|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
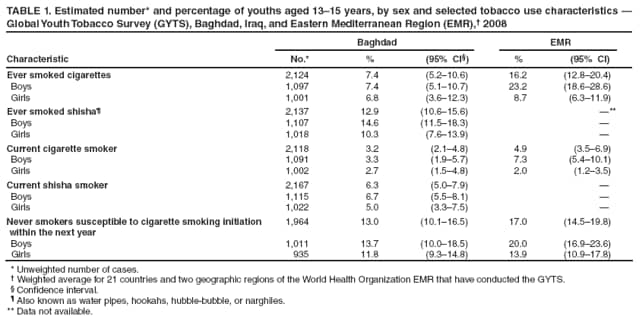
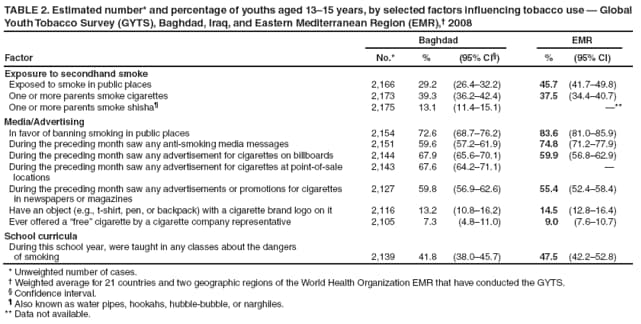
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Tobacco Use Among Students Aged 13--15 Years --- Baghdad, Iraq, 2008In 2008, Iraq's parliament ratified the World Health Organization Framework Convention on Tobacco Control (WHO FCTC) (1), which obligates participants to establish tobacco use monitoring, surveillance, and evaluation systems. Lack of data on adolescent tobacco use in Iraq led the Ministry of Health (MOH) to conduct the Global Youth Tobacco Survey (GYTS) in Baghdad in 2008. GYTS is a school-based survey of students aged 13--15 years that is self-administered in classes in selected schools. As in most Middle East countries, tobacco use in Iraq takes the form of cigarettes and shisha (Figure) (2). Based on GYTS results, 7.4% of students aged 13--15 years reported having ever smoked cigarettes, 12.9% had ever smoked shisha, 3.2% currently smoked cigarettes, and 6.3% currently smoked shisha. Among never smokers aged 13--15 years, 13.0% reported they were likely to initiate cigarette smoking in the next year. Future declines in adolescent tobacco use in Iraq (and Baghdad) could be enhanced by expanding existing tobacco control programs to include prevention and cessation of the use of cigarettes and shisha, implementing measures that discourage adolescents who have never smoked from initiating tobacco use, expanding legislation to ban exposure to secondhand smoke in all indoor workplaces, and enacting legislation banning pro-tobacco advertising and sponsorship. GYTS is a school-based survey developed by WHO, CDC, and the Canadian Public Health Association that collects data on students aged 13--15 years using a standardized methodology for constructing the sample frame, selecting schools and classes, and processing data (3). The Baghdad GYTS used a two-stage cluster sample design that produces representative samples of students in grades intermediate 1--3 and secondary 1, the grades attended by students aged 13--15 years. Schools were selected proportional to the number of students enrolled and the type of school. Classes within the selected schools were selected randomly. All students attending school in the selected classes on the day the survey was administered were eligible to participate. During 2008, the Baghdad Administrative Division included 610 schools and 269,990 students in grades intermediate 1--3 and secondary 1. An estimated 90% of boys remain in school through intermediate grade 3 (S.M. Jasim, Iraq Ministry of Health, personal communication, 2008); however, girls are 40% less likely than boys to be enrolled in intermediate grades, and more than 33% of all students enrolled in intermediate 3 do not continue to secondary 1. A weighting factor was applied to each student record to account for the probability of selection at the school and class levels, adjust for nonresponse (by school, class, and student), and correct for population demographics (3). A total of 2,182 students aged 13--15 years completed the Baghdad 2008 GYTS from 25 selected schools. The school response rate was 100%, the class response rate was 100%, the student response rate was 94.0%, and the overall response rate was 94.0%.* A weighted average of GYTS data from individual surveys conducted in 21 countries and two geographic regions of the Eastern Mediterranean Region (EMR) of WHO was used for comparison. Each GYTS in the 23 EMR sites followed similar sample designs, data collection, and data processing procedures as the Baghdad GYTS. Overall, 7.4% of surveyed students had ever smoked cigarettes, and 12.9% had ever smoked shisha (Table 1). Boys were 97% more likely to have ever smoked shisha than to have ever smoked cigarettes (14.6% versus 7.4%, respectively), whereas girls were 51% more likely to have ever smoked shisha. Current use of shisha was twice that of cigarette smoking for boys (6.7% versus 3.3%) and girls (5.0% versus 2.7%). Overall, 13.0% of never smokers indicated they might initiate cigarette smoking in the next year. For boys and girls, potential initiation of cigarette smoking among never smokers was four times more prevalent than current cigarette smoking. Among surveyed students, 29.2% reported being exposed to smoke in public places during the week preceding the survey, 39.3% reported that their parents smoked cigarettes, 13.1% reported that their parents smoked shisha, and 72.6% were in favor of banning smoking in public places (Table 2). In response to questions regarding advertising, 59.6% of the students reported having seen any anti-cigarette media message during the preceding month; 67.9% had seen pro-cigarette advertising on billboards, 67.6% had seen pro-cigarette advertising at point of sale locations, and 59.8% had seen pro-cigarette advertising in newspapers or magazines. Overall, 13.2% of students reported that they owned an object with a cigarette brand logo on it, and 7.3% reported that they had been offered free cigarettes by a cigarette company representative. With regard to school curricula, 41.8% of students reported having been taught in school during the preceding year about the dangers of smoking. Reported by: SM Jasim, MB ChB, L Kadhim, MB ChB, Ministry of Health, Iraq. F El Awa, PhD, H Fouad, PhD, Eastern Mediterranean Regional Office, World Health Organization, Cairo, Egypt. CW Warren, PhD, J Lee, MPH, V Lea, MPH, A Goding, MSPH, S Asma, DDS, M McKenna, MD, Office on Smoking and Health, National Center for Chronic Disease Prevention and Health Promotion, CDC. Editorial Note:Since March 2003, the government of Iraq has transitioned to the country's first constitutional government in nearly 50 years (4). During this time, most of the governmental focus has been on security and meeting basic population needs such as supplying food, fuel, and shelter. However, during the past 2 years, the MOH has increased emphasis on family life issues, including tobacco control. In March 2008, the MOH made a significant commitment to tobacco control by ratifying the WHO FCTC. The MOH expanded the tobacco control effort in 2008 by developing tobacco-control strategies that include 1) banning smoking in MOH buildings; 2) establishing tobacco-free health institutes in Baghdad and other governorates; 3) collaborating with WHO and the Al-Nahrain medical college in Baghdad to ban smoking in all medical college buildings; 4) initiating the Tobacco Free School Project in 30 primary schools in Baghdad to raise teacher, student, and family awareness about the dangers of tobacco use; and 5) establishing a National Tobacco Control Committee to develop new legislation and regulations regarding tobacco control. The results from the Baghdad GYTS point to a number of challenges facing MOH tobacco control efforts. First, the use of shisha is twice as prevalent as cigarette smoking. Smoking shisha originated in ancient Persia and India, and spread throughout the Middle East and Asia during the 15th century (5,6). In the 21st century, smoking shisha appears to be a new trend in tobacco use and has recently become a preferred form of tobacco smoking for young persons, specifically women, in the Arabian Peninsula (7). For Arab women, shisha smoking carries less of a cultural stigma than does cigarette smoking (5,6). This is a concern because the harmful health effects of shisha can exceed those of cigarette smoking (2). Some reports indicate that the concentration of nicotine is higher from shisha smoking than from cigarette smoking (5,6). Levels of arsenic, chromium, and lead also are higher in shisha smoking compared to single cigarette use. Additionally, because shisha sessions typically last 45--60 minutes, shisha smokers inhale higher concentrations of these toxic substances (5,6). A second concern is that the current cigarette smoking rate for girls (2.7%) is twice that for adult female cigarette smokers in Iraq (8). In addition, the likely initiation of cigarette smoking by girls who have never smoked cigarettes (11.8%) is significantly higher than the current cigarette smoking rate for girls (2.7%). These findings might indicate that girls' cigarette use is increasing, which, if the trend continues, will lead to an increase in the burden of disease caused by tobacco use in Iraq. A very different pattern is found for boys aged 13--15 years in the Baghdad GYTS. The prevalence of cigarette smoking for boys (3.3%) is much lower than for adult males (25.2%) in Iraq (8), but the likely initiation of smoking by boys (13.7%) is approximately half the adult smoking rate. This pattern was found throughout the EMR and suggests the smoking behavior of males dramatically increases at some point beyond age 15 years (3). Overall, current cigarette smoking in Baghdad (3.2%) is similar to that of the 21 WHO member states of the EMR (4.9%). Current smoking among boys in Baghdad (3.3%) is lower than the rate (7.3%) for the region, but the rate for girls is similar (2.7% and 2.0%, respectively). Data on shisha smoking by adolescents in the EMR are not available. The findings in this report are subject to at least four limitations. First, because the sample surveyed was limited to youths attending school, it is not representative of all youths aged 13--15 years. Second, the findings apply only to youths who were in school on the day the survey was administered and who completed the survey. However, student response was high (94.0%), suggesting that bias attributed to absence or nonresponse was minimal. Third, data are based on self-reports of students, who might have underreported or overreported their tobacco use or that of their parents. The extent of this bias cannot be determined; however, responses to tobacco-related questions in surveys similar to GYTS in the United States have shown good test-retest reliability (9). Finally, the Baghdad GYTS did not include detailed questions on shisha, including specific questions on advertising and media, knowledge and attitudes concerning the health effects of shisha use, the likelihood of never shisha users to initiate shisha use, and the desire to stop using shisha. Future surveys need to add questions on these topics to gain a better understanding of the use of shisha. By ratifying the WHO FCTC, the MOH of Iraq has obligated the government to develop a comprehensive tobacco control program. WHO has identified six policy areas that countries should include in their tobacco control programs to maximize effect: 1) raising taxes on tobacco; 2) banning advertising promotion and sponsorship; 3) reducing exposure to secondhand smoke; 4) establishing tobacco cessation programs; 5) informing the public regarding the dangers of tobacco; and 6) establishing surveillance programs aimed at monitoring tobacco use and policies (8). During 2008, the MOH expanded tobacco control effort in Iraq and adopted some of the tenants of these policies by developing several tobacco control strategies in addition to conducting the GYTS. The MOH will need to further expand its tobacco control efforts to meet the goals WHO has established in each of the six policy areas. Future surveys can be used to monitor and evaluate the programs implemented to meet those goals and obligations. References
* The overall response rate was calculated as the school response rate × the class response rate × the student response rate. Table 1
All MMWR HTML versions of articles are electronic conversions from typeset documents. This conversion might result in character translation or format errors in the HTML version. Users are referred to the electronic PDF version (http://www.cdc.gov/mmwr) and/or the original MMWR paper copy for printable versions of official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Date last reviewed: 4/2/2009 |
|||||||||
|