|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
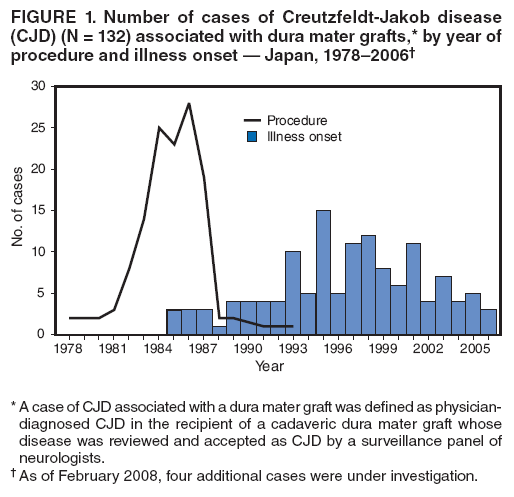
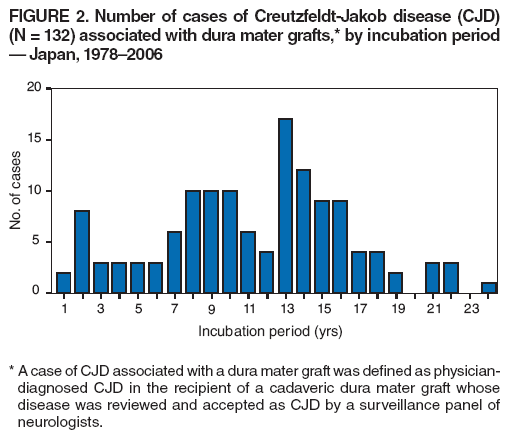
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Update: Creutzfeldt-Jakob Disease Associated with Cadaveric Dura Mater Grafts --- Japan, 1978--2008Please note: An erratum has been published for this article. To view the erratum, please click here. Creutzfeldt-Jakob disease (CJD) is the most common of the human prion diseases (also known as transmissible spongiform encephalopathies), which, according to the leading hypothesis, are caused by an abnormal protein (i.e., prion) that is able to induce abnormal folding of normal cellular prion proteins. Annual worldwide incidence of these always fatal neurodegenerative diseases is estimated at 0.5--2.0 cases per million population. CJD can occur sporadically, or as a genetic disease, or can be transmitted iatrogenically. In 1996, a new human prion disease, variant CJD (vCJD), was first described in the United Kingdom. This disease was believed to have resulted from human consumption of cattle products contaminated with the prions responsible for bovine spongiform encephalopathy (BSE, commonly known as mad cow disease). That year, in part to check for possible vCJD cases, a national survey was conducted in Japan; 821 CJD cases were identified, including 43 cases associated with receipt of cadaveric dura mater grafts (1). A single brand of dural graft (Lyodura) produced by a German manufacturer before May 1987 was identified as the most likely vehicle of transmission in all but one case (2,3). By 2003, continued surveillance in Japan had identified a total of 97 such cases (2). Since then, an additional 35 cases have been identified. This report updates previous reports and summarizes the investigation of all 132 cases to date linked to dural grafts.* The results suggest that, because of the long incubation period between graft receipt and symptom onset (possibly >24.8 years), continued surveillance in Japan might identify additional CJD cases associated with dural grafts. Since 1996, in Japan, a nongovernmental CJD surveillance group supported by the Ministry of Health and Welfare (later renamed the Ministry of Health, Labour, and Welfare) has conducted a national survey seeking cases of human prion disease. The survey is mailed to neurologic, psychiatric, and neuropathologic departments of hospitals with a minimum bed capacity of 100 (overall response rate: 74%) (1,2). A case of CJD associated with a dura mater graft is defined as physician-diagnosed CJD in the recipient of a cadaveric dura mater graft whose disease was reviewed and accepted as CJD by the surveillance system's panel of neurologists. During 1996--2008, as clinicians reported additional CJD cases to the surveillance system sponsored by the Ministry of Health and Welfare, the number of persons identified with CJD associated with cadaveric dura mater grafts increased from 43 initially to 132. All 132 patients had received dura mater grafts during 1978--1993 (Figure 1). Three patients received more than one dural graft during this period, including one patient reported previously (2,3). For purposes of analysis, the first graft was assumed to be the source of infection in all three patients. Of the 132 patients, the most common medical conditions leading to the use of dural grafts were tumor (60 patients, 45%), brain hemorrhage (21, 16%), Jannetta procedure for facial palsy (18, 14%) and for trigeminal neuralgia (seven, 5%), and intracranial aneurysm (nine, 7%). The other conditions were unspecified anomalies (six patients), hematoma (six), injury (four), and ossification of the spinal posterior longitudinal ligament (one). Illness onset for the 132 CJD patients ranged from September 1985 to October 2006 (Figure 1). The mean age of the 132 patients at onset was 55 years (range: 15--80 years); the median age was 57 years. A total of 79 (60%) patients were female. Neuropathologic confirmation of CJD diagnosis was obtained from 31 (23%) patients; 81 (80%) of the other 101 patients with physician-diagnosed CJD had an electroencephalogram with a periodic synchronous discharge pattern characteristic of CJD. Incubation periods ranged from 1.2 years (receipt in 1987 and onset in 1989) to 24.8 years (receipt in 1981 and onset in 2006) (Figure 2). The median and mean incubation periods were 12.4 years and 11.8 years, respectively. A total of 120 of the 132 patients (91%) were documented to have received Lyodura dural grafts; investigators were unable to identify the lot numbers of the grafts used. For the 12 other patients, the brand name of the dural graft was unknown. A total of 109 (83%) patients received their dural grafts during 1983--1987, when an estimated 100,000 persons received Lyodura grafts in Japan (2,4). Reported by: Y Nakamura, MD, R Uehara, MD, PhD, M Watanabe, MD, PhD, A Sadakane, MD, Dept of Public Health, Jichi Medical Univ, Shimotsuke; M Yamada, MD, Dept of Neurology, Kanazawa Univ Graduate School of Medical Science, Kanazawa; H Mizusawa, MD, Dept of Neurology, Tokyo Medical and Dental Univ School of Medicine, Tokyo, Japan. R Maddox, MPH, J Sejvar, MD, E Belay, MD, L Schonberger, MD, Div of Viral and Rickettsial Diseases, National Center for Zoonotic, Vector-Borne, and Enteric Diseases, CDC. Editorial Note:New cases of CJD associated with dural grafts continue to be reported in Japan, and Lyodura grafts remain the most likely vehicle for transmission. Similar to other allogeneic dura mater grafts, Lyodura grafts were derived from cadaveric dura mater and used by surgeons for soft-tissue reconstruction of damaged, missing, or impaired tissues (primarily dura mater). According to the manufacturer, the grafts were gradually absorbed in situ, colonized by fibroblasts and stem cells, and eventually replaced by endogenous connective tissue. In 1987, the first identified case of CJD associated with a Lyodura graft was reported in the United States (5). During the U.S. investigation of that case, the manufacturer reported revising collection and processing procedures for Lyodura to reduce the risk for CJD transmission (6). Only six of the 132 patients in Japan received their dural grafts after 1987, and only one of these six patients is known to have received a Lyodura graft that was most likely produced after 1987. This patient had received two dura mater grafts in 1991 at a hospital that reported using only Lyodura or another brand of dural grafts, Tutoplast (3). No cases have been reported in Japan among patients who received their first dural graft after 1993. The substantial number of CJD cases associated with dural grafts in Japan likely reflects the widespread use in that country of Lyodura grafts produced before May 1987. During 1983--1987, an estimated 20,000 persons in Japan received Lyodura grafts each year, approximately 50 times higher than the estimated number of recipients in the United States (2,4). Although Lyodura was then available to U.S. hospitals through the mail, the German manufacturer produced Lyodura for distribution in Japan and other countries but not for distribution in the United States (7). In June 1987, after the company learned of the first CJD case associated with a Lyodura graft, the manufacturer reported revising procedures for the collection and processing of its dura mater grafts after May 1, 1987, to reduce the risk for CJD transmission (6). The key reported processing changes included conversion from batch to individual processing of dura mater and treatment of each dura mater graft with 1.0 normal sodium hydroxide (NaOH); no practical final screening test of the product for prion contamination is available. However, the change to individual processing of dura mater greatly limited the number of grafts that could be contaminated by a single infected donor. In addition, 1.0 normal NaOH is known to be highly effective for inactivating prions (3). In the United States, after report of the first Lyodura-associated CJD case, the Food and Drug Administration (FDA) issued a recall in late April 1987 of Lyodura that was packaged in 1982, the year the graft used in the initial U.S. case had been packaged. In addition, after receiving report of a second Lyodura-associated CJD case in a patient in New Zealand, CDC advised avoiding Lyodura grafts produced before May 1987 (6). However, no international recall of Lyodura produced before May 1987 occurred. Therefore, the implicated Lyodura with its potential contaminant might have remained in use at Japanese hospitals for several years. Cases of dural graft--associated CJD in Japan have occurred since 1985, peaking during 1995--1999, when 51 of the 132 patients became ill. As this outbreak has continued, the median incubation period has increased to 12.4 years, and the longest period between graft surgery and onset of illness is now 24.8 years. In the United States, two more patients with Lyodura- associated CJD have been identified since the first reported case in 1987. Most recently, a patient aged 26 years died in 2006 from autopsy-confirmed CJD (7). The incubation period in this case was 18.7 years. The long incubation period and always fatal outcome of CJD and other transmissible spongiform encephalopathies underscore the importance of efforts to minimize potential exposures of persons to prions. However, implementing timely preventive measures against these diseases can be difficult because the public health significance of certain actions might not become apparent for years, if at all. For example, in 1987, the producer of Lyodura revised collection and production measures without knowing at the time that these actions likely would prevent many future deaths from Lyodura-associated CJD. Similarly, in 1997, a feed ban was instituted to prevent BSE in the United States, even though no endemic BSE had been recognized in North America. In addition, to prevent potential cases of vCJD in the United States, prospective blood donors who might have been exposed to BSE in the United Kingdom were deferred, even before transmission of the vCJD agent via blood transfusion had been documented in that country (8). In 1997, the FDA's Transmissible Spongiform Encephalopathy Advisory Committee recognized that use of human dura mater carries an inherent risk for transmitting CJD. However, the committee recommended that the use of such grafts be left to the discretion of the treating neurosurgeon, provided that the human dura mater is procured and processed according to additional safety measures outlined by the committee (9). After the committee's recommendations were issued, the number of dural grafts distributed for use in the United States declined from an estimated 4,500 in 1997 to an estimated 900 in 2002, to a documented 389 in 2006, and 368 in 2007 (2) (B.E. Buck, M.D., Miami Tissue Bank, personal communication, August 2008). CDC continues to conduct surveillance for cases of CJD in the United States through various mechanisms, including 1) receipt and investigation, in collaboration with local and state health departments, of case reports from physicians and patient support groups; 2) analysis of national multiple cause-of-death data; and 3) review of prion disease cases confirmed by the National Prion Disease Pathology Surveillance Center (NPDPSC) at Case Western Reserve University (Cleveland, Ohio). During 1996--1997, CDC established NPDPSC in collaboration with the American Association of Neuropathologists to help maintain and enhance U.S. human prion disease surveillance. NPDPSC provides, free of charge, advanced neuropathologic and biochemical prion disease diagnostic services to U.S. physicians and other appropriate health personnel, including local and state health officials. Patients with a rapidly progressive dementia consistent with CJD and a history of dural graft implantation should be reported through local or state health departments to CDC, telephone 404-639-3091. References
* As of February 2008, four additional cases were under investigation in Japan for suspected dural graft--associated CJD. Figure 1
All MMWR HTML versions of articles are electronic conversions from typeset documents. This conversion might result in character translation or format errors in the HTML version. Users are referred to the electronic PDF version (http://www.cdc.gov/mmwr) and/or the original MMWR paper copy for printable versions of official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Date last reviewed: 10/22/2008 |
|||||||||
|