|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
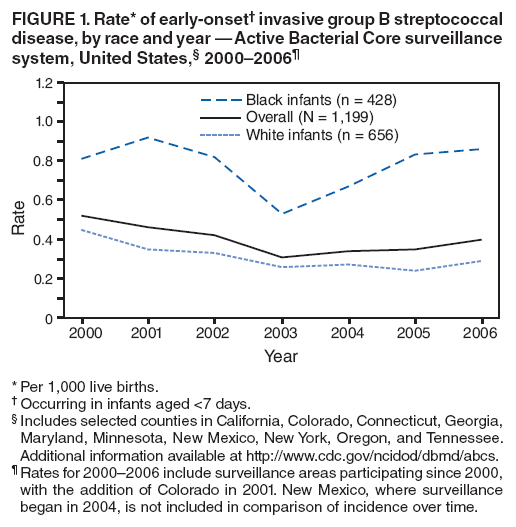
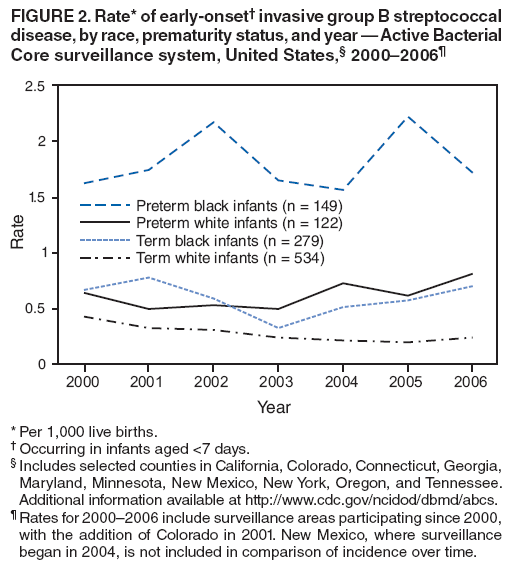
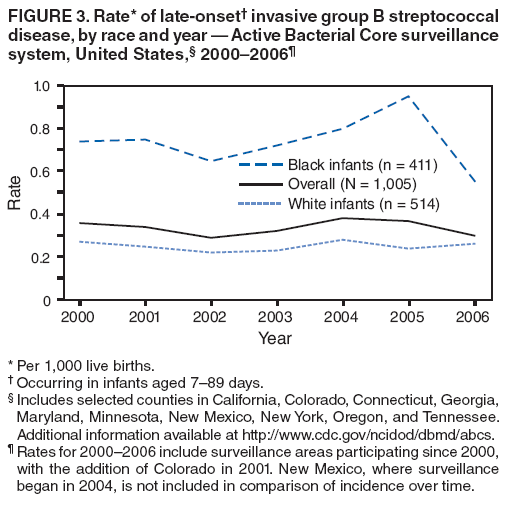
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Trends in Perinatal Group B Streptococcal Disease --- United States, 2000--2006Group B Streptococcus (GBS) is a leading infectious cause of neonatal morbidity and mortality in the United States (1). The bacterium, a common colonizer of the maternal genital tract, can infect the fetus during gestation, causing fetal death. GBS also can be acquired by the fetus during passage through the birth canal or after delivery. Infection commonly manifests as meningitis, pneumonia, or sepsis. In 2002, CDC, the American College of Obstetricians and Gynecologists, and the American Academy of Pediatrics issued revised guidelines for prevention of early-onset GBS disease (i.e., in infants aged <7 days) (2). These guidelines recommended universal screening of all pregnant women for rectovaginal GBS colonization at 35--37 weeks' gestation and administration of intrapartum antibiotic prophylaxis (IAP) to carriers. A report published in 2007 indicated that, during 2003--2005, the overall rate of early-onset GBS disease increased, whereas incidence of late-onset GBS disease (i.e., in infants aged 7--89 days) remained stable (3). This report updates the 2007 report by incorporating 2006 data from the Active Bacterial Core surveillance (ABCs) system. The updated analysis revealed an increase in the overall rate of early-onset GBS disease from 2003 to 2006, driven by an increasing incidence among black term infants. Late-onset GBS disease incidence among black infants, which had increased during 2003--2005, declined in 2006. Continued monitoring is needed to follow trends in early-onset GBS disease among black infants to determine whether additional interventions are warranted. ABCs conducts active, population- and laboratory-based surveillance for all cases of invasive GBS disease in selected counties of 10 states.* GBS cases are identified through regular contact with laboratories and are defined as isolation of GBS from a normally sterile body site (e.g., blood or cerebrospinal fluid) or from the placenta or amniotic fluid in cases of fetal death. In 2005, the areas covered by ABCs represented approximately 450,000 live births (11% of U.S. live births); 70% of infants were white, 20% were black, and 10% were of other race. Surveillance areas used standardized case-report forms to collect demographic, neonatal, and obstetric data from medical records. Race and ethnicity were determined from medical records or birth certificates. Multiple imputation procedures were used to address missing data for race and gestational age (4). Live-birth data from state vital records and national vital statistics reports for each respective year other than 2006 were used as denominators for incidence calculations; incidence for 2006 was calculated using 2005 natality data. The Cochran-Armitage test was conducted to determine linear trend significance. The number of surveillance areas changed slightly during 2000--2006 because of the addition of Colorado in 2001 and New Mexico in 2004; New Mexico cases were not included in evaluations of incidence over time. Because the most notable incidence differences have been associated with race rather than ethnicity (5), the trend analyses described in this report focus on race. During 2000--2006, a total of 1,199 early-onset disease (EOD) and 1,005 late-onset disease (LOD) cases were reported. In 2006, 316 cases were reported (179 EOD and 137 LOD). Of these, 178 (56%) were in white infants, 118 (37%) were in black infants, 14 (4%) were in infants of other races, and six (3%) were in infants of unknown race; 52 (16%) were in Hispanic infants, 246 (78%) were in non-Hispanic infants, and 18 (6%) were in infants of unknown ethnicity. Among cases in 2006 for which outcome information was available (n = 313), the case-fatality ratio was 7% for EOD (13 of 177) and 5% (seven of 136) for LOD. Among cases for which gestational age was available (312 of 316), 28% (49 of 178) of EOD cases were in infants born preterm (gestational age <37 weeks), and 42% (56 of 134) of LOD cases were in infants born preterm. The overall EOD incidence rate showed an initial downward trend from 2000 to 2003 (0.52 to 0.31 cases per 1,000 live births), followed by an increase from 2003 to 2006 (0.31 to 0.40 cases per 1,000 live births; p=0.03). When stratified by race, incidence from 2003 to 2006 among black infants increased significantly (0.53 to 0.86 cases per 1,000 live births; p=0.005), whereas incidence among white infants did not change significantly (0.26 to 0.29 cases per 1,000 live births; p=0.64) (Figure 1). When EOD incidence was stratified by gestational age, the average incidence among preterm infants during 2003--2006 was 2.8 times higher among black infants (1.79 cases per 1,000 live births) compared with white infants (0.67 cases per 1,000 live births) (Figure 2). Both preterm black and white infants had increases in EOD incidence from 2003 to 2006 that were not significant (p=0.61 and 0.21, respectively). EOD incidence among term white infants was stable during 2003--2006. Term black infants were the only group with a significant increase in incidence from 2003 to 2006 (0.33 to 0.70 cases per 1,000 live births; p=0.002). Overall, 93% (549 of 593) of EOD cases from 2003 (the first full year after the universal screening recommendations) through 2006 had information available on prenatal GBS screening. Among these, 387 (70%) mothers were screened at least 2 days before the infant's birth. Among EOD cases in infants delivered at term (395 of 549), a similar proportion of mothers of black and white infants were screened (83% in each group). IAP was administered to 80 (20%) mothers of term infants with EOD during 2003--2006 (16% of black mothers and 23% of white mothers; p=0.09). The overall rates of LOD remained stable from 2000 (0.36 cases per 1,000 live births) to 2006 (0.30 cases per 1,000 live births). In addition, no overall incidence trend was observed from 2003 to 2006 (p=0.7). When stratified by race, LOD incidence among black infants decreased significantly by 42% (p=0.003) from 2005 (0.95 cases per 1,000 live births) to 2006 (0.55 cases per 1,000 live births) (Figure 3). However, no significant trend was observed among black or white infants from 2003 to 2006. Reported by: M Apostol, MPH, Emerging Infections Program, California Dept of Public Health. K Gershman, MD, Colorado Dept of Public Health. S Petit, MPH, Emerging Infections Program, Connecticut Dept of Public Health. K Arnold, MD, Emerging Infections Program, Div of Public Health, Georgia Dept of Human Resources. L Harrison, MD, Maryland Emerging Infections Program. R Lynfield, MD, Minnesota Dept of Health. C Morin, MPH, Minnesota Dept of Health. J Baumbach, MD, New Mexico Dept of Health. S Zansky, PhD, New York State Dept of Health. A Thomas, MD, Oregon Public Health Div. W Schaffner, MD, Vanderbilt Univ School of Medicine. SJ Schrag, DPhil, ER Zell, MStat, MM Lewis, MPH, Div of Bacterial Diseases, National Center for Immunization and Respiratory Diseases; RD Muhammad, MD, EIS Officer, CDC. Editorial Note:GBS emerged as a major cause of neonatal bacterial sepsis in the 1970s. Before the 2002 guidelines recommending universal screening, existing CDC guidelines allowed a choice of two strategies to determine candidates for IAP: 1) monitoring for certain risk factors (risk-based screening) during labor (e.g., preterm delivery or prolonged membrane rupture), or 2) late antenatal culture-based screening for GBS colonization (6). A 2002 population-based study showed that culture-based screening was >50% more effective than risk-based screening (7), and led to the 2002 recommendation for universal, culture-based screening. Implementation of universal screening was expected to result in a 30% further decline in the incidence of EOD, with the most dramatic reductions anticipated among term infants, because screening is performed during 35--37 weeks of gestation. In addition, the transition to a single prevention strategy was expected to reduce racial differences in EOD incidence. Universal screening was not anticipated to affect LOD incidence or racial differences because implementation of IAP had not been associated with LOD prevention (8). The results described in this report indicate an increase in EOD from 2003 to 2006,† and this increase has been driven by increasing incidence among black term infants. This increase was not anticipated and cannot yet be explained fully. The increase in EOD since 2003 was not accompanied by a significant change in the overall incidence rate for LOD. Because EOD incidence trends do not match LOD incidence trends, their shared live-birth denominator is not likely to contribute error to the worsening EOD rates. Also, racial differences in screening do not appear to be a likely cause of the increasing incidence trend among black term infants, because a similar and high proportion of mothers of both black and white case-infants delivered at term were screened. Consistent with this, a recent evaluation of live births during 2003--2004 in the ABCs catchment population found that black race was not associated with lack of screening (9). Additionally, IAP was administered to a similar proportion of black and white mothers of term infants with EOD. The overall proportion receiving IAP (20%) was low, suggesting that missed opportunities for prevention might contribute more than prophylaxis failures to the remaining EOD burden. However, data on screening result often were incomplete, limiting the ability to determine whether lack of IAP administration represented poor adherence to recommendations. Moreover, in the context of a widely implemented prevention strategy, population-based data rather than case-only data provide the most useful guide to assessing guidelines implementation. Other factors might influence the effectiveness of prevention and thus rates of disease, including higher GBS carriage rates among black women (10), the timing of screening, adequacy of specimen collection, appropriate laboratory processing, and implementation of adequate IAP (2). Evaluation of these factors will be important in determining whether the causes of increasing racial differences in EOD can be directly linked to missed opportunities for prevention. The findings in this report are subject to at least three limitations. First, although surveillance data can help describe and monitor racial differences in diseases, often they cannot explain why these differences exist. Unidentified risk factors for which race is a proxy might explain the differences. For example, ABCs includes limited information on cases and does not collect variables related to socioeconomic status. Second, select counties in 10 states are covered by ABCs. As a result, rates might not be representative of the entire United States. Finally, these findings represent only 4 years of data since 2002, and additional surveillance is needed to confirm whether the increasing trend will continue. Since efforts to prevent GBS disease became widespread in the 1990s, the United States has experienced an 80% decline in EOD incidence (8). Despite the increases in EOD rates after 2003, antenatal screening remains the most effective strategy available (7). Within the next year, CDC will work with the American Academy of Pediatrics, the American College of Obstetricians and Gynecologists, and other partners to update the perinatal GBS disease prevention guidelines. This update will focus on both the laboratory and clinical components of the guidelines and will be based on data accumulated since 2002, including licensure of polymerase chain reaction--based rapid tests for GBS and a population-based review of approximately 8,000 labor and delivery records of births in 2003 and 2004 in the ABCs population (9). Information for patients, health-care providers, and public health practitioners regarding GBS is available from CDC at http://www.cdc.gov/groupbstrep. Brochures are available in both English and Spanish by telephone (404-639-2215); information regarding bulk orders is available through the CDC Foundation by telephone (877-252-1200). Acknowledgments This report is based, in part, on contributions by P Daily, MPH, Emerging Infections Program, California Dept of Public Health; D Aragon, S Burnite, and A Daniels, Colorado Dept of Public Health; Z Fraser and JL Hadler, MD, Emerging Infections Program, Connecticut Dept of Public Health; MM Farley, MD, W Baughman, MSPH, P Malpiedi, MPH, P Martell-Cleary, MSW, S Bulens, MPH, and L Lorentzson, Emerging Infections Program, Div of Public Health, Georgia Dept of Human Resources; RA Hollick, MS, KD Holmes, MS, and E Vaeth, Maryland Active Bacterial Core Surveillance, Johns Hopkins Bloomberg School of Public Health; R Danila, PhD, B Jewell, J Rainbow, MPH, and L Triden, Minnesota Dept of Health; K Angeles, MPH, L Butler, MSN, J Keefe, MPH, and E Racz, MPH, New Mexico Dept of Health; G Smith and N Spina, MPH, Emerging Infections Program, New York State Dept of Health; K Stefonek, MPH, Oregon Public Health Div; B Barnes, Vanderbilt Univ School of Medicine; and TH Skoff, MS, E Weston, MPH, and C Wright, Div of Bacterial Diseases, National Center for Immunization and Respiratory Diseases, CDC. References
* California, Colorado, Connecticut, Georgia, Maryland, Minnesota, New Mexico, New York, Oregon, and Tennessee. Additional information available at http://www.cdc.gov/ncidod/dbmd/abcs. † The analysis in this report differs from the previous one (3) in that values were imputed for both race and gestational age to account for missing data, allowing all the observed cases to contribute to estimates of stratified rates and improving the robustness of the rates reported. Figure 1
All MMWR HTML versions of articles are electronic conversions from typeset documents. This conversion might result in character translation or format errors in the HTML version. Users are referred to the electronic PDF version (http://www.cdc.gov/mmwr) and/or the original MMWR paper copy for printable versions of official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Date last reviewed: 2/12/2009 |
|||||||||
|