|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
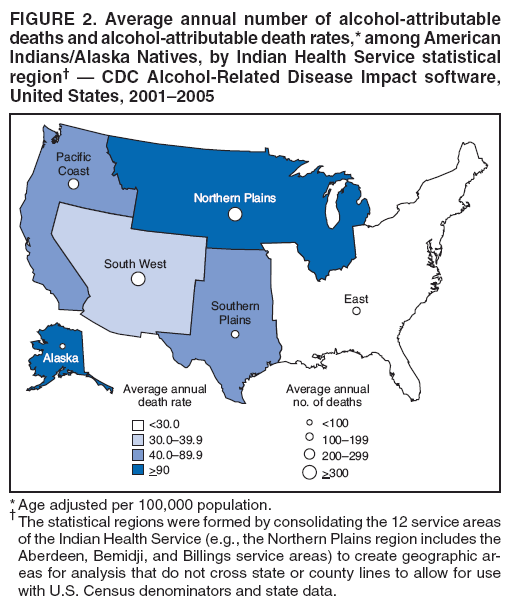
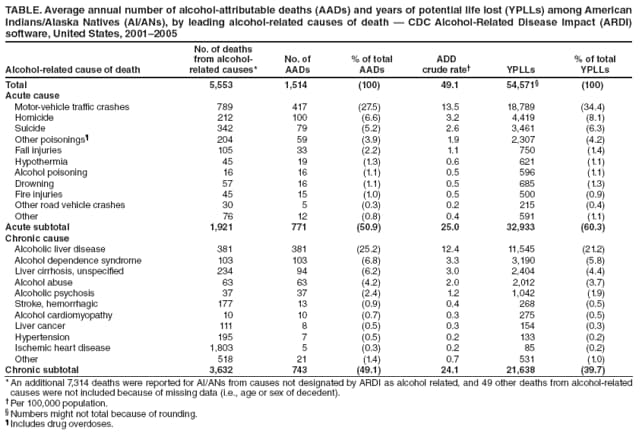
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Alcohol-Attributable Deaths and Years of Potential Life Lost Among American Indians and Alaska Natives --- United States, 2001--2005Excessive alcohol consumption is a leading preventable cause of death in the United States (1) and has substantial public health impact on American Indian and Alaska Native (AI/AN) populations (2). To estimate the average annual number of alcohol-attributable deaths (AADs) and years of potential life lost (YPLLs) among AI/ANs in the United States, CDC analyzed 2001--2005 data (the most recent data available), using death certificate data and CDC Alcohol-Related Disease Impact (ARDI) software.* This report summarizes the results of that analysis, which indicated that AADs accounted for 11.7% of all AI/AN deaths, that the age-adjusted AAD rate for AI/ANs was approximately twice that of the U.S. general population, and that AI/ANs lose 6.4 more years of potential life per AAD compared with persons in the U.S. general population (36.3 versus 29.9 years). These findings underscore the importance of implementing effective population-based interventions to prevent excessive alcohol consumption and to reduce alcohol-attributable morbidity and mortality among AI/ANs. ARDI estimates AADs and YPLLs resulting from excessive alcohol consumption by using multiple data sources and methods.† AADs are generated by multiplying the number of sex- and cause-specific deaths (e.g., liver cancer) by the sex- and cause-specific alcohol-attributable fraction (AAF) (i.e., the proportion of deaths attributable to excessive alcohol consumption). For deaths that are, by definition, 100% attributable to excessive alcohol consumption (e.g., alcoholic liver disease), the total number of AADs equals the total number of deaths. For deaths that are <100% attributable to alcohol, ARDI uses either direct or indirect AAF estimates to generate the total number of AADs. Direct AAF estimates typically come from studies that have assessed the proportion of persons dying from a particular condition (e.g., injuries) at or above a specified blood alcohol concentration (e.g., 0.10 g/dL) or from follow-up studies that have assessed alcohol use of the decedents, based on medical record review and interviews with next-of-kin. Indirect AAF estimates are calculated from pooled risk estimates obtained from meta-analyses of mostly chronic conditions, examining the relationship between various alcohol-related health outcomes (e.g., liver cancer) and the population-based prevalence of alcohol use at consumption levels (i.e., low, medium, or high). For this analysis, death certificate data for 2001--2005 were used to determine the average annual number of deaths from alcohol-related causes for all AI/ANs in the United States and for the U.S. population as a whole. Population-specific, direct AAF estimates for motor vehicle traffic crashes were obtained from the Fatality Analysis and Reporting System§ by averaging 2001--2005 data for AI/ANs and the U.S. population. Population-based prevalence estimates of alcohol consumption were obtained by averaging 2001--2005 data from the Behavioral Risk Factor Surveillance System¶ and were used to calculate all indirect AAFs. AADs were analyzed by cause and stratified by sex and by age, using standard 5-year age groupings. YPLLs were generated by multiplying the age- and sex-specific AADs by the corresponding life expectancies. Death and life expectancy data were obtained from the National Vital Statistics System.** Death records missing data on decedent age or sex were excluded from this analysis. Bridged-race population estimates from the U.S. Census were used to calculate death rates. Death rates were directly age adjusted to the standard 2000 U.S. population using the age groups 0--19, 20--34, 35--49, 50--64, and >65 years. During 2001--2005, an average of 1,514 AADs occurred annually among AI/ANs, accounting for 11.7% of all deaths in this population (Table). Overall, 771 (50.9%) of average annual AADs resulted from acute causes, and 743 (49.1%) from chronic causes. The leading acute cause of death was motor-vehicle traffic crashes (417 AADs), and the leading chronic cause was alcoholic liver disease (381). The crude AAD rate among AI/ANs was 49.1 per 100,000 population (25.0 for acute causes and 24.1 for chronic causes). Of all YPLLs, 60.3% resulted from acute conditions, and 39.7% resulted from chronic conditions. The leading acute cause of YPLLs was motor-vehicle traffic crashes (34.4% of YPLLs), and the leading chronic cause was alcoholic liver disease (21.2%). Overall, 68.3% of AAD decedents among AI/ANs were men, and more AADs occurred among men than women in all age groups (Figure 1); 65.9% of AADs were among persons aged <50 years, and 6.9% were among persons aged <20 years. Of the YPLLs, 68.3% were among those aged 20--49 years. By Indian Health Service statistical region, the greatest number of AADs occurred in the Northern Plains (497 AADs), South West (315), and Pacific Coast (230) regions, and the fewest AADs occurred in Alaska (86) (Figure 2). Age-adjusted AAD rates were highest in the Northern Plains (95.2; 95% confidence interval [CI] = 86.5--103.9), Alaska (92.6; CI = 72.4--112.8), and the South West (80.2; CI = 70.8--89.6), and were approximately four to five times higher than the rate in the East (19.2; CI = 15.8--22.6). Age-adjusted AAD rates and the relative contributions of AADs to total deaths and total YPLLs were substantially higher for AI/ANs compared with the U.S. general population. The age-adjusted AAD rate per 100,000 for AI/ANs was 55.0 (CI = 52.1--57.9) versus 26.9 (CI = 26.7--27.1) for the U.S. general population. Furthermore, AADs accounted for 11.7% of total deaths among AI/AN versus 3.3% for the U.S. general population, and alcohol-attributable YPLLs accounted for 17.3% of total YPLLs for AI/ANs and 6.3% of total YPLLs for the U.S. general population. The average number of YPLLs per AAD also was higher for AI/ANs compared with the U.S. general population (36.3 years versus 29.9 years, respectively). Reported by: TS Naimi, MD, Zuni Public Health Svc Hospital; N Cobb, MD, Div of Epidemiology; D Boyd, MDCM, National Trauma Systems, Indian Health Svc. DW Jarman, DVM, Preventive Medicine Residency and Fellowship Program; R Brewer, MD, DE Nelson, MD, J Holt, PhD, Div of Adult and Community Health, National Center for Chronic Disease Prevention and Health Promotion; D Espey, MD, Div of Cancer Prevention and Control, National Center for Chronic Disease Prevention and Health Promotion; P Snesrud, Office of Minority Health and Health Disparities; P Chavez, PhD, EIS Officer, CDC. Editorial Note:This is the first national report of AADs and YPLLs among AI/ANs; the results demonstrate that excessive alcohol consumption is a leading cause of preventable death and years of lost life in this population. During 2001--2005, AI/ANs were more than twice as likely to die from alcohol-related causes, compared with the U.S. general population; 11.7% of AI/AN deaths were attributed to alcohol. These findings are consistent with those of previous studies (4,5) and might help account for the high rates of injury-related death (e.g., motor-vehicle traffic crashes) that have been observed in this population. The finding that AAD rates vary by region demonstrates that alcohol does not impact all AI/AN communities to the same extent. AI/ANs in specific regions (e.g., Northern Plains) have lower life expectancies; this is likely attributable, in part, to deaths from alcohol-attributable conditions (6). To further address alcohol-attributable mortality among AI/ANs will require concerted action by multiple organizations and groups, including AI/AN communities, towns on nonreservation lands within and surrounding AI/AN communities, and national, state, and local health agencies. Bans on the sale and possession of alcoholic beverages on certain Indian reservations have been shown to reduce consumption and related harms (5), although the efficacy of such policies is influenced by access to alcohol in surrounding communities (7). Culturally appropriate clinical interventions for reducing excessive drinking (e.g., screening and counseling for excessive alcohol consumption and treatment for alcohol dependence) should be widely implemented among AI/ANs (7). In addition, tribal court systems, which deal with large numbers of alcohol-related crimes, should be better integrated with the health-care system and substance-abuse treatment programs. The findings in this report are subject to at least four limitations. First, some AI/ANs might have been misclassified by race on death certificates, which would underestimate the total number of AI/AN deaths (8). In a 1996 Indian Health Service study, racial misclassification on death certificates of American Indians ranged from 1.2% in Arizona to 28.0% in Oklahoma and 30.4% in California (8). Second, this study did not use race-specific AAFs for most conditions, which might result in AAD underestimates for certain conditions (e.g., homicide and suicide) for which the AAFs are thought to be higher among AI/ANs (4). Third, ARDI does not estimate AADs for several conditions (e.g., tuberculosis, pneumonia, hepatitis C, and colon cancer) for which alcohol is believed to be an important risk factor but for which suitable pooled risk estimates are not available. Finally, bridged-race census estimates used in this report are based on multiple race categories; use of denominators based on other race categorization methods (e.g., 2000 U.S. Census data or tribal census data) would result in higher rates than reported. Indian Health Service has initiated an alcohol screening and brief counseling intervention program to help reduce excessive alcohol consumption and related harms among AI/ANs in trauma settings. In addition, effective population-based interventions should be implemented to reduce excessive alcohol consumption in AI/AN populations. These include reducing alcohol availability by limiting outlet density, enforcing 21 years as the minimum legal drinking age (9), increasing alcohol excise taxes, and enforcing laws prohibiting sales to underage or already intoxicated persons, particularly in communities bordering reservations (10). Future efforts should explore regional differences in AADs and evaluate other intervention strategies for reducing alcohol-attributable mortality among AI/AN populations. Acknowledgments This report is based, in part, on data contributed by T Lindsey, National Center for Statistics and Analysis, National Highway Traffic Safety Admin, US Dept of Transportation; M Zack, Div of Adult and Community Health, National Center for Chronic Disease and Public Health Promotion; and C Rothwell and D Hoyert, National Center for Health Statistics, CDC. References
* Available at http://apps.nccd.cdc.gov/ardi. † Available at http://apps.nccd.cdc.gov/ardi/aboutardimethods.htm#aafs. § Available at http://www-fars.nhtsa.dot.gov/main/index.aspx. ¶ Available at http://www.cdc.gov/brfss/index.htm. ** Available at http://www.cdc.gov/nchs/nvss.htm.
Figure 1
All MMWR HTML versions of articles are electronic conversions from typeset documents. This conversion might result in character translation or format errors in the HTML version. Users are referred to the electronic PDF version (http://www.cdc.gov/mmwr) and/or the original MMWR paper copy for printable versions of official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Date last reviewed: 8/28/2008 |
|||||||||
|