromycin, both chemically and
metabolically, clarithromycin should not be administered to infants aged <1 month because it is unknown if the drug can be
similarly associated with IHPS. The drug is contraindicated if there is history of hypersensitivity to any macrolide agent. Similar
to erythromycin, clarithromycin should not be administered concomitantly with astemizole, cisapride, pimazole, or
terfenadine. Clarithromycin inhibits the cytochrome P450 enzyme system (CYP3A subclass), and coadministration of clarithromycin
and a drug that is primarily metabolized by CYP3A can result in elevations in drug concentrations that could increase or
prolong both the therapeutic and adverse effects of the concomitant drug. Clarithromycin can be administered without
dosage adjustment in patients with impaired hepatic function and normal renal function; however, drug dosage and interval
between doses should be reassessed in the presence of impaired renal function. Clarithromycin is classified by FDA as a
Pregnancy Category C drug (76). Animal reproduction studies have shown an adverse effect on the fetus; no adequate or
well-controlled studies in humans exist.
4. Alternate agent (TMP--SMZ). Data from clinical studies indicate that TMP--SMZ is effective in eradicating
B. pertussis from the nasopharynx
(64,77,78). TMP--SMZ is used as an alternative to a macrolide antibiotic in patients aged
>2 months who have contraindication to or cannot tolerate macrolide agents, or who are infected with a macrolide-resistant strain of
B. pertussis. Macrolide-resistant B.
pertussis is rare. Because of the potential risk for kernicterus among infants,
TMP--SMZ should not be administered to pregnant women, nursing mothers, or infants aged <2 months.
Recommended regimen (79):
Infants aged <2 months: contraindicated.
Infants aged >2 months and children: trimethoprim 8 mg/kg per day, sulfamethoxazole 40 mg/kg per day in 2
divided doses for 14 days.
Adults: trimethoprim 320 mg per day, sulfamethoxazole 1,600 mg per day in 2 divided doses for 14 days.
Patients receiving TMP-SMZ might experience gastrointestinal adverse effects, hypersensitivity skin reactions, and
rarely, Stevens-Johnson syndrome, toxic epidermal necrolysis, blood dyscrasias, and hepatic necrosis. TMP--SMZ is
contraindicated if there is known hypersensitivity to trimethoprim or sulfonamides. TMP--SMZ should be prescribed with caution to
patients with impaired hepatic and renal functions, folate deficiency, blood dyscrasias, and in older adults because of the
higher incidence of severe adverse events. Patients taking TMP--SMZ should be instructed to maintain an adequate fluid intake
to prevent crystalluria and renal stones. Drug interactions must be considered when TMP--SMZ is used concomitantly
with drugs, including methotrexate, oral anticoagulants, antidiabetic agents, thiazide diuretics, anticonvulsants, and
other antiretroviral drugs. TMP--SMZ is classified by FDA as a Pregnancy Category C drug
(76). Animal reproduction studies have indicated an adverse effect on the fetus; no adequate or well-controlled studies in humans exist.
5. Other antimicrobial agents. Although in vitro activity against
B. pertussis has been demonstrated for other
macrolides such as roxithromycin and ketolides (e.g., telithromycin)
(60), no published data exist on the clinical effectiveness of
these agents.
Other antimicrobial agents such as ampicillin, amoxicillin, tetracycline, chloramphenicol, fluoroquinolones
(e.g., ciprofloxacin, levofloxacin, ofloxacin, moxifloxacin), and cephalosporins exhibit various levels of in
vitroinhibitory activity against B.
pertussis, but in vitro inhibitory activity does not predict clinical effectiveness. The clinical effectiveness of
these agents for treatment of pertussis has not been demonstrated. For example, both ampicillin and amoxicillin were ineffective
in clearing B. pertussis from nasopharynx
(80). Poor penetration into respiratory secretions was proposed as a possible
mechanism for failure to clear B. pertussis
from the nasopharynx (81). The minimum inhibitory concentration of
B. pertussis to the cephalosporins is unacceptably high
(82). In addition, tetracyclines, chloramphenicol, and fluoroquinolones have
potentially harmful side effects in children. Therefore, none of the above antimicrobial agents are recommended for treatment
or postexposure prophylaxis of pertussis.
Acknowledgements
These guidelines were developed by CDC in consultation with the American Academy of Pediatrics, the American Academy of
Family Physicians (AAFP), and by the Healthcare Infection Control Practices Advisory Committee (HICPAC). The authors would like to
thank Steve Gordon, M.D., Cleveland Clinic Foundation, Nalini Singh, M.D., HICPAC, Richard Clover M.D. (AAFP), Dalya Guris
M.D., National Immunization Program, CDC, and the CDC Pertussis Team for contributing to this report.
Council of State and Territorial Epidemiologists (CSTE). 1997 Position Statements. CSTE National Meeting, Saratoga Springs, NY: CSTE.
Position statement 9.
Guris D, Strebel PM, Bardenheier B, et al. Changing epidemiology of pertussis in the United States: increasing reported incidence
among adolescents and adults, 1990--1996. Clin Infect Dis 1999;28:1230--7.
Tanaka M, Vitek CR, Pascual FB, Bisgard KM, Tate JE, Murphy TV. Trends in pertussis among infants in the United States, 1980--1999.
JAMA2003;290:2968--75.
Gordon JE, Hood RI. Whooping cough and its epidemiological anomalies. Am J Med Sc 1951;222:333--61.
Fine PEM, Clarkson JA, Miller E. The efficacy of pertussis vaccines under conditions of household exposure: further analysis on the 1978-80
PHLS/ERL study in 21 area health authorities in England. Int J Epidemiol 1988;17:635--4.
Heininger U, Cherry JD, Stehr K, et al. Comparative efficacy of the Lederle/Takeda acellular pertussis component DTP (DTaP) vaccine and
Lederle whole-cell component DTP vaccine in German children after household exposure. Pediatrics 1998;102:546--53.
Mark A, Granström M. Impact of pertussis on the afflicted child and family. Ped Infect Dis J 1992;11:554--7.
Postels-Moltani S, SchmittHJ, Wirsing von Konig CH, et al. Symptoms and complications of pertussis in adults. Infection 1995;23:139--42.
Kendrick PL. Secondary familial attack rates from pertussis in vaccinated and unvaccinated children. Am J Hyg 1940;32:89--91.
Medical Research Council. The prevention of whooping-cough by vaccination: a Medical Research Council Investigation. BMJ 1951;47:1463--71.
Izurieta HS, Kenyon TA, Strebel PM, et al. Risk factors for pertussis in young infants during an outbreak in Chicago in 1993. Clin Infect
Dis 1996;22:503--7.
Nelson JD. The changing epidemiology of pertussis in young infants: the role of adults as reservoirs of infections. Am J Dis Child 1978;132:371--3.
Deen JL, Mink CM, Cherry JD, et al. Household contact study of
Bordetella pertussis infection. Clin Infect Dis 1995;21:1211--9.
Gan VN, Murphy TV. Pertussis in hospitalized children. Am J Dis Child 1990;144:1130--4.
Trollfors B, Rabo E. Whooping cough in adults. BMJ 1981;5:696--7.
Riitta H. Clinical symptoms and complications of whooping cough in children and adults. Acta Paediatr Scand 1982;298:13--20.
Wortis N, Strebel PM, Wharton M, et al. Pertussis deaths: report of 23 cases in the United States. Pediatrics 1996;97:607--12.
Halperin SA, Wang EEL, Law B, et al. Epidemiological features of pertussis in hospitalized patients in Canada, 1991--1997: report of
the immunization monitoring program---active (IMPACT). Clin Infect Dis 1999;28:1238--43.
Stefanelli P, Mostrantonio P, Hausman SZ, Giuliano M, Burns DL. Molecular characterization of two
Bordetella bronchiseptica strains isolated
from children with coughs. J Clin Microbiol 1997;35:1550--5.
Yih WK, Silva EA, Ida J, Harrington N, Lett SM, George H.
Bordetella holmesii-like organisms isolated from Massachusetts patients with
pertussis-like symptoms. Emerg Infect Dis 1999;5:441--3.
Keitel WA, Edwards KM. Pertussis in adolescents and adults: time to reimmunize? Semin Respir Infect 1995;10:51--7.
Jenkinson D. Duration of effectiveness of pertussis vaccine: evidence from a 10-year community study. Br J Med 1988;296:612--4.
Pichichero ME, Casey JR. Acellular pertussis vaccines for adolescents. Pediatr Infect Dis J 2005;24:117--26.
Olin P, Gustafsson L, Barreto L, et al. Declining pertussis incidence in Sweden following the introduction of acellular pertussis vaccine.
Vaccine 2003;21:2015--21.
Lambert HJ. Epidemiology of a small pertussis outbreak in Kent County, Michigan. Pub Health Rep 1965;80:365--9.
Salmaso S, Mastrantonio P, Tozzi AE, et al. Sustained efficacy during the first 6 years of life of 3-component acellular pertussis vaccines
administered in infancy: the Italian experience. Pediatrics 2001;108:81.
Bortolussi R, Miller B, Ledwith M, et al. Clinical course of pertussis in immunized children. Ped Infect Dis J 1995;14:870--4.
Kwantes W, Joynson HM, Williams WO.
Bordetella pertussis isolation in general practice: 1977--79 whooping cough epidemic in West Glamorgan.
J Hyg Camb 1983;90:149--58.
Henry R, Dorman D, Skinner J, et al. Limitations of erythromycin in whooping cough. Med J Aust 1981;2:108--9.
Garner JS, Hospital Infection Control Practices Advisory Committee. Guideline for isolation precautions in hospitals. Infect Control
Hosp Epidemiol 1996;17:53--80.
Bass JW, Klenk EL, Kotheimer JB, et al. Antimicrobial treatment of pertussis. J Pediatr 1969;75:768--81.
Baraff LJ, Wilkins J, Wehrle PF. The role of antibiotics, immunizations, and adenoviruses in pertussis. Pediatrics 1978;61:224--30.
Bergquist S, Bernander S, Dahnsjo H, et al. Erythromycin in the treatment of pertussis: a study of bacteriologic and clinical effects. Ped Infect Dis
J 1987;6:458--61.
Steketee RW, Wassilak SGF, Adkins WN, et al. Evidence of a high attack rate and efficacy of erythromycin prophylaxis in a pertussis outbreak in
a facility for developmentally disabled. J Infect Dis 1988;157:434--40.
Farizo KM, Cochi SL, Zell ER, et al. Epidemiological features of pertussis in the United States, 1980--89. Clin Infect Dis 1992;14:708--19.
Halperin SA, Bortolussi R, Langley JM, et al. Seven days of erythromycin estolate is as effective as fourteen days for the treatment of
Bordetella pertussis infections. J Pediatr 1997;100:65--71.
Altemeier WA, Ayoub EM. Erythromycin prophylaxis for pertussis. Pediatrics 1977;59:623--5.
Halsey N, Welling MA, Lehman RM. Nosocomial pertussis: a failure of erythromycin treatment and prophylaxis. Am J Dis Child 1980;134:521--2.
Grob PR. Prophylactic erythromycin for whooping-cough contacts [letter]. Lancet 1981;1:772.
Spencely M, Lambert HP. Prophylactic erythromycin for whooping-cough contacts [letter]. Lancet 1981;1:772.
Granstrom G, Sterner G, Nord CE, et al. Use of erythromycin to prevent pertussis in newborns of mothers with pertussis. J Infect
Dis 1987;155:1210--4.
Biellik RJ, Patriarca PA, Mullen JR, et al. Risk factors for community- and household-acquired pertussis during a large-scale outbreak in
central Wisconsin. J Infect Dis 1988;157:1134--41.
Sprauer MA, Cochi SL, Zell ER, et al. Prevention of secondary transmission of pertussis in households with early use of erythromycin. Am J
Dis Child 1992;146:177--81.
Fisher MC, Long SS, McGowan KL, Kaselis E, Smith DG. Outbreak of pertussis in a residential facility for handicapped people. J
Pediatr 1989;114:934--9.
Wirsing von Konig CH, Postels-Multani S, Bock HL, et al. Pertussis in adults: frequency of transmission after household exposure.
Lancet 1995;346:1326--9.
De Serres G, Boulianne N, Duval B. Field effectiveness of erythromycin prophylaxis to prevent pertussis within families. Ped Infect Dis
J 1995;14:969--75.
Schmitt HJ, Wirsing von Konig CH, Neiss A, et al. Efficacy of acellular pertussis vaccine in early childhood after household exposure.
JAMA 1996;275:37--41.
Halperin SA, Botolussi R, Langley JM, et al. A randomized, placebo-controlled trial of erythromycin estolate chemoprophylaxis for
household contacts of children with culture-positive
Bordetella pertussis infection. Pediatrics 1999;104:42.
Hoppe JE, Eichhorn A. Activity of new macrolides against
Bordetella pertussis and Bordetella
parapertussis. Eur J Clin Microbiol Infect Dis 1989;8:653--4.
Kurzinsky TA, Boehm DM, Rott-petri JA, Schell RF, Allison PE. Antimicrobial susceptibilities of
Bordetella species isolated in a multicenter
pertussis surveillance project. Antimicrobn Agents Chemother 1988;32:137--40.
Hoppe JE, Bryskier A. In vitro susceptibilities of
Bordetella pertussis and Bordetella
parapertussis to two ketolides, (HMR 3004 and HMR 3647),
four macrolides (azithromycin, clarithromycin, erythromycin A, and roxithromycin), and two ansamycins (rifampin and rifapentine). Antimicrob
Agents Chemother 1998;42:965--6.
Hardy DJ, Hensey DM, Beyer JM Voktko c, McDonald EJ, Fennandes PB. Comparative in vitro activities of new 14-, 15, and
16-membered macrolides. Antimicrob Agents Chemother 1988;32:1710--9.
Bannatyne RM, Cheung R. Antimicrobial susceptibility of
Bordetella pertussis strains isolated from 1960 to 1981. Antimicrob Agents
Chemother 1982;21:666--7.
Mortensen JE, Rodgers GL. In vitro activity of gemifloxacin and other antimicrobial agents against isolates of
Bordetella pertussis and Bordetella parapertussis.
J Antimicrob Chemother 2000;45:47--9.
Doucet-Populaire F, Pangon B, Doerman HP, Boudjadja A, Ghnassia JC. In vitro activity of a new fluroquinolone BAY 128039 in comparison
with ciprofloxacin and macrolides against Bordetella pertussis.
In: Programs and abstracts of the 37th Interscience Conference on Antimicrobial
Agents and Chemotherapy, Toronto, Ontario, Canada, September 28--October 1, 1997 (Abstract F-145:170).
Felmingham D, Robbins MJ, Leakey A, et al. The comparative in vitro activity of HMR 3647, a ketolide antimicrobial, against clinical
bacterial isolates. In: Programs and abstracts of the 37th Interscience Conference on Antimicrobial Agenta and Chemotherapy, Toronto, Ontario,
Canada, September 28--October 1, 1997 (Abstract F-116:166).
Aoyama T, Sunakawa K, Iwata S, Takeuchi Y, Fujii R. Efficacy of short-term treatment of pertussis with clarithromycin and azithromycin.
J Pediatr 1996;129:761--4.
Bace A, Zrnic J, BegovacJ, Kuzmanovic N, Culig J. Short-term treatment of pertussis with azithromycin in infants and young children. Eur J
Clin Microbiology Infect Dis 1999;18:296--8.
Bace A, Kuzmanovic N, Novac D, Anic-Milic T, Radosevic S, Culig J. Clinical comparative study of azithromycin and erythromycin in
the treatment of pertussis---preliminary results. Abstract #36, ICMAS-5, Jan 26-28, 2000, Seville.
Langley JM, Halperin SA, Boucher FD, Smith B, Pediatric Investigators Collaborative Network on Infections in Canada. Azithromycin is
as effective as and better tolerated than erythromycin estolate for the treatment of pertussis. Pediatrics 2004;14:96--101.
Lebel MH, Mehra S. Efficacy and safety of clarithromycin versus erythromycin for the treatment of pertussis: a prospective, randomized, single
blind trial. Pediatr Infect Dis J 2001;20:1149--54.
Pichichero ME, Hoeger WJ, Casey JR. Azithromycin for the treatment of pertussis. Pediatr Infect Dis J 2003;22:847--9.
Riitta H. The effect of early erythromycin treatment on the infectiousness of whooping cough patients. Acta Paediatr Scand 1982;298:10--12.
Friedman DS, Curtis RC, Schauer SL, et al. Surveillance for transmission and antibiotic adverse events among neonates and adults exposed to
a healthcare worker with pertussis. Infect Control Hosp Epidemiol 2004;25:967--73.
Honein MA, Paulozzi LJ, Himelright IM, et al. Infantile hypertrophic pyloric stenosis after pertussis prophylaxis with erythromycin: a case
review and cohort study. Lancet 1999;354:2101--5.
US Food and Drug Administration. Current categories for drug use in pregnancy. Washington, DC: FDA Consumer 2001;35:3.
Henry RL, Dorman DC, Skinner J, et al. Antimicrobial therapy in whooping cough. Med J Aust 1981;2:27--8.
Hoppe JE, Halm U, Hagedorn HJ, et al. Comparison of erythromycin ethylsuccinate and co-trimoxazole for treatment of pertussis.
Infection 1989;17:227--31.
American Academy of Pediatrics. Pertussis. In: Peter G, ed. 1997 Red Book: Report of the Committee on Infectious Diseases. 24th ed. Elk
Grove Village, IL: American Academy of Pediatrics; 1997.
Trollfors B. Effect of erythromycin and amoxycillin on
Bordetella pertussis in the nasopharynx. Infection 1978;6:228--30.
Hoppe JE, Haug A. Treatment and prevention of pertussis by antimicrobial agents (part II). Infection 1988;16:148--52.
Hoppe JE. State of art in antibacterial susceptibility of
Bordetella pertussis and antibiotic treatment of pertussis. Infection 1998;26:242--6.
Members of the CDC Pertussis Team
Karen Broder, MD, Margaret Cortese, MD Amanda Cohn, MD, Katrina Kretsinger, MD, Barbara Slade, M.D., Kristin Brown, MPH,
Christina Mijalski, MPH, Kashif Iqbal, MPH, Pamela Srivastava, MPH.
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services.References to non-CDC sites on the Internet are
provided as a service to MMWR readers and do not constitute or imply
endorsement of these organizations or their programs by CDC or the U.S.
Department of Health and Human Services. CDC is not responsible for the content
of pages found at these sites. URL addresses listed in MMWR were current as of
the date of publication.
Disclaimer
All MMWR HTML versions of articles are electronic conversions from ASCII text
into HTML. This conversion may have resulted in character translation or format errors in the HTML version.
Users should not rely on this HTML document, but are referred to the electronic PDF version and/or
the original MMWR paper copy for the official text, figures, and tables.
An original paper copy of this issue can be obtained from the Superintendent of Documents,
U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800.
Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to
mmwrq@cdc.gov.