 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Counseling to Prevent Skin CancerRecommendations and Rationale of the U.S. Preventive Services Task Force Corresponding author: Alfred O. Berg, M.D., M.P.H., Chair, U.S. Preventive Services Task Force, c/o Center for Primary Care, Prevention, and Clinical Partnerships, Agency for Healthcare Research and Quality; e-mail: uspstf@ahrq.gov. This report was written by the U.S. Preventive Services Task Force with editorial and technical support from the Agency for Healthcare Research and Quality, U.S. Department of Health and Human Services. The standard MMWR format has been modified to accommodate other publications of the report. Summary This statement summarizes the current U.S. Preventive Services Task Force (USPSTF) recommendation on counseling to prevent skin cancer and the supporting scientific evidence, and updates the 1996 recommendation contained in the Guide to Clinical Preventive Services, Second Edition (U.S. Preventive Services Task Force. Screening for skin cancer. In: Guide to clinical preventive services, 2nd ed. Washington DC: US Department of Health and Human Services, Office of Disease Prevention and Health Promotion, 1996:141--52). The USPSTF finds insufficient evidence to recommend for or against routine counseling by primary care clinicians to prevent skin cancer. Although counseling parents may increase children's use of sunscreen, the USPSTF found little evidence to determine the effects of counseling on the sun protection behaviors of adults. These behaviors include wearing protective clothing, reducing excessive sun exposure, avoiding sun lamps and tanning beds, or practicing skin self-examination. The USPSTF, an independent panel of private sector experts in primary care and prevention, systematically reviews the evidence of effectiveness of a wide range of clinical preventive services, including screening tests, counseling, and chemoprevention. Members of the USPSTF represent the fields of family medicine, gerontology, obstetrics/gynecology, pediatrics, nursing, and prevention research. IntroductionThis statement summarizes the current U.S. Preventive Services Task Force (USPSTF) recommendation on counseling to prevent skin cancer and the supporting scientific evidence, and updates the 1996 recommendation contained in the Guide to Clinical Preventive Services, Second Edition (1). The USPSTF, an independent panel of private sector experts in primary care and prevention, systematically reviews the evidence of effectiveness of a wide range of clinical preventive services, including screening tests, counseling, and chemoprevention. The Task Force grades its recommendations according to one of five classifications (A, B, C, D, I), reflecting the strength of evidence and magnitude of net benefit (benefits minus harms) (Box 1). The USPSTF grades the quality of the overall evidence for a service on a 3-point scale (good, fair, poor) (Box 2). This recommendation and rationale statement and complete information on which this statement is based, including evidence tables and references, are available at http://www.ahrq.gov/clinic/uspstfix.htm (2) and in print by subscription through the AHRQ Clearinghouse (1-800-358-9295 or e-mail at ahrqpubs@ahrq.gov) and through the National Guideline Clearinghouse™ at http://www.guideline.gov. Summary of RecommendationThe U.S. Preventive Services Task Force concludes that the evidence is insufficient to recommend for or against routine counseling by primary care clinicians to prevent skin cancer. I recommendation. The USPSTF found insufficient evidence to determine whether clinician counseling is effective in changing patient behaviors to reduce skin cancer risk. Counseling parents may increase the use of sunscreen for children, but there is little evidence to determine the effects of counseling on other preventive behaviors (such as wearing protective clothing, reducing excessive sun exposure, avoiding sun lamps/tanning beds, or practicing skin self-examination) and little evidence on potential harms. Clinical Considerations
Scientific EvidenceEpidemiology and Clinical ConsequencesMelanoma is a leading cause of cancer death in the United States. The lifetime risk for dying of melanoma is 0.36% in white men and 0.21% in white women (3). Between 1973 and 1995, the age-adjusted incidence of melanoma increased more than 100%, from 5.7 per 100,000 people to 13.3 per 100,000 people. The increase in annual incidence rates is likely due to several factors, including increased sun exposure and possibly earlier detection of melanoma. Although primary prevention efforts have focused on young people, the elderly (especially elderly men) bear a disproportionate burden of morbidity and mortality from melanoma and nonmelanoma skin cancer. Men older than age 65 account for 22% of the newly diagnosed cases of malignant melanoma each year and women in the same age group account for 14%. Basal cell and squamous cell carcinomas are more than 10 times as common as melanoma but account for less morbidity and mortality. Squamous cell cancers, however, may account for 20% of all deaths from skin cancer. Effectiveness of Available InterventionsPreventive strategies include reducing sun exposure (e.g., by wearing protective clothing and using sunscreen regularly), avoiding sunlamps and tanning equipment, and practicing skin self-examination. There is little direct evidence, however, that any of these interventions reduce skin cancer morbidity or mortality. Reducing Sun Exposure Avoiding direct sunlight by staying indoors or in the shade or by wearing protective clothing is the most effective measure for reducing exposure to ultraviolet light, but there are no randomized trials of sun avoidance to prevent skin cancer. In numerous observational studies, increased sun exposure in childhood and adolescence is associated with increased risk for nonmelanoma skin cancer, which usually occurs in sun-exposed areas such as the face. Recent studies provide a more complex picture of the relationship between sun exposure and melanoma, however. Although melanoma incidence is higher in regions near the equator where ultraviolet exposure is most intense, melanoma often occurs in areas of the body not exposed to the sun. In observational studies, intermittent or intense sun exposure was associated with increased risk for melanoma; chronic exposure was associated with lower risk, as was the ability to tan (4--7). Sunlamp and Tanning Bed Avoidance Six of 19 case-control studies found a positive association between use of sun lamps and melanoma risk, but most did not adjust for recreational sun exposure or for the dosage and timing of sunlamp exposure (8). Among nine studies that examined the duration, frequency, or timing of sunlamp or tanning bed exposure, four found a positive association, particularly if the dose of exposure was high and if it caused burning. Sunscreen Use Daily sunscreen use on the hands and face reduced the total incidence of squamous cell cancer in a randomized trial of 1,621 residents in Australia (rate ratio [RR]: 0.61; 95% confidence interval [CI] = 0.46--0.81) (9). Sunscreen had no effect on basal cell cancer. Based on this trial, 140 people would need to use sunscreen daily for 4½ years to prevent one case of squamous cell cancer. An earlier randomized trial demonstrated that sunscreen use reduced solar keratoses, precursors of squamous cell cancers (10). There are no direct data about the effect of sunscreen on melanoma incidence. An unblinded randomized trial showed that children at high risk for skin cancers who used sunscreen developed fewer nevi than those who did not. Several epidemiologic studies have found higher risk for melanoma among users of sunscreens than among nonusers (11--13). A recent meta-analysis of population-based case-control studies found no effect of sunscreen use on risk for melanoma (14). The conflicting results may reflect the fact that sunscreen use is more common among fair-skinned people, who are at higher risk for melanoma, than it is among darker-skinned people; or, this finding may reflect the fact that sunscreen use could be harmful if it encourages longer stays in the sun without protecting completely against cancer-causing radiation. Skin Self-Examination The only evidence for the effectiveness of skin self-examination comes from a single case-control study (1,15). After adjustment for other risk factors, skin self-examination was associated with lower incidence of melanoma (odds ratio [OR]: 0.66; 95% CI = 0.44--0.99) and lower mortality from melanoma (OR: 0.37; 95% CI = 0.16--0.84), although the definition of "self-examination" was limited. This study did not provide sufficient evidence that skin self-examination would reduce the incidence of melanoma or improve outcomes of melanoma. Effectiveness of CounselingCommunity and worksite educational interventions have demonstrated effectiveness for increasing the use of skin protection measures, such as wearing hats and long-sleeve shirts and staying in the shade; however, evidence addressing the effectiveness of clinician counseling to prevent skin cancer is extremely limited. Most studies of counseling have examined intermediate outcomes such as knowledge and attitudes rather than changes in behavior. In a recent survey, 60% of pediatricians said that they usually or always counsel patients about skin protection, but advice to use sunscreen is more common than advice about wearing protective clothing or avoiding the midday sun (16). Simple reminders and instructional materials for clinicians can overcome some of the barriers to regular counseling. A randomized trial of a community-based intervention involving 10 towns in New Hampshire suggests that office-based counseling by physicians may be an effective component of a multimodal program to promote skin protection (17). The proportion of children using some sun protection increased significantly in the intervention towns (from 78% to 87%) compared to a decrease in the control communities (from 85% to 80%). More parents reported receiving some sun protection information from a clinician in the intervention towns. However, most of the change was due to increased sunscreen use rather than to reduced sun exposure. Potential Harms of Skin Protection BehaviorsThere are limited data regarding potential harms of counseling or of specific skin protection behaviors. Skin cancer counseling that focuses on the use of sunscreen could possibly lead to a false sense of security, which might lead to more time in the sun. For example, a randomized trial with young adults found that those who used sunscreen with a high sun protection factor (SPF) stayed longer in the sun than those who used sunscreen with a lower SPF (18). There has been some concern that use of SPF of 15 results in vitamin D deficiency. However, a randomized trial among people over 40 years of age found that sunscreen use over the summer had no effect on 25-hydroxyvitamin D3 levels. Concerns related to sun avoidance include reduced physical activity levels among children and negative effects on mental health. However, no studies have evaluated the effects of sun protection behaviors on these outcomes. Recommendations Of OthersThe American Cancer Society (19), the American Academy of Dermatology (20), the American Academy of Pediatrics (21), the American College of Obstetricians and Gynecologists (22), and a National Institutes of Health consensus panel (23) all recommend patient education concerning sun avoidance and sunscreen use. The American Academy of Family Physicians recommends sun protection for all with increased sun exposure (24). The American College of Preventive Medicine (ACPM) concluded that sun-protective measures (e.g., clothing, hats, opaque sunscreens) are probably effective in reducing skin cancer but that the evidence does not support discussion of sunscreen and sun protection with every patient. ACPM concluded that evidence is insufficient to advise patients that chemical sunscreens protect against malignant melanoma and that their use may actually lead to increased risk (25). Recently, the International Agency for Research on Cancer (IARC), part of the World Health Organization, qualified their recommendation for sunscreen use in ways that address the importance of learning more about potential harms of counseling for sunscreen use as follows: Sunscreens probably prevent squamous-cell carcinoma of the skin when used mainly during unintentional sun exposure. No conclusion can be drawn about the cancer-preventive activity of topical use of sunscreens against basal-cell carcinoma and cutaneous melanoma. Use of sunscreens can extend the duration of intentional sun exposure, such as sunbathing. Such an extension may increase the risk for cutaneous melanoma (26). The Task Force on Community Preventive Services found insufficient evidence to determine the effectiveness of a range of population-based interventions to reduce unprotected UV light exposure and recommended additional research on educational policy approaches, media campaigns, and both health-care setting and community-based interventions (27). References
Box 1 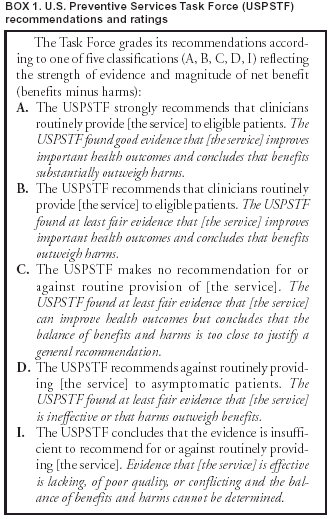 Return to top. Box 2 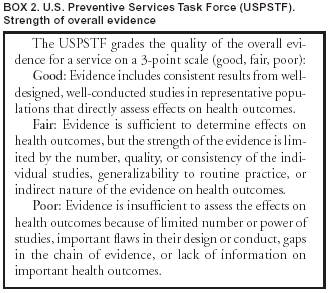 Return to top.
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 10/2/2003 |
|||||||||
This page last reviewed 10/2/2003
|