|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
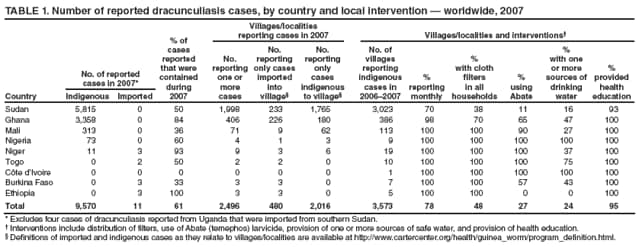
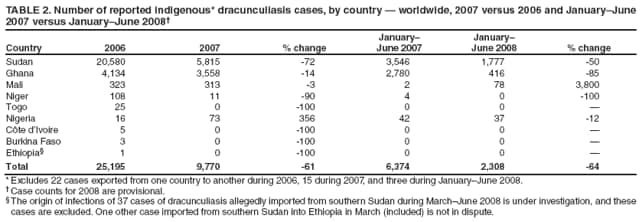
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Update: Progress Toward Global Eradication of Dracunculiasis, January 2007--June 2008The World Health Assembly (WHA) first adopted a resolution calling for the eradication of dracunculiasis (Guinea worm disease) in 1986, when an estimated 3.5 million cases occurred annually in 20 countries (17 in Africa and three in Asia) and 120 million persons were at risk for the disease (1,2). Because of slow mobilization in countries with endemic disease, the global dracunculiasis eradication program did not meet the 1995 target date for eradicating dracunculiasis that was set by African ministers of health in 1988 and confirmed by WHA in 1991 (3). In 2004, WHA established a new target date of 2009 (4). This report updates the progress of the global dracunculiasis eradication program since January 2007 (5,6). At the end of December 2007, dracunculiasis remained endemic only in Sudan, Ghana, Mali, Nigeria, and Niger. During 2007, a total of 9,585 cases were reported worldwide from 3,573 villages with endemic disease, including 15 cases exported from one country to another (Table 1). From 2006 to 2007, the number of indigenous cases decreased by 61% (from 25,195 to 9,770). Of the 2,308 cases occurring during January--June 2008, 98% were reported from Sudan, Ghana, and Mali (Table 2). Sporadic violence in areas with endemic dracunculiasis in Sudan and Mali is a major concern and poses the greatest challenge to the success of the global dracunculiasis eradication program. Dracunculiasis can be prevented by 1) filtering drinking water through a finely woven cloth, 2) treating contaminated water with Abate (temephos) larvicide, 3) providing clean water from borehole or hand-dug wells, and 4) educating persons to avoid entering water sources when Guinea worms are emerging from their bodies, thereby preventing contamination of water sources. Containment of transmission, achieved through voluntary isolation of each patient, provision of first aid, manual extraction of the emerging worm, and applying occlusive bandages, is a complementary component to the four main interventions.* Countries enter the World Health Organization (WHO) precertification stage of eradication approximately 1 year after reporting the last indigenous case (approximately one incubation period for Dracunculus medinensis).† Nine countries where dracunculiasis was formerly endemic (Benin, Burkina Faso, Chad, Côte d'Ivoire, Ethiopia, Mauritania, Kenya, Togo, and Uganda) are in the precertification stage of eradication. WHO already has certified 180 countries and territories as dracunculiasis-free; Cambodia and 20 African countries remain to be certified. In each country affected by dracunculiasis, a national Guinea worm eradication program receives monthly reports of dracunculiasis§ from every village with endemic transmission. Reporting rates are calculated by dividing the number of villages with endemic dracunculiasis reporting each month by the total number of reports expected each month from all villages with endemic disease. All villages where endemic transmission transmission of dracunculiasis is stopped are kept under active surveillance and response for 3 consecutive years. Country ReportsSudan. The last indigenous case of dracunculiasis in northern Sudan occurred in 2001, and all subsequent reported cases have occurred in southern Sudan. The civil war in Sudan ended in 2005, and the Southern Sudan Guinea Worm Eradication Program was created in 2006. Access to areas of southern Sudan that had been inaccessible during the civil war resulted in the discovery of a large number of previously unreported cases. Reported cases increased 179% from 2005 to 2006, from 5,569 cases in 1,293 villages to 15,539 cases in 3,345 villages. In 2007, the number of reported cases decreased by 63% (to 5,815), and the reporting rate increased to 70% (from 63% in 2006). Of the 5,815 cases reported in 2007, 49% were contained. In January--June 2008, the number of reported cases decreased by 50% (to 1,777), and the rate of reporting increased to 85%. The Southern Sudan Guinea Worm Eradication Program has approximately 28,000 village volunteers and health staff members working in the program. Ghana. Ghana's Guinea worm eradication program reported 26% fewer cases in 2007 compared with 2006, with cases decreasing from 4,134 in 606 villages in 2006 to 3,358 cases in 406 villages in 2007. A surge in cases occurred during October 2006--March 2007, when municipal water supplies were disrupted in the northern region's capital city of Tamale and in the nearby town of Savelugu. During January--June 2008, the number of reported cases decreased by 86%, compared with the same period in 2007 (Table 2). Mali. In 2006, Mali had an unexpected outbreak in the previously dracunculiasis-free region of Kidal, after an infected person from another Malian village where dracunculiasis was endemic contaminated a water source. This outbreak was reported 2 months after it was detected. Mali's Guinea worm eradication program began interventions in August 2007 but could not gain access to the affected area during September--December 2007 because of insecurity. As a result of this and two smaller outbreaks discovered in Ansongo District, Gao Region (when Niger notified Mali regarding cases exported from Mali to Niger), the number of cases reported in Mali decreased by only 3% from 2006 (323 cases) to 2007 (313 cases). During January--June 2008, 78 cases were reported, compared with two cases for the same period in 2007. Nigeria. Nigeria reported 16 cases during 2006 (69% of which were contained), compared with 73 cases (60% of which were contained) in 2007, amounting to an increase of 356% (Table 2). All 73 of the cases in 2007 were from one outbreak in a village that had never experienced endemic dracunculiasis. During January--June 2008, Nigeria reported 37 cases (100% of which were contained), compared with 42 cases (40% of which were contained) reported during the same period in 2007, amounting to a decrease of 12%. Nigeria has reported no cases since March 2008. Niger. In 2006, a total of 108 indigenous cases were reported in Niger. In 2007, this number decreased by 90% to 11 indigenous cases. In addition, Niger reported three imported cases in 2007. Since 2007, Niger has reported one imported case, which was contained in February 2008, and no indigenous cases. Ethiopia. Before 2008, the most recent indigenous case of dracunculiasis reported in Ethiopia had occurred in June 2006 in Awukoy village of Gambella Region. However, during March--June 2008, 37 new indigenous cases were reported, of which 31 were contained. All but one or two of the cases were in persons who reportedly traveled to Pochalla County in southern Sudan in early 2007, where they allegedly became infected. Most of the patients were ethnic Agnuak farmers, who lived on both sides of the Ethiopia-Sudan border and crossed the border frequently. However, an investigation by the Southern Sudan Guinea Worm Eradication Program did not confirm endemic dracunculiasis in Pochalla County in 2007, and a team from WHO that visited the Gambella region in May 2008 reported that two of the patients interviewed said they did not travel to Sudan in 2007. Having reported no dracunculiasis for the past decade, Pochalla County was presumed to be free of endemic dracunculiasis and has had no formal surveillance for dracunculiasis except for questioning conducted during polio immunization days. The investigation is ongoing. Reported by: DR Hopkins, MD, E Ruiz-Tiben, PhD, The Carter Center, Atlanta, Georgia. ML Eberhard, S Roy, Div of Parasitic Diseases, National Center for Zoonotic, Vector-Borne, and Enteric Diseases, CDC. Editorial Note:Dracunculiasis is a parasitic infection caused by D. medinensis. Persons become infected by drinking water from stagnant sources (e.g., ponds, open wells, or pools) contaminated by copepods (water fleas) that contain immature forms of the parasite. After 1 year of development within the host's body, adult worms approximately 1 meter (39.4 inches) long emerge through skin lesions, usually on the lower limbs. These lesions frequently develop severe secondary bacterial infections. No effective antiparasitic drug or vaccine for dracunculiasis exists, and infected persons do not become immune to the parasite. The emergent Guinea worm is removed manually by rolling it on a stick or roll of gauze a few centimeters each day. Disabilities caused by dracunculiasis during the emergence of the worm are related to the invasion of bacteria that invade the skin lesion and aggravate the pain, swelling, and cellulitis along the worm tract (7,8). The global campaign to eradicate dracunculiasis now has the support of all countries where the disease remains endemic, in addition to a large coalition of agencies, foundations, governments, and nongovernmental organizations. The major partners, apart from the ministries of health of the endemic countries, are the Carter Center, CDC, UNICEF, and WHO. At the end of December 2007, dracunculiasis remained endemic only in Sudan, Ghana, Mali, Nigeria, and Niger. Niger and Nigeria might have interrupted all transmission of dracunculiasis, although that cannot be known until at least one full incubation period for D. mednienesis has elapsed (i.e., late 2008 for Niger and early 2009 for Nigeria). In Mali, sporadic violence in the newly endemic area is the main residual concern. After several years of delay, Ghana also now appears to be well under way toward stopping transmission. Despite its recent substantial progress, southern Sudan likely will harbor the last cases of dracunculiasis in the world, given the large number of cases still occurring, the sporadic insecurity that still occurs in some areas, and the uncertainty about future political developments. The success of the 15 countries that have already stopped transmission of dracunculiasis has depended on adequate coverage and quality of surveillance, careful analysis of and rapid response to surveillance data, active supervision, effectiveness of implementation, and adequate political, financial, and technical assistance from national governments and partner organizations. Uganda's Guinea worm eradication program exemplifies this success (9). Eradication of dracunculiasis will mark the first worldwide elimination of a parasitic disease and the first time a disease will have been eradicated without benefit of a vaccine. Establishment of adequate surveillance for dracunculiasis in countries and areas that are dracunculiasis-free or that appear to have recently interrupted transmission is a high priority for the countries and for WHO, which is responsible for eventual certification of eradication. References
* Transmission from a patient with dracunculiasis is contained if all of the following conditions are met: 1) the disease is detected before or within 24 hours of worm emergence; 2) the patient has not entered any water source since the worm emerged; 3) a volunteer has managed the patient properly, by cleaning and bandaging the lesion until the worm is fully removed manually and by providing health education to discourage the patient from contaminating any water source (if two or more emerging worms are present, the case is not contained until the last worm is pulled out); and 4) the containment process, including verification of dracunculiasis, is validated by a supervisor within 7 days of emergence of the worm. † Certification of a country as "free of dracunculiasis" requires at least a 3-year period after the last known indigenous case is reported, during which adequate surveillance and response to alleged cases of dracunculiasis must be maintained. § A case of dracunculiasis is defined as disease in a person exhibiting a skin lesion or lesions with emergence of one or more Guinea worms (each person should be counted only once in a calendar year). Table 1
All MMWR HTML versions of articles are electronic conversions from typeset documents. This conversion might result in character translation or format errors in the HTML version. Users are referred to the electronic PDF version (http://www.cdc.gov/mmwr) and/or the original MMWR paper copy for printable versions of official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Date last reviewed: 10/29/2008 |
|||||||||
|