 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Progress in Global Measles Control and Mortality Reduction, 2000--2007Despite the availability of a safe and effective vaccine since 1963, measles has been a major killer of children in developing countries (causing an estimated 750,000 deaths as recently as 2000), primarily because of underutilization of the vaccine (1). At the World Health Assembly in 2008, all World Health Organization (WHO) member states reaffirmed their commitment to achieving a 90% reduction in measles mortality by 2010 compared with 2000, a goal that was established in 2005 as part of the Global Immunization Vision and Strategy (2). This WHO-UNICEF comprehensive strategy for measles mortality reduction (1) focuses on 47 priority countries.* The strategy's components include 1) achieving and maintaining high coverage (>90%) with the routinely scheduled first dose of measles-containing vaccine (MCV1) among children aged 1 year; 2) ensuring that all children receive a second opportunity for measles immunization (either through a second routine dose or through periodic supplementary immunization activities [SIAs]†); 3) implementing effective laboratory-supported disease surveillance; and 4) providing appropriate clinical management for measles cases. This report updates previously published reports (3,4) and describes immunization and surveillance activities implemented during 2007. Increased routine measles vaccine coverage and SIAs implemented during 2000--2007 resulted in a 74% decrease in the estimated number of measles deaths globally. An estimated 197,000 deaths from measles occurred in 2007; of these, 136,000 (69%) occurred in the WHO South-East Asian Region. Achievement of the 2010 goal will require full implementation of measles mortality reduction strategies, especially in the WHO South-East Asian Region. Immunization ActivitiesWHO and UNICEF use data from administrative records and surveys to estimate routine MCV1 coverage among children aged 1 year (5). Coverage levels achieved during measles SIAs are estimated using the reported number of doses administered and dividing by the target population. According to WHO and UNICEF estimates, global routine MCV1 coverage has continued to improve steadily since 2000, reaching 82% in 2007; however, coverage has varied substantially by geographic region (Table 1). Of 23.3 million infants in 2007 who missed receiving their first dose of measles vaccine through routine immunization services by the age of 1 year, 15.2 million (65%) resided in eight highly populated countries: India (8.5 million children), Nigeria (2.0 million), China (1.0 million), Ethiopia (1.0 million), Indonesia (0.9 million), Pakistan (0.8 million), the Democratic Republic of the Congo (0.6 million), and Bangladesh (0.5 million) During 2000--2007, a second opportunity§ for measles immunization was provided in the 47 priority countries to approximately 576 million children aged 9 months--14 years through SIAs. In 2007, 20 (43%) of these 47 countries conducted SIAs, reaching approximately 91 million children; 16 (80%) of these SIAs integrated at least one other child-survival intervention (e.g., insecticide-treated bed nets, vitamin A supplements, and deworming medication) (Table 2). Surveillance ActivitiesEffective surveillance for measles entails establishing case-based surveillance that includes case investigation and laboratory testing of samples from all suspected measles cases (6).¶ In 2007, 162 (84%) of the 193 WHO member states had implemented case-based surveillance, compared with 120 (62%) countries in 2004 (the first year for which data are available). In 2007, 178 countries (92%), compared with 168 countries (88%) in 2000, reported measles surveillance data to WHO and UNICEF through the annual Joint Reporting Form. Worldwide, the number of reported measles cases decreased from 852,937 in 2000 to 279,006 in 2007 (a 67% decrease). All regions reported a decrease in reported measles cases, with the highest percentage reduction occurring in the Americas** and the African regions (93% and 85%, respectively), and the lowest in the South-East Asian Region (12%). The WHO measles and rubella laboratory network, which in 1998 consisted of fewer than 40 laboratories, by the end of 2007 had expanded to 679 national and subnational laboratories providing support for measles and rubella surveillance in 164 countries. Mortality Estimates for 2007Despite the progress made on measles surveillance and reporting globally, measles incidence remains underreported, and complete and reliable surveillance data on the number of measles deaths are lacking for many countries, particularly those with the highest disease burden. To estimate measles mortality, WHO used the published natural history model (7) and updated it with 1) the most recent time-series of population data (8), 2) WHO-UNICEF routine immunization coverage estimates and reported coverage of SIAs, and 3) measles incidence as reported to WHO. This process produced the 2007 mortality estimates and permitted updating of previous estimates for 2000--2006. During 2000--2007, global mortality attributed to measles was reduced by 74%, from an estimated 750,000 deaths in 2000 to 197,000 deaths in 2007 (Table 1, Figure). Approximately 90% of estimated measles deaths occurred among children aged <5 years: 679,000 (95% uncertainty interval: 490,000--890,000) in 2000 and 177,000 (126,000--240,000) in 2007. The largest regional percentage reduction in estimated measles mortality during 2000--2007 occurred in the Eastern Mediterranean (90%) and African (89%) regions, accounting for 16% and 63% of the global reduction in measles mortality, respectively. The 47 priority countries accounted for 98% of the total estimated number of deaths globally in 2007, whereas the reduction in measles deaths among these countries accounted for 96% of the global reduction in measles deaths during 2000--2007. During 2000--2007, approximately 11 million measles deaths worldwide were averted because of measles control activities; of these, an estimated 3.6 million deaths (33%) were averted as a result of accelerated activities (i.e., increases in routine vaccination coverage and implementation of measles SIAs). Reported by: A Dabbagh, PhD, M Gacic-Dobo, D Featherstone, PhD, P Strebel, MBChB, JM Okwo-Bele, MD, Dept of Immunization, Vaccines, and Biologicals, World Health Organization, Geneva, Switzerland. E Hoekstra, MD, P Salama, MD, United Nations Children's Fund, New York, New York. A Uzicanin, MD, Global Immunization Div, National Center for Immunization and Respiratory Diseases, CDC. Editorial Note:During 2007, further progress was made toward achieving the 2010 global measles mortality reduction goal of a 90% reduction in measles mortality compared with 2000. Increased MCV1 coverage, together with the accelerated efforts to vaccinate children through SIAs during 2000--2007, resulted in a 74% decrease in the estimated number of measles deaths globally during this period. The largest percentage decrease in estimated measles deaths occurred in the Eastern Mediterranean Region, which appears to have already met the 2010 goal. An important contributor to the rapid reduction in measles mortality in the Eastern Mediterranean Region during 2007 is the intensification of SIAs in the region, which resulted in more than twice the number of children reached through SIAs in 2007 compared with 2006. The African Region was the largest contributor to the global decline in measles mortality, accounting for 63% of the decline. However, a number of countries have experienced outbreaks of more than 1,000 cases in 2007 (e.g., the Democratic Republic of Congo, Nigeria, Uganda, and Tanzania) because of gaps in MCV1 coverage and children missed during SIAs. The reduction in the South-East Asian Region was substantially smaller because India, which alone accounts for 67% of the region's population, has not yet begun large-scale measles SIAs. The number of reported measles cases also declined by approximately two thirds worldwide during 2000--2007. However, direct comparisons between trends in estimated deaths and trends in reported cases should be made with caution because the static model used to estimate deaths does account for the cyclical nature of measles (7). Furthermore, measles incidence is grossly underreported, and the mathematical model used to estimate global measles mortality adjusts for underreporting of cases (7). The prevention of an estimated 3.6 million additional deaths during 2000--2007 because of accelerated measles control activities highlights the potential future benefits of continuing the ongoing efforts of the Measles Initiative†† and international partners (e.g., the GAVI Alliance and the International Finance Facility for Immunization) to support country efforts to strengthen routine immunization and implementation of SIAs. In addition to the primary objective, measles SIAs provide the platform for delivery of other child survival interventions, which attracts high-level political support, allows for resources to be pooled, and increases community participation (9). As countries with high measles disease burden approach the Global Immunization Vision and Strategy goal of a 90% reduction in global measles mortality by 2010, major challenges should be addressed. First, accelerated measles mortality reduction activities (e.g., SIAs coupled with further efforts to improve routine MCV1 coverage) need to be successfully implemented in the South-East Asian Region, especially in India, which contributes substantially to the global burden of measles. Second, to sustain the current reduction in measles deaths, vaccination systems need to be improved to ensure that >90% of infants receive their MCV1 on schedule. Third, countries need to monitor accumulation of susceptible children (by evaluating routine MCV1 and SIA coverage data by birth cohort) and conduct follow-up SIAs when the number of susceptible children approaches the size of a birth cohort. Fourth, disease surveillance systems need to be strengthened at all levels to enable case-based surveillance with testing of clinical specimens from all suspected cases. Fifth, measles case management should be improved (e.g., by including use of vitamin A). Finally, further efforts are needed to ensure sustainability of measles control activities. Recent shortfalls in the donor funds available to support measles mortality reduction activities (10) make increased country responsibility and political commitment critical for both achieving and sustaining the goal of a 90% measles mortality reduction by 2010. References
* Afghanistan, Angola, Bangladesh, Benin, Burkina Faso, Burundi, Cambodia, Cameroon, Central African Republic, Chad, Côte d'Ivoire, Democratic Republic of the Congo, Djibouti, Equatorial Guinea, Eritrea, Ethiopia, Gabon, Ghana, Guinea, Guinea-Bissau, India, Indonesia, Kenya, Laos, Liberia, Madagascar, Mali, Mozambique, Myanmar, Nepal, Niger, Nigeria, Pakistan, Papua New Guinea, Republic of the Congo, Rwanda, Senegal, Sierra Leone, Somalia, Sudan, Timor-Leste, Togo, Uganda, Tanzania, Vietnam, Yemen, and Zambia. † SIAs generally are carried out using two approaches. An initial, nationwide catch-up SIA targets all children aged 9 months--14 years; it has the goal of eliminating susceptibility to measles in the general population. Periodic follow-up SIAs then target all children born since the last SIA. Follow-up SIAs generally are conducted nationwide every 2--4 years and target children aged 9--59 months; their goal is to eliminate any measles susceptibility that has developed in recent birth cohorts and to protect children who did not respond to the first measles vaccination. § Second opportunity for immunization is provided to all children, including those who were not reached with MCV1 and those who were previously vaccinated (because approximately 15% of children vaccinated with a single dose at age 9 months will fail to develop immunity to measles). ¶ Case-based surveillance includes investigation of every suspected measles case and routine reporting of detailed epidemiologic and laboratory data for each confirmed measles case. ** The Region of the Americas interrupted indigenous measles transmission in November 2002; cases reported since 2002 are imported or linked to importation. †† The Measles Initiative comprises the American Red Cross, CDC, the United Nations Foundation, UNICEF, and WHO. Figure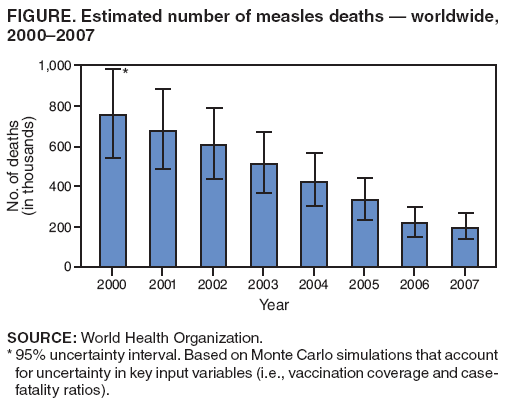 Return to top. Table 1 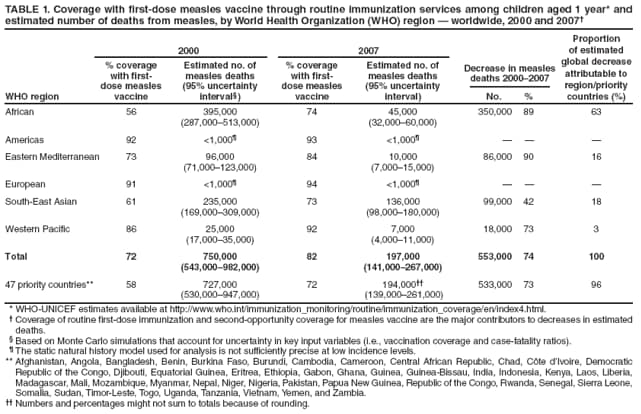 Return to top. Table 2 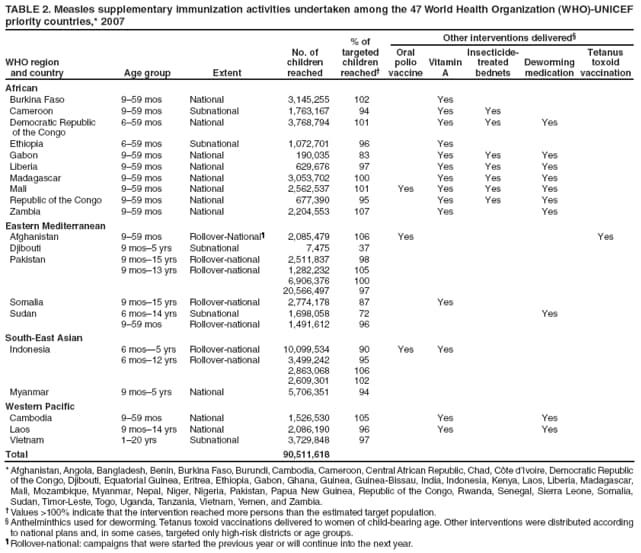 Return to top.
All MMWR HTML versions of articles are electronic conversions from typeset documents. This conversion might result in character translation or format errors in the HTML version. Users are referred to the electronic PDF version (http://www.cdc.gov/mmwr) and/or the original MMWR paper copy for printable versions of official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Date last reviewed: 12/3/2008 |
|||||||||
|